
Abstract
Objective
The advantages and popularity of technology among learners have vaulted it to the forefront of medical education. The current state of learning and teaching intertwined with technology in medical education and residency is described. Following these characterizations, consideration is given to changes worth exploring in the habits of mind and habits of action that medical students and residents exhibit to deepen their learning and improve their performance.
Methods
Review of literature was conducted to summarize relevant transformations in instructional practices in medical school and residency that can contribute to more effective learning environments.
Results
Learners have different approaches that will include differing uses of technology. Technology encourages multitasking, information overload, and the increasing prevalence of invalid information. Implementing bite-sized learning approaches, problem-based or case-based formats, questions, and alternative hypotheses encourages learners to channel technological innovations into their own styles of learning.
Conclusion
To build knowledge in the technological era of learning, do not take learners’ digital readiness for granted. Approach technology as a tool to be wielded when required and not as a crutch.
Introduction
Graduate medical education programs seek to educate adult learners from diverse backgrounds efficiently and effectively. Although technology plays a critical role in learning and teaching practices, the inadequate use of smart technologies may have an inverse effect on the intended outcomes. Technology today has many applications to facilitate reading and learning from texts, yet the availability of these digital tools does not guarantee their efficient or effective use. Technology may widen the differences in adults’ approaches to learning, and an adult learner must be digitally ready and confident in their online skills to accurately distinguish between trustworthy and untrustworthy online information.
The growing presence of technology in education has also burdened the adult learner with information saturation. In this article, these dilemmas surrounding the advent of technology in medical student education and residency are discussed in an effort to work toward a more effective and equitable learning environment.
Part I: Where are Learners Today?
Graduate medical education programs have a difficult task undertaking the teaching of adult learners who come to the experience from diverse backgrounds. Each residency program must tailor to the needs of its trainees, keeping in mind that the approach to learning can differ greatly between individuals at the same level of training. For example, adult learners often differ in the environment in which they prefer to learn (e.g., group learning vs. independent study) and in their preferred study medium (e.g., digital or print style).1,2 Some learners respond well to simulation tasks, while others learn better by watching their teachers work clinically on real patients. Advancements in technology have widened the differences in adults’ approaches to learning by broadening the options they have for gathering information, acquiring knowledge, and honing their skills. 3 However, the overreliance on or misuse of technology has been criticized as a crutch. 4 For better or worse, both teaching and assessment have gravitated toward technology. Standardized assessments, question banks, virtual lectures and conferences, flashcards, e-books, online simulations, and more have saturated the market for medical students. In this article, we attempt to answer the question: Is technology always the best resource for learning, and how can it be best utilized?
Massive amounts of information are consumed daily during residency. Residents must find an effective way to manage that deluge of information if they are to learn what is essential and not find themselves swept away. Residents are often responsible for self-teaching. Yet, without guidance, even these mature students may find themselves ill-equipped to cull key concepts or critical content from all the online information they encounter. 5 It may seem unnecessary to teach adult learners who have grown up with digital technologies how to engage with them more effectively, but in actuality, these individuals are not always as efficient with digital mediums as they suppose themselves to be.6,7 They may be facile at maneuvering through the latest technologies, tech features, and apps, but they still require instruction that focuses on evaluating, synthesizing, and integrating the information they locate online.8,9 They also can be susceptible to biased, inaccurate, and intentionally misleading content populating digital media. 10
In understanding where the learner is with respect to the efficient use of smart technologies, we must take into question the concept of digital readiness. According to a recent PEW report, 3 digital readiness includes 3 tenets. First, the adult learner in residency must have digital skills capable of initiating useful online sessions and browsing resources and various databases. Second, trust is a vital component when determining the accuracy of information online. 8 Finally, use determines the degree to which the adult learner can carry out tasks with the digital tools at their disposal. Technology today comes equipped with a large array of tools not available in the print-only world that can facilitate reading and learning from texts, including apps for annotation and notecards, digital glossaries, and tools for collaborating. 11 Yet, the availability of these many digital tools does not ensure their smart use. Therefore, while it may seem counterintuitive, learners require strategic guidance if they are to engage efficiently and effectively with digital texts and tools in a manner that promotes comprehension and retention.12,13 Those strategies may include monitoring one’s understanding, reading more slowly, periodically stopping to reflect on or ask questions about what was read, annotating digital texts, and writing down on paper key points or questions.13,14 “Digitally Ready” adults must be confident in their online skills, accurately distinguish between trustworthy and untrustworthy online information, and have enough familiarity with technology to utilize its advantages. 4
In residency, there are often competing demands and, consequently, decreased time for reflection and engagement with material, which can lead to burnout (Figure 1).
15
Virtual lectures have recently increased in popularity. COVID-19 pandemic forced physicians to rapidly adapt and integrate new technologies into daily practice and into medical education.16,17 For instance, recent studies on virtual lectures during the COVID-19 pandemic found that one of the significant downfalls of a virtual curriculum was the loss of student–faculty interaction.16-18 One technique that might help maintain connections between students and faculty during online lectures is the use of polling systems like Poll Everywhere®. These systems can also allow teachers to quickly gauge students’ understanding of key points in the lectures before moving on. Real-time polling could also serve as a catalyst for class discussions of issues. Burnout cycle experienced by too many medical students and residents.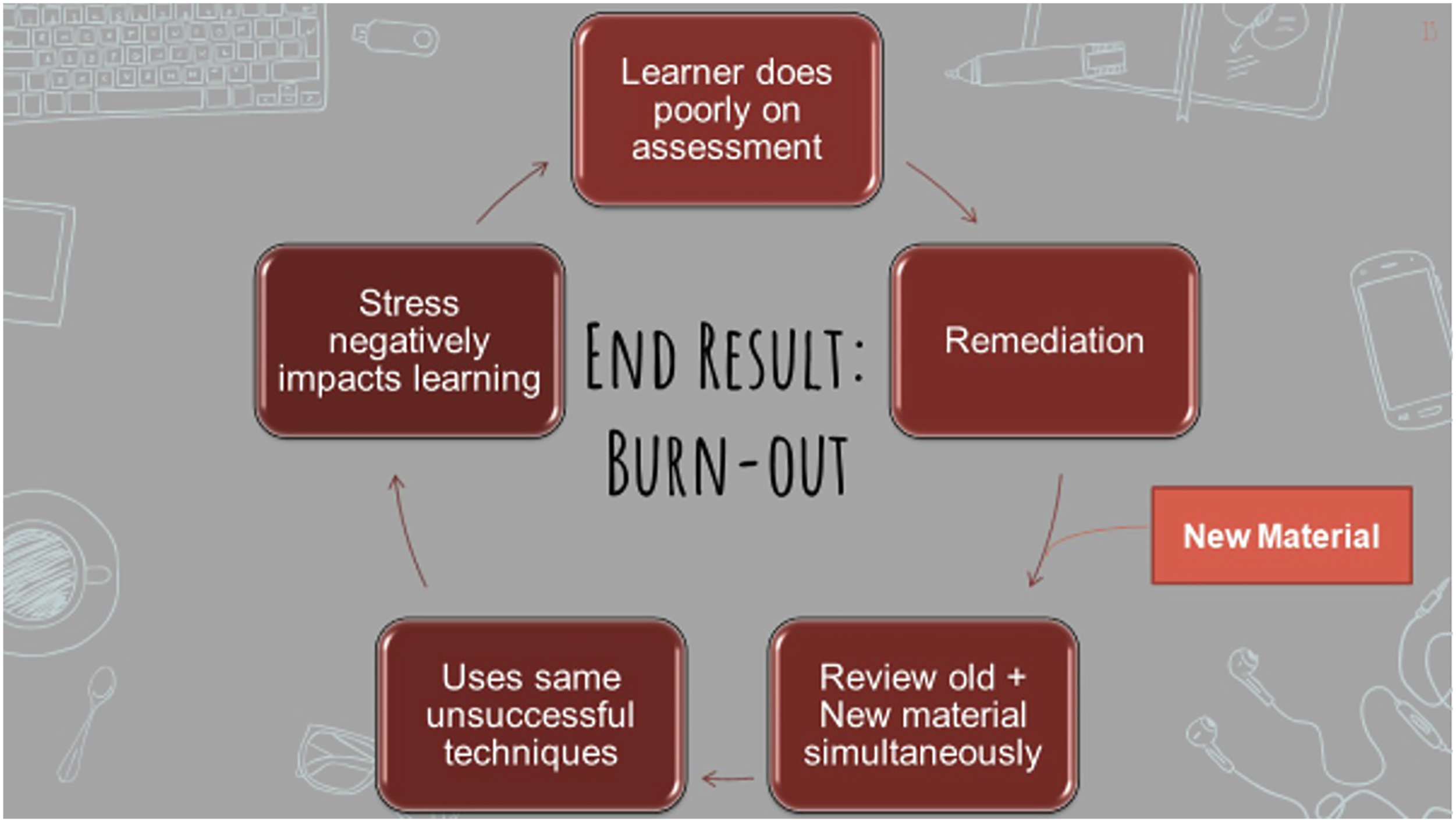
The infrequent assessments that are part of medical school programs do not and cannot cover all the material residents are expected to learn. Thus, medical students and residents want to self-assess frequently to monitor their progress and keep content fresh in memory. 19 For that reason, these learners often spend a good amount of their personal funds on question banks and other daily forms of self-assessment. However, some useful simulations and scenario-based tools (e.g., Step 3 CCS case simulator software) are simply out of reach financially and technologically for many students.
Part II: How are Learners Being Taught?
Even though reading from a textbook has gained a reputation as an “old-school” style of learning, it is still considered a tried-and-true staple of learning in residency. One study by Singer and Alexander explored the differences in comprehension of 90 undergraduate students who read both digital and print versions of news articles and book excerpts on topics of childhood ailments. 2 Not surprisingly with millennials and subsequent generations that have grown up with Internet access and smart devices, survey results demonstrated a significant preference for digital text. Students additionally felt they understood the material better when reading digitally. Paradoxically, when those undergraduates were asked to recall key points linked to the main idea and other relevant information of the passages, their comprehension was significantly better when they read the printed and not the digital text—evidence that these students were poorly calibrated.
What makes learners comprehend and interact with various educational mediums differently? Singer Trakhman proposed that underlying differences may be the result of navigational issues with the document.
14
For example, research has shown that effective readers use the location of information on the printed page to prompt their recall.20,21 When reading digitally, this sense of location is disrupted due to scrolling; in fact, scrolling itself negatively affects comprehension performance.
22
Another factor that affected digital reading performance across several studies was reading time.
22
Specifically, students were found to read significantly faster on screen than on print, which could mean that they were not paying close attention to the content when they were online. In a person-center analysis that looked at an array of navigational behaviors students exhibited during digital reading in relation to comprehension, they identified 4 distinct learner profiles:
23
Regulators and Gliders registered the best comprehension scores and were better calibrated than Plodders and Samplers both in print and digitally. Depending on their online reading profiles, medical students and residents may likewise find their comprehension of digital texts negatively affected.
In addition, despite its notable advantages, technology can be a significant distractor. According to Matei, who monitored phone use with the RescueTime app, the average person spends more than 3 hours per day on their cell phone, not including television and laptop use time. 24 The act of using personal devices for learning creates the unintended consequences of distraction and impulse to multitask (e.g., checking emails, text messages, and social media). These distractions are often misrepresented as multitasking. Despite what the label suggests and what many students believe, multitasking is detrimental to learning since no one can perform 2 tasks simultaneously unless one of those tasks is entirely habituated (e.g., brushing teeth and walking). Numerous research studies have established this fact and have shown that technology encourages multitasking.25-27 The impetus for such multitasking often involved such tasks as responding to incoming text messages and e-mails or checking in with social network sites. 27
The growing presence of technology in graduate medical education has thus become a double-edged sword. The adult learner is now burdened with information saturation, the proliferation of misleading and malicious online content, the struggle to use valid evidence to support claims, and the tendency to treat complex issues in an overly simplistic fashion. 5 The high workload of graduate medical education training fosters an environment that encourages multitasking and technology can contribute to constant distractions. 28 Nonetheless, despite such pitfalls technology has become an essential tool in residency training. 29 It provides easy access to limitless resources, surgical videos, anatomy software, and spaced repetition notecards. Vula, an open-access atlas designed to provide free otolaryngology operative information to the developing world, and other resources can be invaluable sources of critical information in a timely and affordable manner. Similarly, social media in medicine (e.g., MedTwitter) has been shown to increase publication citations and is helpful for staying in-the-know on medical guidelines and updates. As technology developments continue to transform the delivery of clinical medicine, so too will it continue to impact the manner in which medical students and residents become doctors.
Part III: What Transformations in Learning are Needed?
When we juxtapose the demands placed on medical students and residents with the ways in which they are being taught, it is evident that the conditions for optimal learning and performance rarely exist. Thus, to function in these non-optimal conditions, many students revert to an information management mindset instead of investing in knowledge building. 30 Information management is a general approach to learning that entails doing what is minimally necessary to get through the array of assigned tasks or responsibilities. Often that means that students work to acquire whatever knowledge or skills they see as needed in the short term, focusing on the content they view as pertinent to the tasks upon which they will be judged. Because information management is so heavily tied to tasks and responsibilities that may be short-lived, retaining what is learned through this approach can be problematic. When the tasks and duties are completed and the demand is no longer pressing, the associated learning can fade from memory.
In contrast to information management, knowledge building is an approach to learning whereby the students are invested in acquiring knowledge and skills that they consider valuable and essential for their current and future success.
30
As shown in Figure 2, what content draws their attention and time during learning is based on what they perceive as important and credible information. The understandings they acquire are intentionally and strategically linked to prior learning forming an interconnected, principled body of knowledge that is apt to endure in memory and be more readily retrievable when the need arises. Moreover, that principled body of knowledge allows learners to critically judge the information they subsequently encounter in print, online, or in lectures. Knowledge builders do not simply accept what they see or hear at face value—they weigh its veracity and usefulness.
31
Characteristics of knowledge building.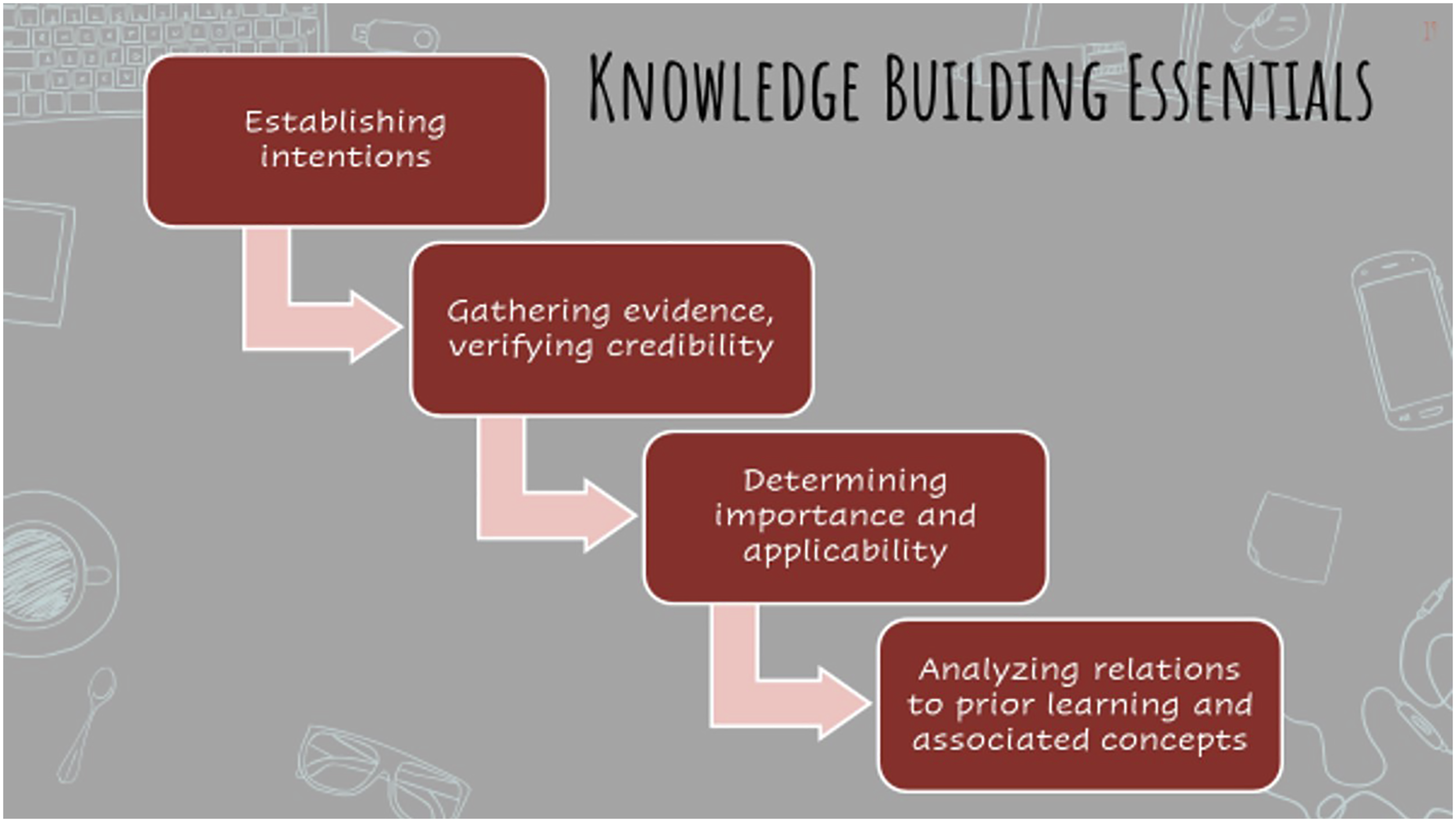
One reason for the prevalence of the information management approach to learning, even among very capable individuals, is that the educational system does not teach students how to be knowledge builders. On the contrary, the nature of school at all levels is too often about covering as much content as possible and focusing on test performance as indicators of success. 30 Mature learners like medical students and residents, therefore, need to rethink the very mindset and work habits that proved success throughout much of their prior educational experience. Although the mental effort and strategic processes involved in knowledge building may initially be unfamiliar and more time-consuming than those aligned with information management, their repeated use can lead to habits of mind that are second nature and that will serve medical students and residents throughout their careers. Further, this personal investment in knowledge building will be invaluable for anyone who hopes to become highly competent or even an expert in the medical profession. 31 In fact, there is no other path to high competence or expertise in any complex field.
But how does one become better at knowledge building? There is no singular answer to this important question. However, we can offer some guidance in that regard: • Think of your professional training as interconnected and a process of expertise development that requires time and personal investment that cannot be rushed. • Operate with a knowledge building mindset and be aware of when, where, and why you shift to information management. • Self-test understanding frequently as you are learning to identify content that requires reinforcement. • Learn to question and challenge information as it is encountered; healthy skepticism leads to deeper learning • Employ technology to assist in structuring what you read, heard, or view into meaningful chunks (e.g., illness scripts; iconic images; families of cases). • Learn to bootstrap your knowledge by forming connections between new topics, subjects, procedures, and what you already know. In effect, hone the ability to reason relationally. • Find ways to apply new learning to relevant tasks or problems.30,32
Before we leave this topic of information management and knowledge building, it is important to establish that both these approaches to learning are necessary within professional education. Heavy demands will inevitably be placed on medical students and residents. Given the overload of information and high workload in medical school and during residency, it can be easy to revert to information management. Nonetheless, there is a time and place for information management even as students are striving to become knowledge builders. The key for these learners is to be aware and intentional about when, where, and why to engage in information management or knowledge building and to use technologies wisely to assist in these processes. 32
Part IV: What Transformations in Instruction are Needed?
If, as we have suggested, the tendency for information management to take hold in learners at all academic levels is attributable in part to their educational experiences, it is worth considering what changes in those experiences should occur if knowledge building is to be promoted. Here, we will consider several practical guidelines. • Teach
It has been said that school curricula are a mile wide and an inch deep, and each year the material to be taught and to be learned grows.
33
This reality leaves teachers who feel obliged to “cover the content” doing little more than just mentioning everything and not really teaching anything. Mentioning puts the onus on learners who often lack sufficient background and guidance to fill in the informational gaps the best they can.
34
However, if knowledge building is the goal, then it is essential for teachers to be far more selective in what content they highlight and they need to allow more time for their students to reflect on and apply what they are learning. • Treat the
Apprenticeships have existed for centuries as a way for master craftsmen to pass along their collective wisdom to promising newcomers. These master craftsmen would model some portion of a complex task and then diligently observe as the apprentice tried to replicate that process. Feedback and more modeling might follow until the apprentice was able to execute that piece of the task well. This cycle would repeat as each new element was added. In much the same way, attending physicians and instructors working with residents should see themselves in the role of master craftsmen who model and guide their apprentices. As such, they need to be cognizant of their residents’ strengths and needs, ensure these apprentices have ample opportunities to practice under their careful supervision, and offer whatever instructive feedback is required.
35
•
When new topics or procedures are being presented to medical students and residents, it is not only helpful to teach more about less but also to signal specific elements of the content that deserves greater attention from those learners. The research on information processing has shown the value of signaling for acquiring and retaining information.
36
Signals can be trigger words like first, principal, or essential, or they may take the form of bolded or italicized words and phrases, summaries, or other visual cues. When lecturing, instructors should also intentionally signal when information warrants increased attention. Periodically summarizing or restating what has been shared can also reinforce key ideas. Another way instructors can help learners navigate the flow of information is by providing them with an online advanced organizer that lists the main points or terms to be covered. Students can then use the organizer for notetaking (e.g., reMarkable 2 or other tablets). • Incorporate
Another practical step that instructors can take to guide students’ learning is to restructure the body of content around a topic into smaller bite-size segments interspersed with opportunities to practice and apply the just-taught subject matter.37,38 The micro-lessons can make effective use of technology to present supportive videos, application materials, or mini-assessments. These bite-size approaches also allow for small group interactions where critical content can be discussed, rehearsed, and possibly extended. • Consider
A substantial number of medical programs internationally have taken an alternative approach to manage the extensive body of knowledge and skills that medical students and residents must master.39,40 Traditionally, instruction unfolds by first building up students’ foundational knowledge and skills and then applying the acquired content to cases. In problem-based or case-based learning that script is flipped. Specifically, learners are first presented with a medical problem or case to be solved and then they go about building the knowledge and skills the solution requires. Even if a program is not formalized as problem-based or case-based, it is possible to introduce mini-problems or cases into the content. • Use instructional time to
It is increasingly common for medical students and residents to engage in self-teaching of instructional content through the use of online videos, simulations, mini-assessments, and the like. Although there can be a great variability in students’ ability to self-teaching, there is evidence that this process can result in at least moderate gains when compared to in-person instruction.
41
Yet, self-teaching does not have to be an all-or-nothing proposition for medical students and residents or their instructors.
41
Instead, in keeping with other practical guidelines we offered such as teaching more about less, bite-size lessons, and problem-based approaches, medical students and residents should be encouraged to learn the more basic information on their own or in groups before lectures. The lecture can then move beyond this more readily acquired content to delve into more nuanced, integrated, and complex subject matter that benefits from instructors’ experience and expertise. Instructors and residents could even work together to compile quality resources that students could use for self-teaching. •
One final guideline we would offer as a step toward transforming learning environments that foster information management into educational experiences that promote knowledge building relates to more open channels of communication. Medical students and residents should feel that their experiences, inquiries, and insights are valued parts of the instructional discourse. By not just allowing students’ observations, questions, and alternative hypotheses into the learning environment during training but welcoming those contributions, the understanding and curiosity of medical students and residents can be fostered. 42 Furthermore, it is through these interactions that instructors can be better informed about what their students know about the subject matter at hand and what alternative perspectives they may have to offer.
Conclusion
The advantages and popularity of technology among learners have vaulted it to the forefront of medical education. Learners have different learning approaches that will include differing uses of technology. Technology encourages distraction and multitasking, which can negatively impact learning. Learners do not often learn efficiently or effectively due to information overload and the increasing prevalence of invalid information. We must do better in the assessment of the true state of learners’ knowledge with the understanding that information management and knowledge building are both effective tools in their own right. Our assessment of knowledge should gauge the ability to analyze and solve problems from a background of previously learned principles. To build knowledge in the technological era of learning, do not take learners’ digital readiness for granted. Approach technology as a tool to be wielded when required and not as a crutch. Implementing bite-sized approaches, problem-based, or case-based formats and welcoming observations, questions, and alternative hypotheses will encourage learners to channel technological innovations into their own styles of learning.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Written informed consent for publication of this deemed not necessary by the University of Pittsburgh Institutional Review Board.