
Abstract
Introduction
Pediatric vocal cord paralysis has a myriad of etiologies, including neck or intracranial surgical injuries, birth trauma or congenital neurologic condition. In 7% of cases, the vocal cord paralysis is related to a neurological disease. 1 Type 1 Arnold Chiari is a rare neurological malformation that may be associated with hydrocephalus, myelomeningocele and uni- or bilateral vocal cord paralysis. 2 The vocal cord paralysis in type 1 Arnold Chiari malformation results from the disruption of neural motor outputs to laryngeal muscles. 2 To date, there was no documented case reporting the occurrence of vocal cord paralysis related to the neurosurgical decompression procedure in type 1 Arnold Chiari patient. In this paper, we reported the first cases of bilateral vocal cord abduction paralysis related to suboccipital decompression and C1 laminectomy in a child with type 1 Arnold Chiari malformation.
Case Report
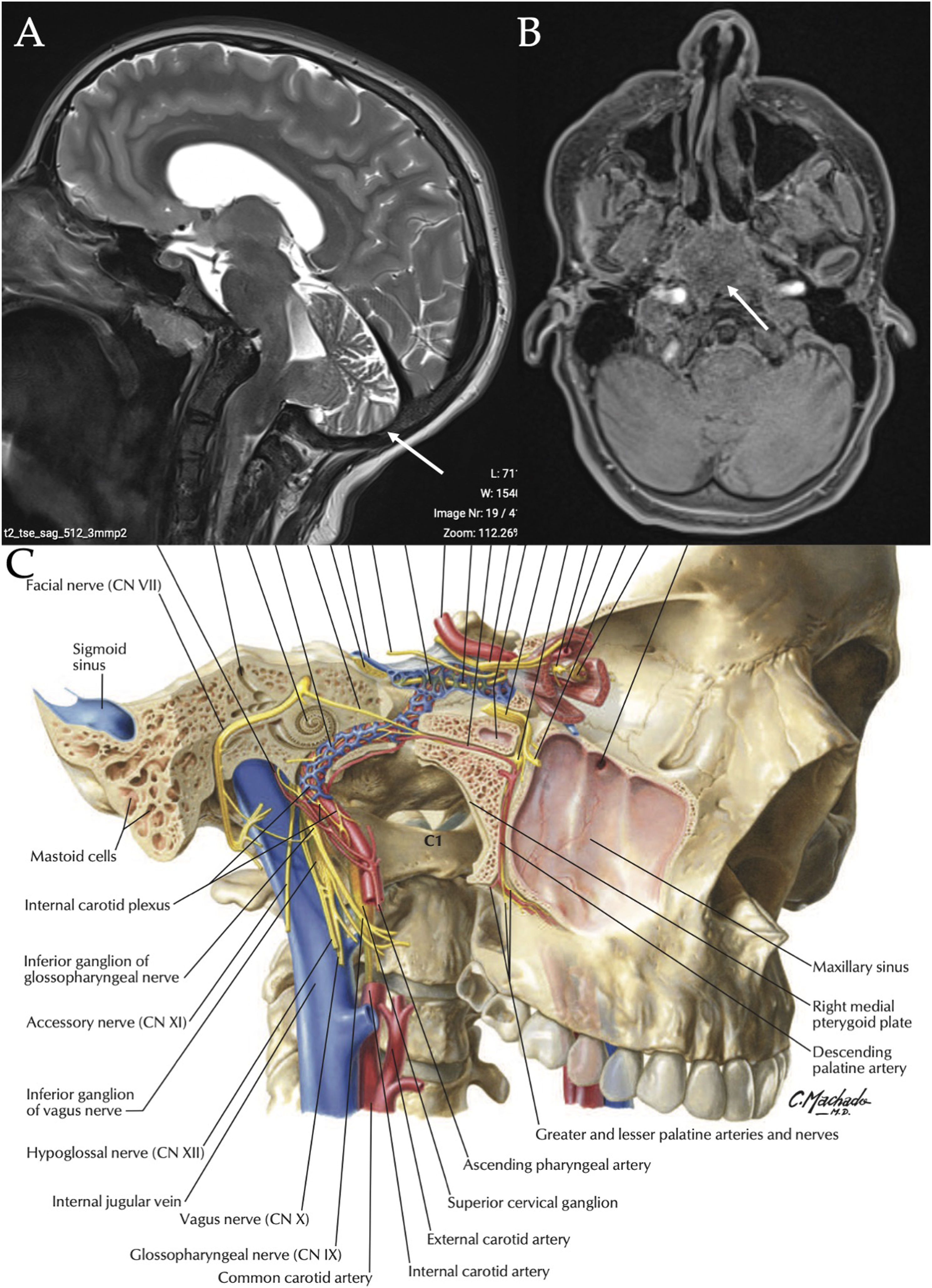
A 12-year-old female presented in the Laryngology Office for aphonia, severe dysphagia, and accumulation of saliva in the laryngopharyngeal cavities. The patient underwent suboccipital decompression and C1 laminectomy one month prior to the consultation for a type 1 Arnold Chiari malformation discovered in the Emergency department. At this time, patient had diplopia, headaches, vomiting, and instability. The MRI revealed a type 1 Arnold Chiari malformation and she underwent two 48-hour consecutive neurosurgical decompressions. The second procedure (revision) was performed because there was a posterior compression of the cerebral stem. In the postoperative period, the patient suffered from dyspnea (aspirations), severe cough, aphonia, accumulation of saliva in the upper aerodigestive tract, and severe dysphagia. Surgeons proceeded to an urgent tracheotomy to protect the respiratory tract from the saliva aspirations. The neurological examination reported a bilateral lesion of the following cranial nerves: IX, X, and XII. Figure 1 reports the patient MRI and the anatomic location of these cranial nerves regarding C1. The fiberoptic endoscopic evaluation of swallowing and the stroboscopical examination found a bilateral vocal cord abduction paralysis (Figure 2), a lack of laryngopharyngeal mucosa sensitivity, and an absence of contraction of pharyngeal constrictor muscles. Speech therapy and B12 vitamins were prescribed without improvement or recovery of the swallow and laryngeal functions over the 15 months of follow-up. The tracheotomy, gastrostomy and the manual aspiration of excess saliva was maintained over time. Bilateral vocal cord abduction paralysis. Notes: There was excess of saliva in the upper aerodigestive tract because lack of pharyngeal constrictor muscle activity (A). The vocal cords were paralyzed in abduction position (B). Cranial nerve location regarding C1 and patient imaging. Notes: T1 MRI in sagittal (A) and axial (B) section reported the herniation of the hindbrain into a low occipital or high cervical meningoencephalocele. The anatomical picture
6
(C) describes the anatomic relation between C1 and the following cranial nerves: glossopharyngeal, vagus, and hypoglossal.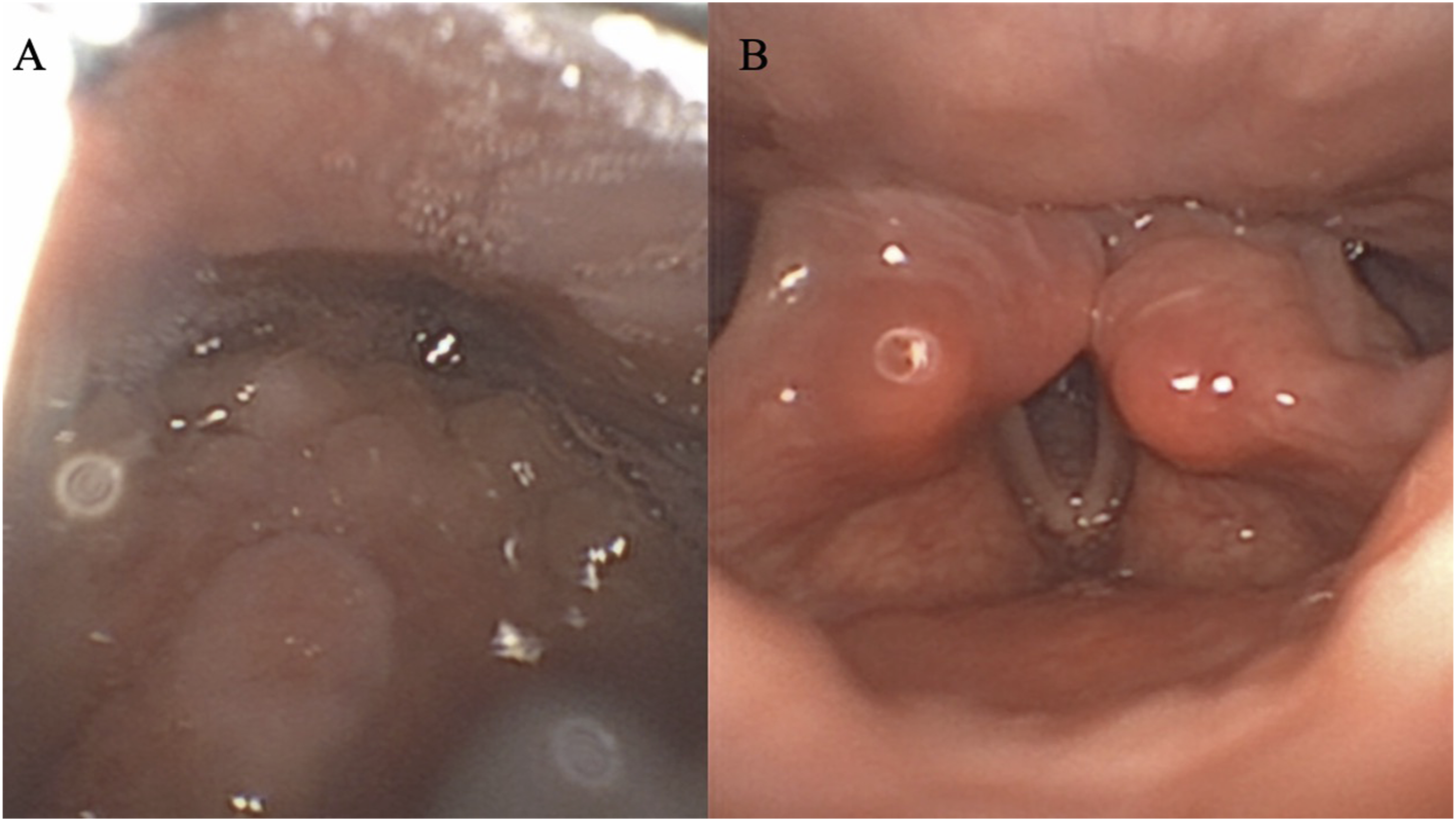
Discussion
To the best of our knowledge, this is the first case report of a bilateral vocal cord abduction paralysis following decompression surgery of type 1 Arnold Chiari malformation. Indeed, our patient did not report voice, swallow, or tongue function abnormality prior to the procedures. The most common complications of decompression neurosurgical approach in Arnold Chiari patients included pseudomeningocele, meningitis, hydrocephalus and cervical instability. 3 The need of revision surgery concerned 8 to 18% of cases, 3 and may be associated with a higher risk of complications. However, there is no concurrent bilateral vocal cord and tongue paralysis in the literature. In untreated type 1 Arnold Chiari malformation, the risk of bilateral vocal cord paralysis is due to the protrusion of medulla and cerebellum through the foramen magnum and the related compression or extern traction upon the vagus.4,5 The vocal cord paralysis may, in these cases, recover after a suboccipital decompression and C1 laminectomy. 3 In the present case, the nerve lesions occurred probably during the C1 laminectomy, through section, excessive compression or traction of the cranial nerves. From an anatomical standpoint, both glossopharyngeal and vagus nerves have their roots on the lateral side of the medulla oblongata and come out of the skull from the jugular foramen. Vagus, glossopharyngeal, and hypoglossal nerves are located close to each other at the level of C1 vertebrae (ganglion of vagus nerve), which is not the case of the accessory nerve, as it parts away just before the ganglion.
Conclusion
In this paper, we reported a very rare case of aphonia, dysphagia and aspiration-related dyspnea after a C1 laminectomy in a child who underwent neurosurgical procedure for a type 1 Arnold Chiari malformation. The bilateral lesion of IX, X, and XII cranial nerve is a rare but severe complication of this kind of procedure and highlights the importance of surgical steps of the procedure in front of the C1 vertebrae.
Footnotes
Acknowledgments
B. Johnson for the proofreading of the paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.