
Abstract
Objective
To characterize the association between scholarly activity, academic rank, practice setting, and malpractice claims among otolaryngologists over the past decade.
Methods
Data was extracted from the two legal databases, WestLaw and LexisNexis. The records were obtained from January 2010 to January 2020. Scopus and PubMed databases were used to identify bibliometric data.
Results
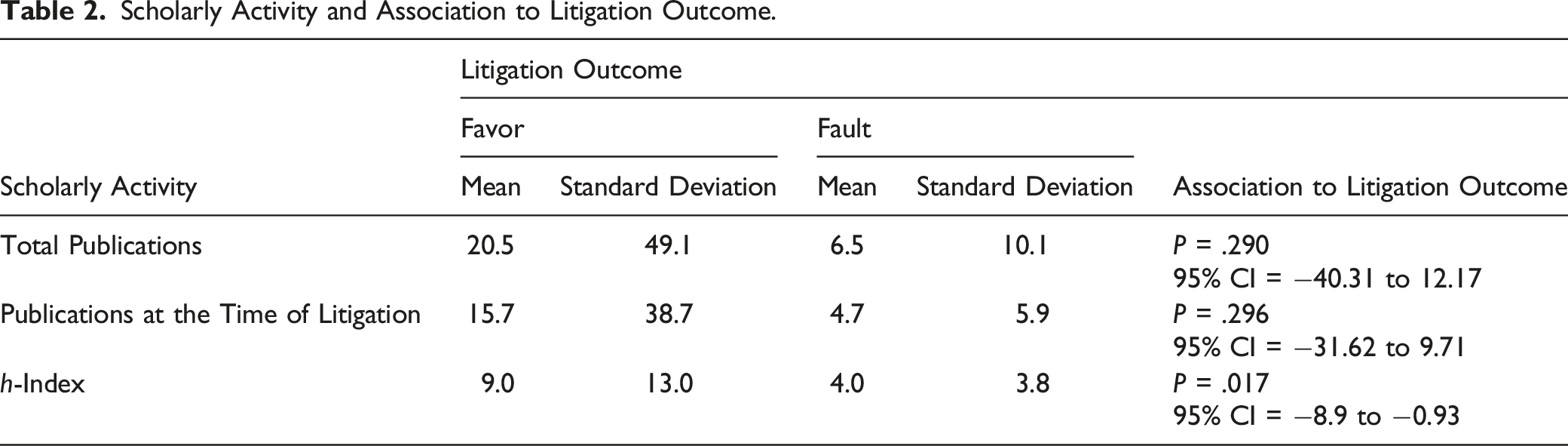
Of the 102 malpractice cases identified, 77.5% (N = 79) were ruled in favor of the defendant, 13.7% (N = 14) in favor of the plaintiff, and 8.8% (N = 9) were settled outside of the court. A total amount of $46,533,346.82 was rewarded to plaintiffs in 14 cases. Endoscopic sinus surgery was the procedure associated with the most malpractice claims (N = 16). Alleged improper performance (N = 51) was the most common underlying reason for litigation. Of the 102 defendant surgeons, 82 (80.4%) were in community/private settings. Among the 14 cases in that a surgeon was found at fault, 13 (92.8%) were in the community/private setting. Among the surgeons with at least one publication, the mean Hirsch Index (h-index) was 8.2. There was a statistically significant correlation between the mean h-index and litigation outcome (95% CI: −8.9 to −0.9, P = .017).
Conclusion
Our analysis showed that most malpractice litigations were among otolaryngologists practicing in community/private settings. We also found that higher scholarly activity measured by the h-index was associated with verdicts in favor of the defendant/surgeon. This study was limited by not all-inclusive aspects of the legal databases that were used, the small sample size, and the lack of multivariable analysis.
Introduction
Practicing defensive medicine impacts patient care and increases healthcare costs.1,2 Ideally, the legal system would allow just compensations for patients harmed by inappropriate care and drive improvements in the overall quality of care.3,4 Surgeons are particularly at high risk for potential medical malpractice claims throughout their careers. It has been reported that 7.4% of physicians in all specialties are subjected to malpractice litigation every year, and the projected career malpractice risk for general surgery and surgical subspecialties is approximately 80% by the age of 45. 5 Therefore, it is imperative for surgeons to recognize the trends in medical malpractice to manage the potential risk of litigation and further improve the quality of patient care.
The complexity of head and neck anatomy has been proposed as a major contributing factor that potentially places head and neck surgery at high risk of litigation. 6 In a study by Hong et al., 7 more than half of all otolaryngologists face at least one malpractice claim, with more than two claims per otolaryngologist on average.
Over the past decade, online platforms on scholarly activity have gained increasing popularity and made it possible to access physicians’ scholarly output. Since the introduction of the Hirsch Index (h-index) 17 years ago, the h-index has been used as a measurement tool of scholarly activity and the impact of researchers’ publications. 8 The h-index is calculated by counting the total number of publications by an author that other researchers have cited at least the same number of times (h). 9 Multiple publications have investigated the relationship of scholarly activity with funds provided by industry and the changes in scholarly activity over time among surgeons.9-11 However, the effect of scholarly activity on the frequency or outcome of medical malpractice lawsuits has not been previously studied. Furthermore, whether resident involvement in patient care affects the risk of adverse events and subsequent litigation risk remains controversial.12,13
To our knowledge, there is currently no literature on the impact of the scholarly output, academic rank, and practice setting on the litigation outcome. In this study, we aim to explore if there is an association between scholarly activity, academic rank, and practice setting with malpractice claims among otolaryngologists.
Methods
We performed a comprehensive search and extracted the data using the two main computerized legal databases: WestLaw (Thomson Reuters, St. Paul, MN) and LexisNexis (MEGA Jury Verdicts and Settlements, Dayton, OH). These databases contain detailed legal information from federal cases and all 50 states. However, these databases do not contain data on out-of-court settlements or settlements that are not made by the physician directly. This study was deemed exempt from the Institutional Review Board at the Penn State Health Milton S. Hershey Medical Center.
A Boolean search was performed using “malpractice” combined with the following search terms: otolaryngology, otolaryngologist, ENT, “Ear, Nose, and Throat”, otology/otologist, neurotology/neurotologist, laryngology/laryngologist, facial plastic surgery/surgeon, facial plastic and reconstructive surgery/surgeon, rhinology/rhinologist, head and neck surgery/surgeon, sleep surgery/surgeon, and endocrine surgery/surgeon. The data was queried in September 2020, and records from January 2010 to January 2020 were obtained. This particular period was chosen because the measurement of academic productivity with the h-index was first introduced in 2005 by Hirsch et al. and was not available for a majority of the defendant physicians until years later. 8 The initial search revealed 851 cases. Duplicates and non-relevant cases were excluded. The final data consisted of 102 jury verdicts and settlement court cases.
Data was gathered for all alleged litigation claims related to otolaryngologists and otolaryngology subspecialists. Each malpractice claim was reviewed for case year, surgeon’s specialty/subspecialty, defendant institution type, the reason for the lawsuit, requested malpractice claim, paid malpractice claim, defendant professorship status (if applicable), total number of publications, total number of publications at the time of litigation, defendant’s h-index at the time of litigation, and verdict.
Bibliometric Data
The Scopus database (www.scopus.com; Elsevier, Amsterdam, Netherlands) was used to extract bibliometric data for each defendant otolaryngologist. The extracted bibliometric data included the total number of publications, the number of publications at the time of litigation, and the h-index. If the Scopus search did not reveal any results, the PubMed database was explored using each physician’s first and last name. The physician’s middle name and affiliated institution were used if the investigation was inconclusive. We also performed a search using the google search engine and the Doximity website (www.doximity.com; Doximity Inc, San Fransisco, CA) to identify physicians’ practice settings and related academic rank.
Litigation Cause Classifications
The underlying cause for litigation was classified into six categories: Failure of informed consent, misdiagnosis or delayed diagnosis, alleged improper performance or treatment, postoperative complications, improper disposition, and negligence in care. The failure of informed consent is defined as a failure to provide adequate information or provision of misinformation about the disease process, risks of surgery, and postoperative complications pre-operatively. 14 Misdiagnosis or delayed diagnosis is when the patient’s condition or injury progressed beyond where it usually would have due to inappropriate or delayed diagnosis. Improper disposition is the inappropriate timing or location of a patient’s discharge, level of care, or transfer.
Statistical Assessment
IBM SPSS Version 22 (IBM Corp. Armonk, NY) and Microsoft Excel (Microsoft Corporation, Redmond, WA) were used for data analysis. An independent t-test was used to determine the differences in means for the two groups. Chi-square, Fisher’s exact test, was performed to compare categorical variables, and analysis of variance (ANOVA) was performed to compare the means of three or more groups. We completed the Kruskal–Wallis test for non-normally distributed data when appropriate.
Results
Demographic Data
From 2010 to 2020, 102 malpractice cases in the otolaryngology field and otolaryngology subspecialties were identified. Of the 102 cases, 77.5% (N = 79) were ruled in favor of the defendant, 13.7% (N = 14) in favor of the plaintiff, and 8.8% (N = 9) were settled outside of the court. A total amount of $46,533,346.82 was rewarded to plaintiffs in 14 cases. The mean amount of paid malpractice claim was $3,323,810.48 ± $4,956,062.86 (range, $150,000.00–$15,349,014.10) and median was $1,122,100.00. The malpractice claims were filed in 27 states. New York had the highest number of malpractice claims (N = 24), followed by California (N = 12) and Michigan (N = 8, Figure 1). Distribution of malpractice claims among states. New York (N = 24) had the highest number of malpractice claims, followed by California (N = 12), Michigan (N = 8), Indiana (N = 7), and New Jersey (N = 5).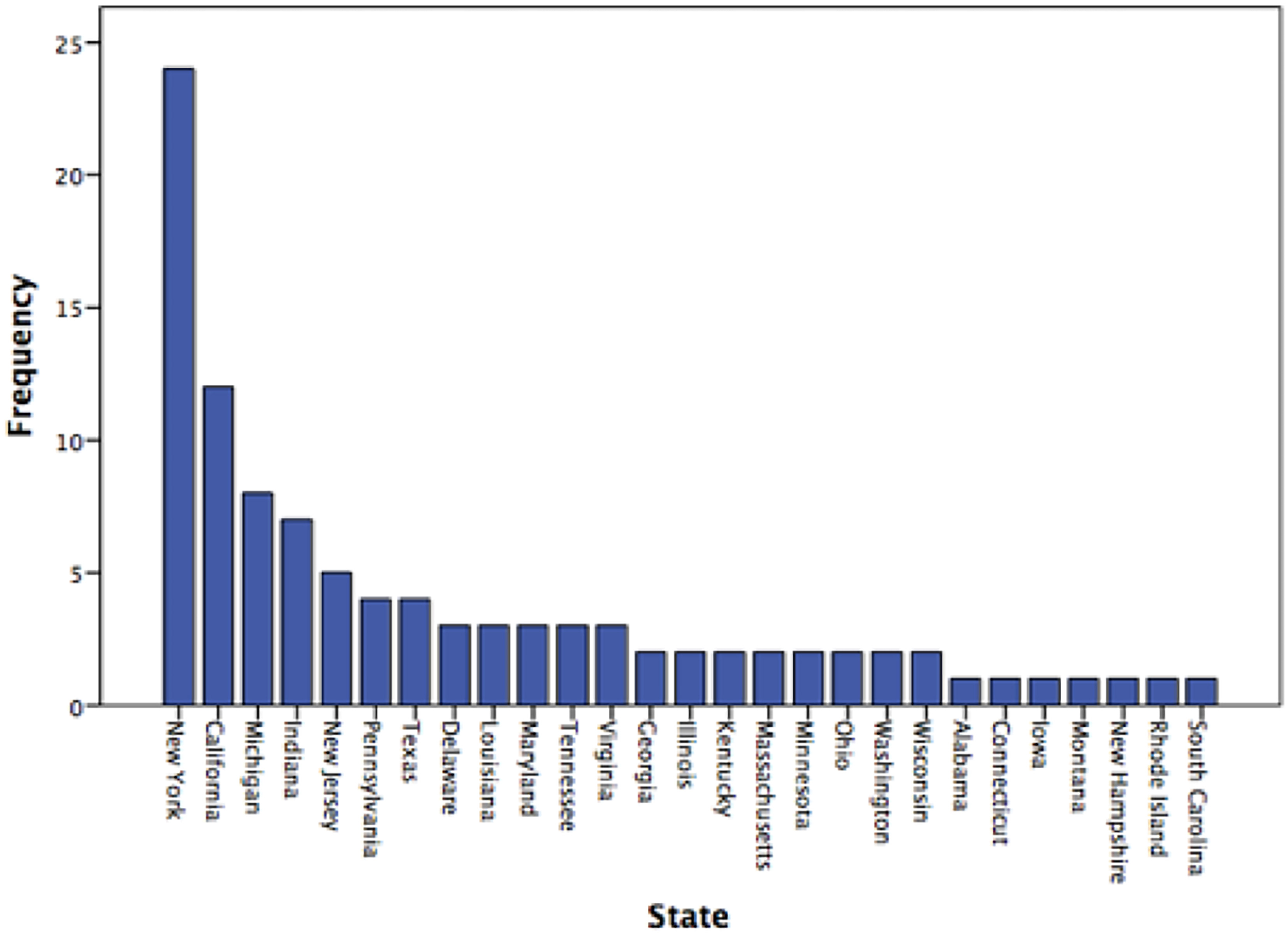
Malpractice Claims Categories and Causes
Comparison of Case Characteristics Among Reasons for Litigation.
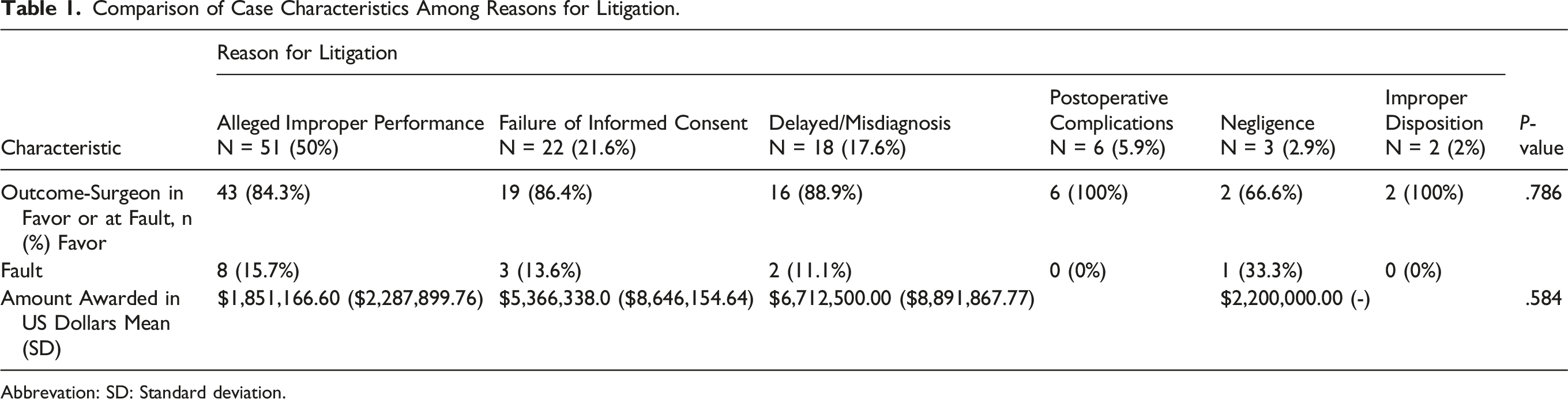
Abbrevation: SD: Standard deviation.
The claims were classified into seven categories based on the type of procedure. Head and neck oncology constituted the largest number of malpractice claims (N = 37), followed by rhinology (N = 24, Figure 2). Two claims were not related to otolaryngology procedures, but the otolaryngologist was sued. The most common procedures that led to malpractice claims were endoscopic sinus surgery (N = 16), parotidectomy (N = 9), thyroidectomy (N = 8), and tonsillectomy (N = 7). Among 16 endoscopic sinus surgeries that lead to malpractice claims, 15 were performed by general otolaryngologists, and a fellowship-trained rhinologist performed one. Distribution of the case categories and malpractice claims. Head and neck oncology (N = 37), rhinology (N = 24), otology/neurotology (N = 17), facial plastic and reconstructive surgery (N = 10), pediatrics (N = 9), dental (N = 2), laryngology (N = 1). FPRS: Facial Plastic and Reconstructive Surgery.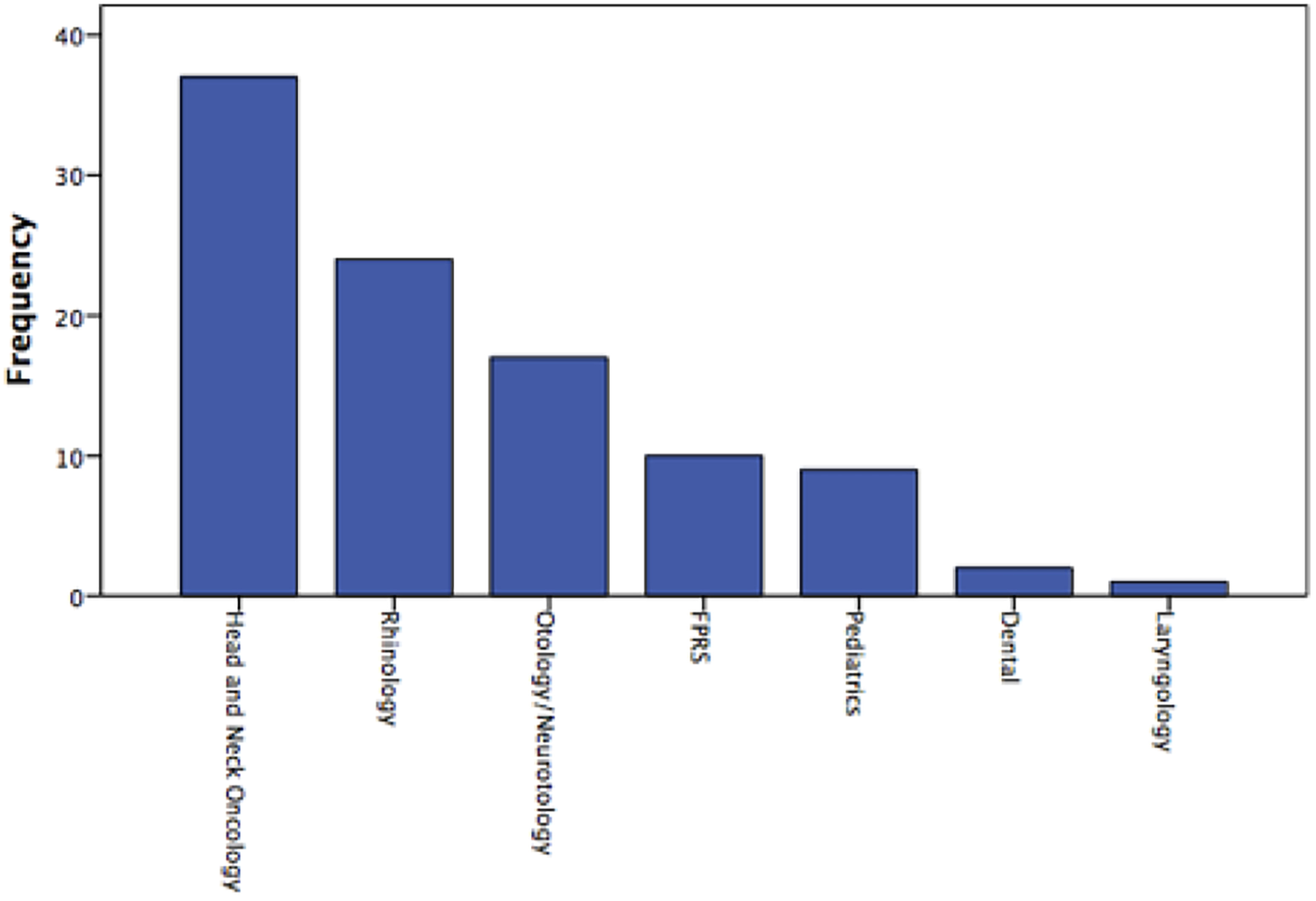
Practice Setting, Scholarly Activity, and Malpractice Claims
Of the 102 defendant surgeons, 20 (19.6%) were faculty at an academic institute versus 82 (80.4%) community/private. Among the 14 cases in that, a surgeon was found at fault and 13 (92.8%) were in the community/private setting. Of the 20 academic faculty sued, 11 (55%) were full professors, three (15%) associate professors, and six (30%) assistant professors. There was a statistically significant association in litigation outcome among the three academic ranks (95% CI: 1.85 to 2.5, P = .049).
Scholarly Activity and Association to Litigation Outcome.
Discussion
Practice Setting
In our study, academic surgeons constituted less than 20% of the litigation cases. According to the 2017 American Academy of Otolaryngology-Head and Neck Surgery (AAO-HNS) Socioeconomic Survey, an estimated 30% of otolaryngologists work in academic practice, and 70% work in a community-type setting, which may explain why most litigated otolaryngologists were in a community or private-practice setting. 15 The lower reported rate of litigations in academic settings is also attributable to several other factors. A higher volume of encounters and greater procedure-specific volume in academic institutes as well as community/private practices with robust patient volume may be associated with improved quality of care and lower risk of litigation. Additionally, the available resources in academic institutions for adverse events that are focused on communication and resolution models may be a protective factor against the potential risk of litigation. Other protective factors include greater financial funds and dedicated defending attorneys or law firms in large academic institutions against malpractice claims than private/community practices. In a study by Minnicuci and Bryan, 16 authors investigated medical education litigation over a decade. They found that institutional defendants are more likely to settle malpractice lawsuits early and outside the court, specifically if the litigation results in negative publicity.
While the abovementioned elements might reduce malpractice claims in large academic centers, otolaryngologists working in academic institutions are not immune from malpractice litigations. The attendance of surgical and medical trainees can potentially pose a liability risk and subsequent risk of litigation to attending surgeons. 17 Thiels et al. 12 evaluated medical malpractice litigations against surgical trainees over ten years. The authors identified 87 malpractice claims involving surgical residents, and only in five cases, the supervising attending was not cited as a defendant. In ten cases, the attending surgeon was litigated because of a lack of supervision over the trainee, and in all ten patients, the supervising surgeon was found at fault. That being said, there are undeniable advantages to working with trainees and residents including greater availability to address patients’ acute needs, promoting current and up-to-date medical knowledge, and providing an extra pair of eyes in the care of patients that may reduce the risk of error and subsequent potential for litigation.
Scholarly Activity
Scholarly output in the form of research is integral in determining appointment and promotion within academic medicine. Its utility has been evaluated in various disciplines within medical specialties and has shown to increase with rising academic rank.18,19 In our sample group, in addition to a significantly higher h-index among academic surgeons (Mean = 19) versus community/private (Mean = 3), there was a statistically significant association between a higher h-index and favorable litigation outcome. It is conceivable that the higher scholarly output might be associated with a lower risk of malpractice litigation due to any of several factors, including reduced time spent in direct patient care, perceived stature of a prolific clinician, or increased awareness of evidence-based guidelines. Higher scholarly output among academic faculty may keep them more up-to-date on current practice standards, innovations, and new surgical techniques, thus allowing for improved patient outcomes. Another factor to consider is that although there are high-volume clinicians who are also extremely productive in academics, the h-index may partially be a proxy for the time away from patients and lower clinical volume that may account for the lower number of malpractice claims.
Surgeons with higher academic ranks potentially have a greater experience in the field that is not only related to surgical performance but also associated with recognizing and mitigating factors that may result in malpractice claims. This can range from patient communication to obtaining thorough and timely informed consent. Another important factor to consider is the experience gained by physicians serving as expert witnesses in malpractice trials. It has been shown that testifying physicians who were qualified as expert witnesses for either side were vastly experienced with high scholarly output and primarily served in academic institutes.20,21 This expertise among surgeons with higher academic ranks can help recognize and alleviate the risk factors for litigation.
Underlying Reason for Litigation
Over the past decade, the present analysis of malpractice cases demonstrates similar litigation trends as previous studies within the otolaryngology field. Similar to the study by Tolisano et al., 22 endoscopic sinus surgery was the most common procedure that led to litigation. We also found that allegations of improper performance continue to be the most common underlying reason for malpractice claims, and failure of informed consent continues to be a significant contributor to the litigation landscape among otolaryngologists.8,23,24 The information provided by studying malpractice claims are best employed to provide an understanding of factors resulting in legal allegations and to provide means to reduce the potential risk of litigation.
Limitations
A limitation of our study was the retrospective nature and possible inaccuracies in the online databases used to identify physicians and their affiliated scholarly output. This study is also limited by the not all-inclusive aspects of the legal databases (LexisNexis and WestLaw) used. These two major legal databases do not include the cases settled outside the court and rely on private jury verdicts. When compared to National Practitioner Data Bank (NPDB), the available data in WestLaw and LexisNexis is found to be underrepresented. 25 Unlike WestLaw and LexisNexis, NPDB relies on hospitals, state licensing boards, and medical malpractice insurance companies to report all malpractice payments that are paid on behalf of a physician, providing more comprehensive data on settlements and judgments.25,26 As a result, the small sample size presented in this study may not represent the entire otolaryngology specialty. Also, several confounding factors such as the geographical location of the practice, type of community (urban, suburban, and rural), states with Tort reform versus states without, and the patient volume were not considered in the analysis. Further studies with multivariable models are required to account for these variables.
Conclusion
Our analysis showed that most malpractice litigations were among otolaryngologists practicing in community/practice settings. Although a higher number of court cases and settlements were noted in private practice, it is unclear based on the available data if this is due to surgeon experience (e.g., a higher number of cases done at academic institutions), settlement strategies, or other underlying reasons. We found that higher scholarly activity measured by the h-index was associated with verdicts in favor of the defendant/surgeon. The clinical significance of this finding is unknown and cannot be extrapolated based on the currently available data. Further research is needed to identify the risk stratification of litigation in otolaryngology based on surgeon experience, number of cases overall (settled outside of the court in addition to those proceeding to court), number of years in practice, and if the scholarly status has a true association with eventual litigation outcomes.
Footnotes
Authors’ Note
This paper was an oral presentation at the AAO-HNSF October 2021 Annual Meeting & OTO Experience.
Authors’ Contributions
K. Z.: Study concept and design; acquisition, Analysis, or interpretation of data; drafting of the manuscript; Statistical analysis; Administrative, technical, or material support. S. P.: Acquisition, analysis, or interpretation of data; Drafting of the manuscript. M. C.: Acquisition, analysis, or interpretation of data; Drafting of the manuscript. R. S.: Study concept and design; Drafting of the manuscript. D. G.: Drafting of the manuscript; Critical revision of the manuscript for important intellectual content. J. G. L.: Study concept and design; Drafting of the manuscript; Critical revision of the manuscript for important intellectual; Administrative, technical, or material support; Study supervision.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The authors confirm that we have read the Journal’s position on issues involved in ethical publication and affirm that this report is consistent with those guidelines.
Data Availability
All authors had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. The data is available to anyone for review upon request.