
Abstract
Background
The prognostic factors for tumor recurrence and mortality of patients diagnosed with Papillary Thyroid Carcinoma (PTC) with immediate surgery in Colombia has not been reported.
Objective
To retrospectively evaluate the risk factors for recurrence and survival at 10 years in patients with the diagnosis of PTC treated at Fundación Santa Fe deBogota (FSFB).
Methods
A total of 486 patients with thyroid surgery accompanied by medical follow-up were recruited. Demographic, clinical, and pathological variables were followed-up for a median period of 10 years.
Results
The most significant variables for recurrence were tumors with > 4 cm of size (hazard ratio [HR] = 8.1; 95% confidence interval [CI] = 1.7–55) and extrathyroidal spread (HR = 26.7; 95% CI = 3.1–228).
Conclusion
PTC in our population has low rates of mortality (0.6%) and recurrence (9.6%), with an average time of recurrence of 3 years. Size of the lesion, positive surgical margins, extrathyroidal spread, and high postoperative serum thyroglobulin (Tg) level act as prognostic factors that determine the likelihood of recurrence. Unlike other studies, the influence of age and gender does not act as a prognostic factor.
Introduction
The survival rate for patients diagnosed with PTC has been relatively stable for more than 20 years, with an overall survival rate of 80% to 98%.1–9 The treatment is heterogeneous and risk-dependent, including active surveillance, lobectomy/total thyroidectomy, neck dissection, radioactive Iodine-131 (RAI), and thyroid-stimulating hormone (TSH) suppression therapy; therefore, minimizing the risk of disease recurrence and metastatic spread. Tyrosine kinase inhibitor should be considered for iodine-resistant disease associated with large and advanced tumors.10–13
In general, between 5% and 27% of cases develop local,14–19 regional, or remote extension, indicating the presence of more aggressive forms of the disease and histopathological features that define their prognosis.20–23 Approximately, 60% to 75% of the cases of recurrence are in cervical lymph nodes, whereas 20% occurred in the thyroid bed, and the other 5% of the recurrences are in the trachea and muscles. 15 This behavior can worsen the prognosis of the disease and increase the risk of death.16,24,25 PTC is responsible for 70% of all deaths from thyroid cancer. 26 Staging systems have been created to identify patients with a moderate and high risk of recurrence and death based on a very heterogeneous population, such as AMES, 27 AGES, 28 MACIS, 29 DAMES, 30 GAMES, 31 TNM, 32 and others; not allowing adequate local risk stratification. Factors such as sex, age, histopathology features, soft tissue compromise, type and extent of surgery, and the administration of RAI have been analyzed.5,7,8,16,20–23,33,34 The aim of this study was to retrospectively assess the prognostic factors associated with recurrence and survival at 10 years of 486 patients treated at Fundación Santa Fe deBogota (FSFB) with PTC. In Colombia, we do not have studies that evaluate the prognostic factors of immediate surgery, and the information on the Latin American countries is scarce.
Material and methods
Patients and tumors
A retrospective medical record review of prognostic factors from a total of 2100 patients, who underwent thyroidectomy for PTC treated by just one surgeon in the head and neck surgery department of FSFB from 1993 to 2011 was conducted, when active surveillance and overtreatment remain unclear; after 2015 more conservative management strategies has been implemented. 10 Of these, 486 patients met all inclusion review criteria and were included in the study. The patients with benign pathology, nonadenocarcinoma histology (such as squamous, medullary, or anaplastic), with clinical records outside FSFB, surgical treatment in other institutions, and those who could not be followed-up during the established time were not included. The diagnosed patients who were included in this study presented a finding of thyroid nodules or nodules on physical examination or as an incidental finding during imaging studies for another reason.
All patients underwent total or subtotal thyroidectomy with or without neck dissection and, when it was indicated, administration of RAI. The primary tumor was classified according to the 8th edition of the American Joint Committee on Cancer, TNM classification of malignant tumors. 32 The histologic variants of PTC were grouped into 7 groups: usual/classic, follicular, tall cell, diffuse sclerosing, poorly differentiated, columnar cells, and others. In cases where patients had more than one subtype of variants, they were classified according to the most aggressive category.
Treatment and follow-up
The treatment for patients with PTC was total or subtotal thyroidectomy and neck dissection in cases where lymphadenopathy was identified. In all patients with tumors larger than 1 cm, with involvement of lymph nodes, extrathyroidal extension, and metastasis, RAI was performed. Patients were prepared with a low iodine diet and/or administration of recombinant TSH (Thyrogen®), for the administration of RAI. Doses range from 30 to 150 mCi according to the stratification criteria risk and the nuclear medicine department. All patients received levothyroxine to maintain TSH levels below 0.2 mIU/L and calcium with vitamin D when needed. Some patients with aggressive forms of the disease, extrathyroidal extension, and microscopic residual tumors received postoperative radiation therapy in the neck. After treatment, the patients were monitored with measurements of thyroglobulin (Tg) and thyroglobulin antibodies (TgAb) at least every 6 months, and a neck ultrasound (NUS) was requested at least every 6–12 months if the patient had Tg under suppression above 2 ng/ml. [18F] 2-fluoro-2-deoxy-D-glucose-positron emission tomography-computed tomography was made for patients with rising serum Tg and negative whole-body RAI scan (WBRS). Disease-free status was defined with the following criteria: (1) no clinical evidence of tumor, (2) no imagenological evidence of tumor, (3) Tg undetectable under suppression or less than 2 ng/ml with TSH released, and (4) negative TgAb. 35
Recurrence
A high risk of recurrence was indicated by values of Tg under suppression greater than or equal to 2-ng/ml. This data was correlated with NUS, computerized tomography scan, and WBRS. Recurrences were confirmed with biopsy as suitable. For cases of lung and brain metastasis, radiological images were considered sufficient.
Statistical analysis
All clinical, radiological, pathological, treatment, and follow-up data were collected from medical records in a central database. To evaluate the final stage of the disease, living or dead, illness or disease-free status, telephone contact was performed with all patients.
Data were analyzed using SPSS version 19.0 (Armonk, NY, IBM Corp) and the EPIDAT 3.1 program (Software for Epidemiologic Analysis of Tabulated Data; http://dxsp.sergas.es). The Kolmogorov–Smirnov test was used to assess the normal distribution of data. Continuous data with normal distribution are expressed as a mean and standard deviation; otherwise, data are expressed as the median with the interquartile range. The student’s t-test for unpaired data and Mann–Whitney U test were used to analyze the normal and nonnormal distribution of continuous variables, respectively. Categorical data are expressed as a percentage. Fisher’s exact and chi-square tests were used to analyze categorical variables.
Survival time distributions until recurrence were estimated using the Kaplan+Meier method and log-rank test. Multivariate statistical analyses were performed having as outcome recurrence for variables that presented P < 0.2 and/or were previously reported in the literature to be significant using the Cox proportional hazards regression model.
Ethical component
This study was conducted with the approval of the Corporate Ethics Committee of FSFB.
Results
Of the 486 patients with PTC, 83% of patients were women, 44% being younger than 45 years (age range: 13–79 years). In 65% of the cases, the PTC diagnosis was asymptomatic and found incidentally on neck ultrasound requested by other causes. 25% of patients consulted for thyroid mass, 4.9% for dysphagia, 4.5% for dysphonia, and 2.6% for obstructive dyspnea. Three patients had external beam radiotherapy on the neck (in an inoperable macroscopic tumor where the risk/benefit was unfavorable, associated with an aggressive histology); 2% of patients had a diagnosis of thyroiditis associated before surgery. 6.1% of patients had a first-degree relative with PTC. One patient had multiple endocrine neoplasia 2A incidentally coexisting with medullary thyroid carcinoma, which has been reported rarely. 36
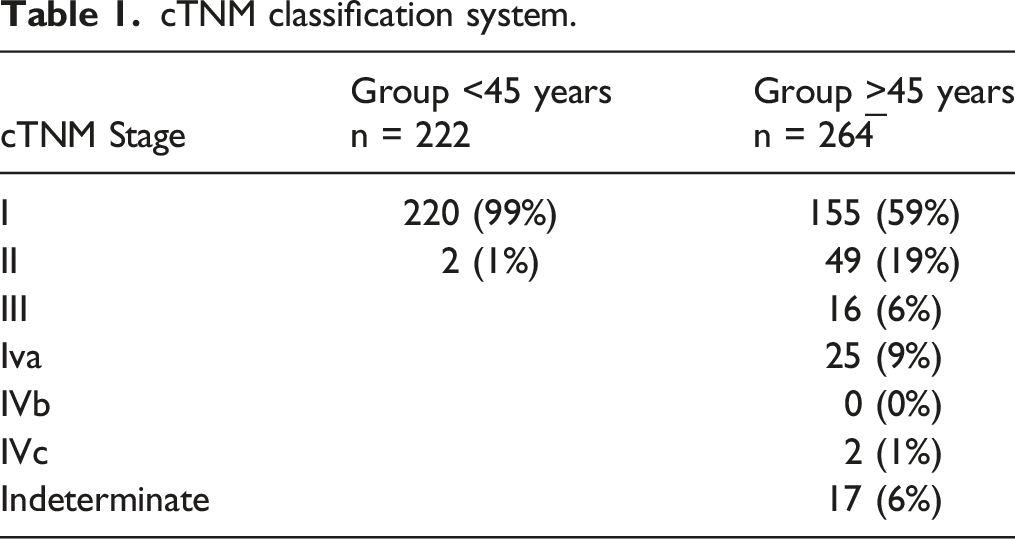
In the preoperative evaluation, 77% of the patients had a palpable nodule; in 33% of cases the nodule was larger than 2 cm, and 13% had palpable lymphadenopathy in one or more areas of the neck (zone III was the most common), 2% had extrathyroidal muscles and nerve involvement; and finally, 4 patients had lung metastases.
cTNM classification system.
Total thyroidectomy was carried out in 436 patients (89.7%), a lobectomy in 50 patients (10.3%), and central lymph node dissection in 282 patients (58%): modified radical neck dissection in 74 patients (26.2%), mediastinal dissection in 94 patients (33.3%), and paratracheal dissection in 217 patients (76.9%). Unilateral neck dissection was done for 80.2% of patients and bilateral neck dissection in 19.2% of the patients. 67% of patients present a carcinoma less than 2 cm in size and of these patients, 30% were found to have the extrathyroidal extension: 89% of these to the prethyroid muscles, 13% to the recurrent laryngeal nerve, 7% to the trachea, and 5% to the tracheoesophageal groove.
The most common postoperative complication was hypoparathyroidism in 22% of cases; 98% of cases of hypoparathyroidism were transient. 37 cases of dysphonia, 3 hematomas, 5 local infections, and 1 pulmonary embolism occurred. There was no operative mortality.
Clinicopathologic characteristics of the patients with thyroid carcinoma with or without recurrence.
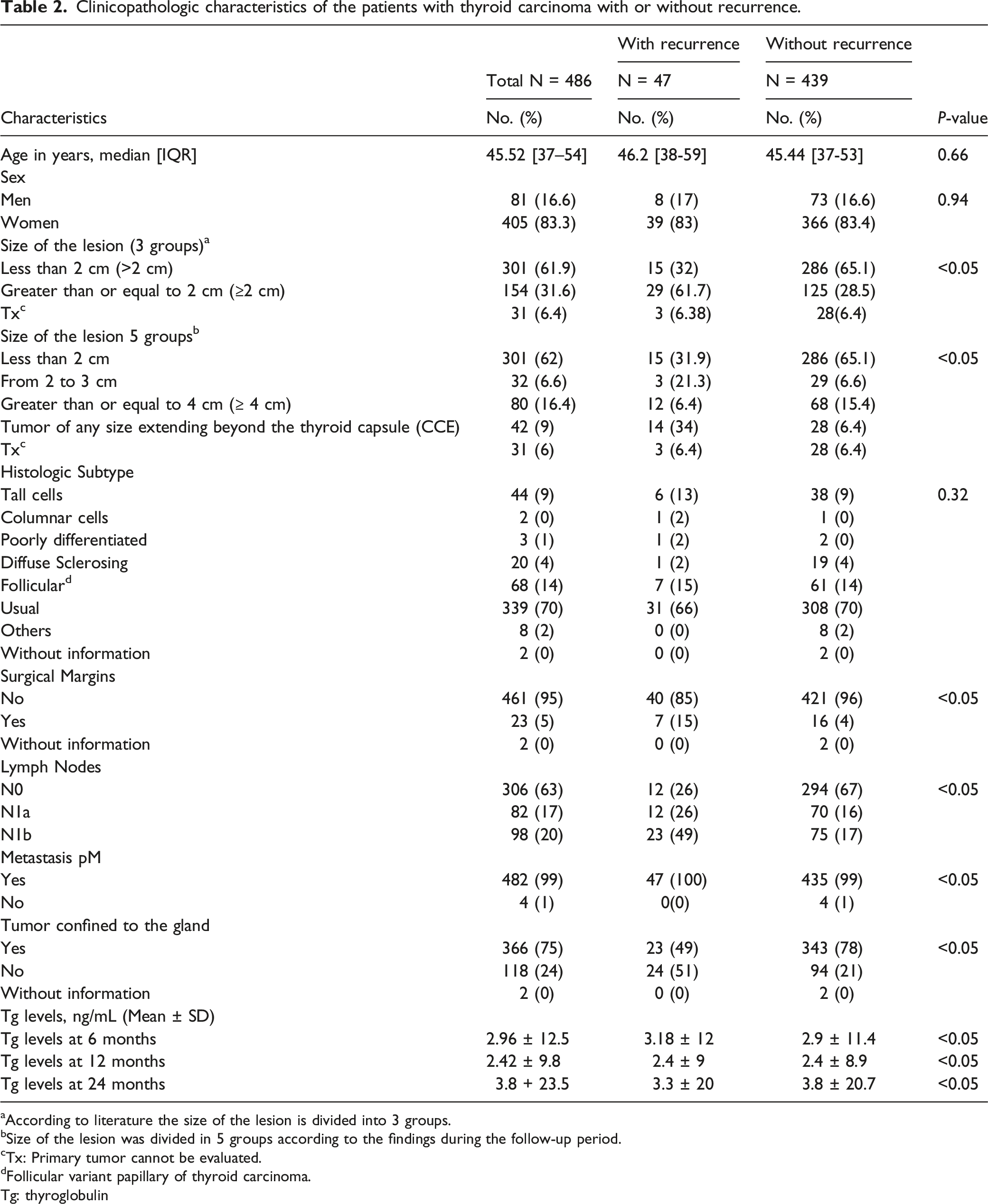
aAccording to literature the size of the lesion is divided into 3 groups.
bSize of the lesion was divided in 5 groups according to the findings during the follow-up period.
cTx: Primary tumor cannot be evaluated.
dFollicular variant papillary of thyroid carcinoma.
Tg: thyroglobulin
Application of the pTNM system resulted in the assignment of 60% of the cases to pT1, and 8% to pT4. 62% belonged to pTN0, 16.9% to N1a, and 20.2% to N1b. RAI was administered to 70% of patients, 35.8% receiving over 100 mCi, and 46.4% receiving less than 100 mCi. External radiotherapy in the neck was administered to 14 patients.
Recurrence
Of 486 patients that were evaluated periodically with serum Tg, TgAb and images, 90.3% had no recurrence. Clinical recurrence occurred in 40 patients (10%). Of those, 36 patients had a recurrence in regional lymph nodes, 1 in the trachea, 7 cases in the lung, and 1 had bone metastases. 45% of patients with recurrence confirmed by biopsy had high Tg levels, whereas 37.5% of patients with recurrence had normal Tg levels. The remaining 7 patients with metastases were not controlled with Tg. Half of the patients who had a recurrence in lymphadenopathy had it in zone VI and VII (22 patients). At the end of the study, 7 deaths occurred, and 3 cases were related to PTC One patient died with involvement of the trachea. 4 other cases were by undetermined causes.
Association analysis
Based on the univariate analysis and the association of variables related to prognosis according to the literature, it was found that the variables age and sex were not statistically significant, whereas tumor size, lymph node involvement, and the tumor was confined to the gland without extrathyroidal extension, were statistically significant (Table 2).
Progression-free survival analysis
In the follow up period, patients who underwent surgery presented a median survival of 19.5 years as at 20 years 98.5% were alive. Lesion size was classified into 5 groups: (1) less than 2 cm, (2) from 2 to 3 cm, (3) greater than or equal to 4 cm, (4) tumor of any size extending beyond the thyroid capsule, and (5) primary tumors which could not be measured. The probability of relapse is higher as tumor size increases. Also, patients with positive lymph nodes (N1a and N1b) have a higher local risk of recurrence. RAI treatment and high levels of serum Tg had an overall effect on recurrence. Patients who received RAI had a greater probability of recurrence compared with patients who do not receive treatment, this may be possible by the presence of neoplastic involvement at diagnosis (P = 0.001). Moreover, the Tg levels tend to increase over time after surgery, which enhances the ability to predict the likelihood of recurrence with a higher probability when it is above 2 ng/mL at 6 and 12 months after surgery (Figure 1). (A) Tumor sizes were classified into 5 groups: less than 2 cm (<2 cm), 2 cm to 3 cm, greater than 4 cm (>4 cm), tumor of any size extending beyond the thyroid capsule (CCE), and primary tumor cannot be evaluated (Tx). (B) Risk of recurrence according to lymphatic commitment. (N0): No regional lymph node metastasis; (N1a): Metastasis to the lymph nodes around the thyroid, (N1b): Metastases to unilateral, bilateral or contralateral cervical or retropharyngeal or superior mediastinal lymph nodes. (C) Risk of recurrence according to indication for radioactive iodine therapy (I-131). 0: No treatment. 1: ablation with iodine 131. (D) Risk of recurrence according to TG serum levels after 12 months of surgery.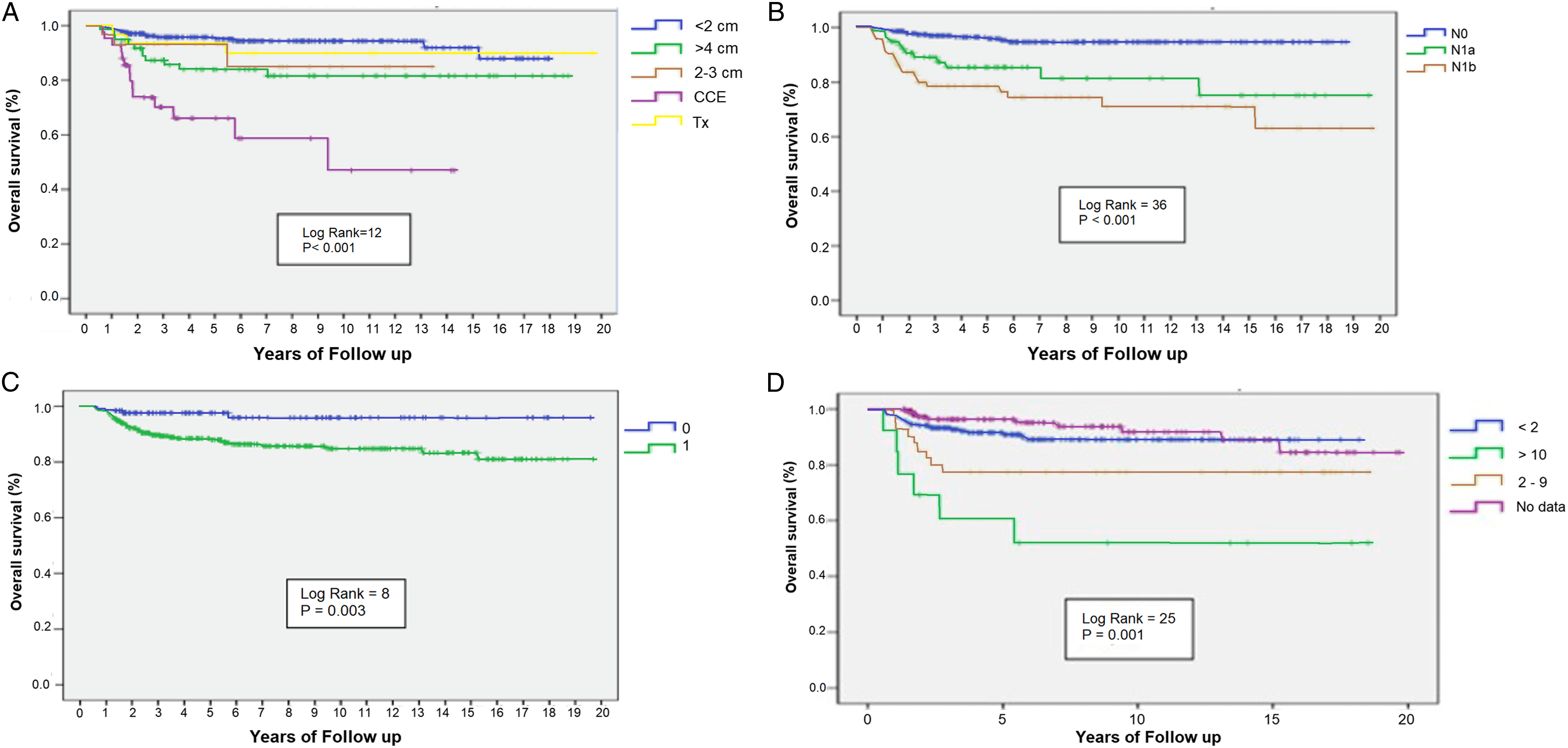
At the end of the follow-up period, having a multifocal pathology at the time of diagnosis had no overall effect on disease recurrence. 51% of the patients with a multifocal pathology had recurrence; however, this difference is not statistically significant (P = 0.421). Concerning the other clinicopathological variables, we found that patients with undifferentiated TC, with the presence of surgical margins after surgery, with a tumor not confined to the thyroid gland, and distant metastases, are more likely to relapse and have a smaller survival percentage. The probability of remaining in remission at 10 years is 83% when the local disease is present. No significant difference was found in survival rates between men and women with a Log Rank (Mantel-Cox) of 0.02, and a P-value of 0.96 for survival in stage T1.
During follow-up, 1.4% of patients with TC died. 6 of the 7 patients were women and had RAI as a treatment after surgery. The age range at the time of diagnosis was from 18 to 67 years and patients had a follow-up period from 1 to 18 years after surgery. 71% of the patients had the usual histological subtype and not multifocal pathology at the time of diagnosis. Of these patients, 42% died due to PTC with Tg levels at a recurrence of 19, 43, and 300 ng/mL. At diagnosis, the size of the lesion was 2 and 5 cm. One of the patients had the tumor confined to the gland and 2 patients were classified in the tumor of any size extending beyond the thyroid capsule (CCE) group.
Multivariate data analysis
Prognostic factors for recurrence.
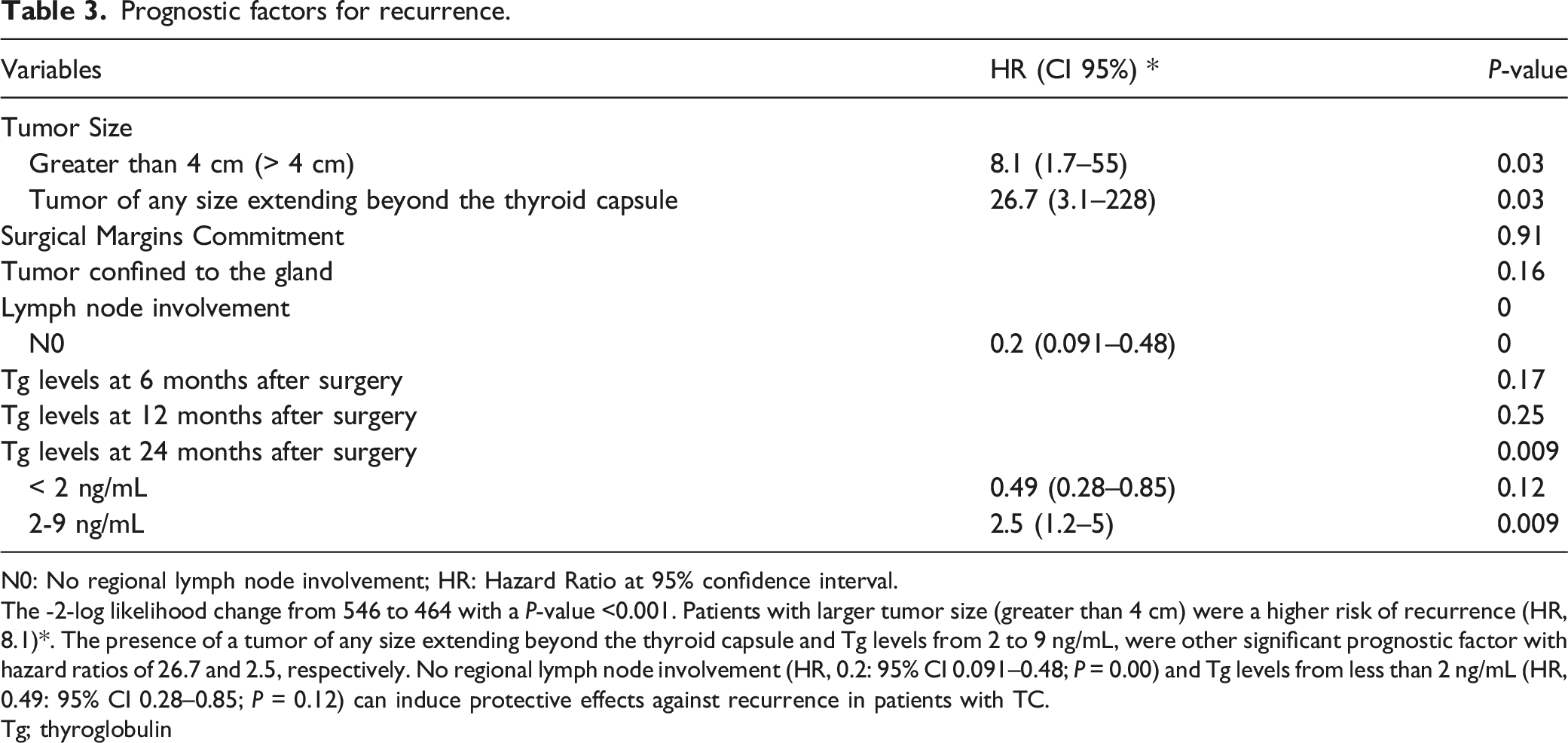
N0: No regional lymph node involvement; HR: Hazard Ratio at 95% confidence interval.
The -2-log likelihood change from 546 to 464 with a P-value <0.001. Patients with larger tumor size (greater than 4 cm) were a higher risk of recurrence (HR, 8.1)*. The presence of a tumor of any size extending beyond the thyroid capsule and Tg levels from 2 to 9 ng/mL, were other significant prognostic factor with hazard ratios of 26.7 and 2.5, respectively. No regional lymph node involvement (HR, 0.2: 95% CI 0.091–0.48; P = 0.00) and Tg levels from less than 2 ng/mL (HR, 0.49: 95% CI 0.28–0.85; P = 0.12) can induce protective effects against recurrence in patients with TC.
Tg; thyroglobulin
Discussion
This study analyzed patients with immediate surgery for PTC at a time when active surveillance and overtreatment were unclear. The prognostic factors that have been identified in many retrospective studies are age at diagnosis, sex, extent, and size of the primary tumor, lymph node metastases, a distance of metastases, histology, an extension of the primary surgical procedure, and RAI.16,20–23 Age at diagnosis and sex are important variables to assess the prognosis; however, no statistically significant differences were found between these variables and recurrence in patients with PTC in our study. Also, it was found that measuring the size of the lesion is best performed by stratification in 5 groups as follows: Less than 2 cm, from 2 to 3 cm, greater than or equal to 4 cm, tumor of any size extending beyond the thyroid capsule (CCE), and primary tumor cannot be evaluated (Tx). Most of the recurrences were found in the first and last category, determined with 15 and 16 patients, respectively. In literature, the size of the lesion is classified only in two groups: less than 2 cm and greater than or equal to 2 cm, leaving out other size categories that can produce a different prognosis. In our population, tumors larger than 4 cm and tumors of any size with extrathyroidal extension are prognostic factors for recurrence. In contrast, not having regional lymph node metastasis and maintaining Tg levels below 2 ng/mL as time passes after surgery, act as protective factors. Lack of surgical margins and a primary tumor limited to the thyroid gland were not statistically significant in the hypothesis testing and therefore were not used for the multivariate analysis. Additionally, it was identified that postoperative Tg levels of 2 to 9 ng/mL under TSH suppression may be a prognostic factor for recurrence.
Currently, it has been demonstrated, in numerous case series studies, an association between a poor clinical outcome and age at diagnosis, histological type, tumor size, distant metastases at the time of diagnosis, and extrathyroidal extension.7,14,37 Although it is suggested that the prognostic impact of lymph node metastases remains controversial,38,39 some authors defined that a lymphatic local commitment is associated with an increased risk of tumor recurrence and a lower survival rate.15,37,40
A recent study found that age is not a risk factor for recurrence or a survival prognostic factor, so it should not be used as an independent factor in making treatment decisions. 8 While another study found that variables such as age, tumor size (T4), distant metastasis (M1), stage IV, thyroidectomy extension, and RAI are prognostic factors that affect survival at 10 and 15 years, 33 other retrospective studies established a poor prognosis in older patients with well-differentiated TC. 41
Some authors have determined sex as a prognostic factor; 42 however, many others argued the opposite. 43 A study conducted in 2004 and another in 2008 argue that parameters such as gender, lymph node metastasis, and lymph node dissection didn´t show a significant impact on survival.7,33
Other variables not mentioned such as a family history of PTC, advanced disease stage (III or IV), and the extent of thyroidectomy have been recognized as statistically significant predictors of recurrence and survival. 9 Likewise, factors such as invasion of lymphatic vessels, blood vessel invasion, muscular invasion, age over 45 years, tumor size greater than 4 cm, distant metastasis, follicular subtype (histology), capsular invasion, and thyroidectomy extension, have been associated with poor survival at 5 and 10 years. 7
Since the results of these studies appear to be closely related to all risk factors mentioned above, they have been used to develop various prognostic staging systems, to identify patients at low or high risk of recurrence or cases of death related to PTC. 44 These strategies include the AGES (Age, tumor Grade, Extent, and Size), 28 AMES (Age, Metastases, Extent, and Size), 27 DAMES (DNA ploidy, Age, Metastases, Extent, and Size), 30 MACIS (Metastases, Age, Completeness of resection, Invasion, and Size), 29 GAMES (Grade, Age, Metastases, Extent, Size), 31 and TNM (Tumor size, Nodal metastases, distant Metastases). 32
Implications of this study
In our population, performing initial surgery or other more intensive treatments, PTC has lower rates of recurrence and mortality with a low rate of surgical complications. Furthermore, it has been confirmed that lesion size, involvement of surgical margins, tumor confined to the thyroid gland (no extrathyroidal extension), presence of lymph nodes, and serum Tg at 6, 12, and 24 months after surgery are prognostic factors to be reviewed in patients with PTC to determine the possibility of recurrence and thus giving a more aggressive initial treatment.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.