
Abstract
Objective
Schwannomas are common nerve sheath tumors and may occur anywhere in the body. 4% of head and neck schwannomas occur in the sinonasal cavity, and fewer yet have an intracranial component, making these presentations extremely rare. Furthermore, schwannomas present with nonspecific imaging signs and can only be definitively differentiated via histopathologic review, leading to misdiagnosis as various nasal tumors. We aim to conduct a review of published literature on sinonasal schwannomas with and without intracranial extension and provide additional case representations.
Methods
A literature review was conducted using the PubMed Database with the terms “sinonasal schwannoma,” “intracranial,” “anterior skull base,” and “schwannoma.” Results were reviewed, and additional cases identified were referenced and included in the study. Inclusion criteria were any case with intracranial extension of the schwannoma. There were no exclusion criteria. Review data was compiled into Excel and used for data analysis and comparison. Additionally, a search was done within our institution to identify additional cases of sinonasal schwannoma.
Results
We identified 17 cases of sinonasal schwannoma with intracranial extension, five from our institution and twelve from literature. Analysis revealed: 8 females (47%), 9 males (53%), 9 patients presented with headaches (53%), 6 patients presented with anosmia (35%), 4 patients presented with nasal obstruction (24%), and 2 patients with no symptoms (12%). Mean age and median were 39.4 ± 10.1 and 40, respectively. For treatment, 4 patients underwent endoscopic resection (24%), 11 underwent craniotomy (65%), and data was unavailable for 2 patients. Post-treatment complications occurred in 6 patients, 5 had CSF leaks (29%) and 1 had a hematoma (6%).
Conclusion
We identified and discussed 17 cases of sinonasal schwannoma with intracranial extension. We hope our review provides insight for clinicians to maintain schwannoma as a potential differential when evaluating nasal and anterior skull base masses.
Introduction
Schwannomas are slow-growing and benign tumors thought to arise from Schwann cells, which are responsible for the myelination of nerve fibers. While schwannomas may occur anywhere in the body, roughly 25–45% of all schwannomas occur in the head and neck region, the most commonly affected location being the vestibulocochlear nerve. 1 Sinonasal schwannomas account for 4% of all head and neck schwannomas, with fewer than one hundred reported cases.1-3 The clinical presentation of sinonasal schwannomas is generally variable and nonspecific due to tumor location and indolent course. Additionally, when schwannomas extend intracranially, there is considerable overlap with more common entities. Some patients are asymptomatic and diagnosed after workup of incidental findings on imaging. When present, symptoms can vary from anosmia, nasal obstruction, epistaxis, headaches, visual disturbances, and fullness.2,4-6 This review tries to elucidate characteristic features of sinonasal schwannomas, however, the findings are nonspecific. Our set of cases demonstrates that schwannoma must be on the differential for a sinonasal or anterior skull base mass. We consider an additional 6 cases ranging in size and presentation.
Methods of Review
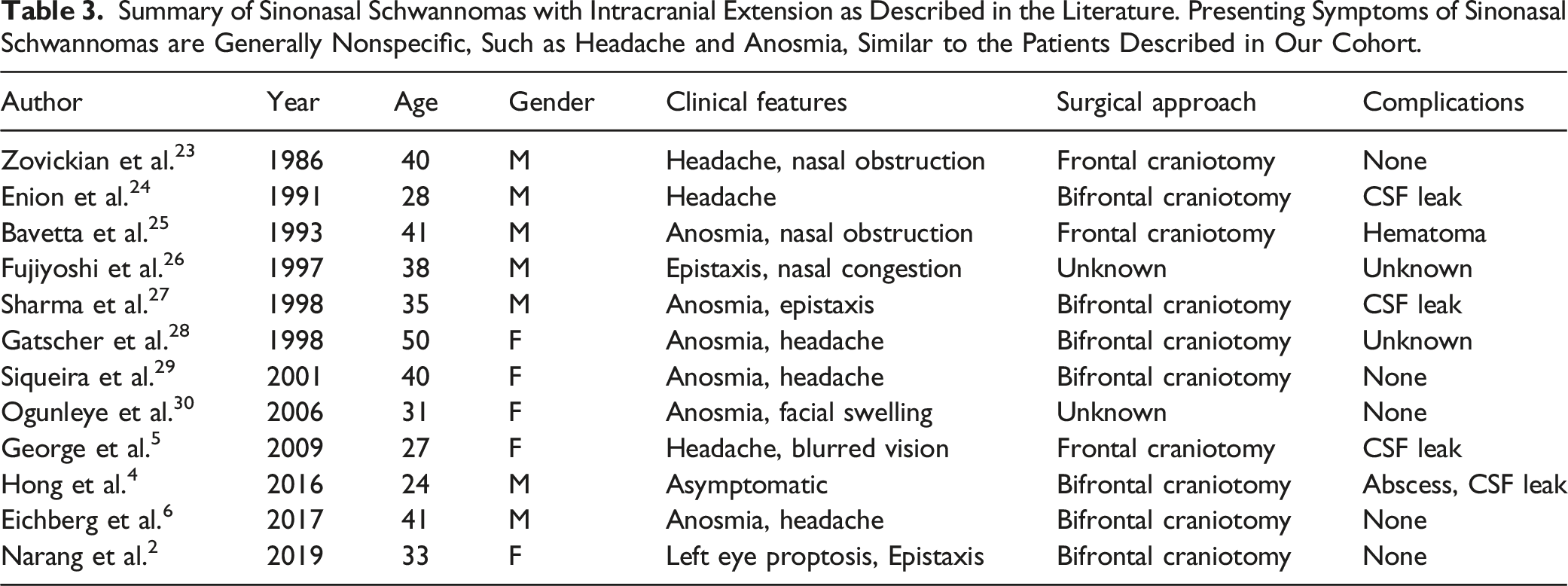
A thorough review of published literature was done to identify additional cases of sinonasal schwannomas with intracranial extension, done via a search of the “PubMed” database. First, a simple search was conducted for “sinonasal schwannoma” and “intracranial.” Following this, another search was done for “anterior skull base” and “schwannoma.” Relevant articles and their references were reviewed, and additional articles of interest were gathered from them. The inclusion criteria for the review were any cases that had sinonasal schwannomas with an intracranial extension. All statistical analysis was done in Excel. Our review identified twelve reported patients with an intracranial extension of sinonasal schwannomas (Table 3).
Patients and Results
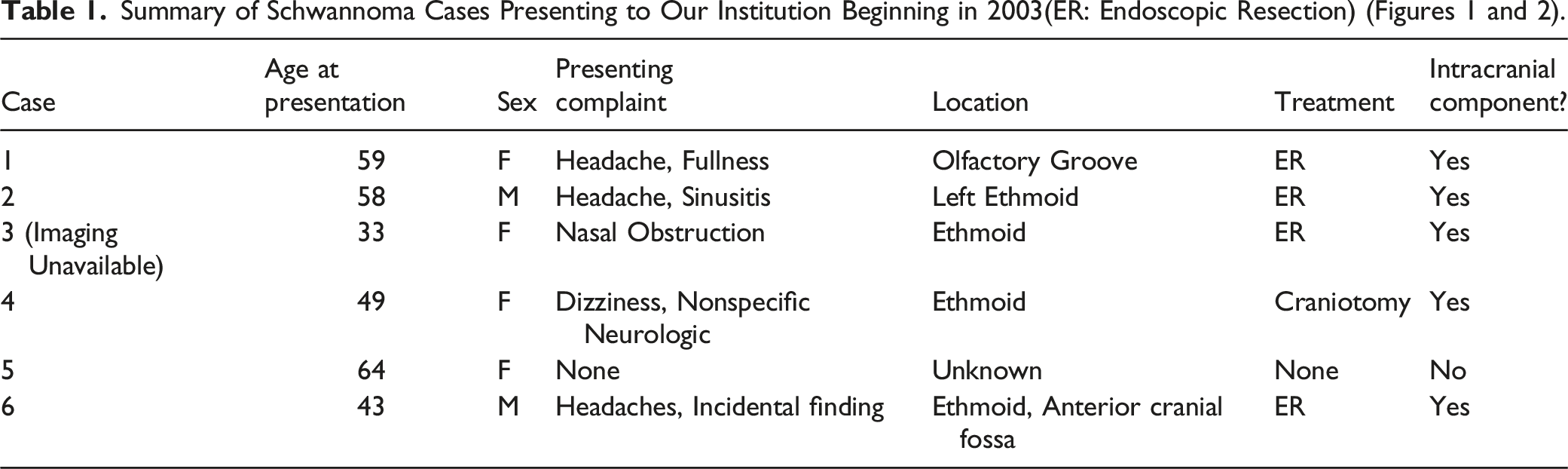
When added to the reported cases in existing literature, the results are as follows: 8 out of 17 cases were female (47%,), 9 out of 17 cases were male (53%), 9 out of 17 patients presented with headaches as the primary symptom (53%), 6 patients presented with anosmia (35%), 4 patients presented with nasal obstruction (24%), and 2 patients had no symptoms, and the mass was found incidentally (12%). The mean age of the 17 patients was 39.4 ± 10.1, and the median was 40. The most common origin location seen was the ethmoid sinus. For treatment, 4 patients underwent endoscopic resection (24%), 11 underwent craniotomy (65%), and treatment data was unavailable for 2 patients. Post-treatment complications occurred in 6 out of the 17, with 5 having CSF leaks (29%) and 1 having hematoma post craniotomy (6%).
Discussion
Schwannomas are tumors of the peripheral nervous system most commonly arising from tumorigenic Schwann cells, which are responsible for the myelination of nerve fibers. They are usually sporadic; however, about 5% of schwannomas occur in relation to the Neurofibromatosis Type 2 mutation.3,7,8 The leading theory on the origin of sinonasal schwannomas is that they arise from the ophthalmic and maxillary branches of the trigeminal nerve or nasal autonomic nerves.
9
Based on our review, there are twelve documented cases of sinonasal schwannomas with intracranial extension, and our series describes an additional five cases, bringing the total to seventeen in published literature (Table 3). Schwannomas have been shown to arise from Schwann cells but more recently have been thought to involve injury to many cell types such as axons, macrophages, T cells, fibroblasts, extracellular matrix, and blood vessels.
7
Schwannomas tend to occur in areas where the nerve is prone to injury or undue stress, such as the trigeminal nerve, which is confined during its course.7,8 While mostly benign tumors, they do have the potential to become malignant. As they grow larger, schwannomas remodel surrounding tissue and bone, leading to invasion of adjacent spaces such as the anterior skull base (Figures 1 and 2). Panel 1. (A–B): Case 1, Homogenously enhancing mass in the right anterior ethmoidal sinus and nasal cavity, extending into the right orbit and anterior cranial fossa. (C): Case 2, Homogenous mass involving the right nasal cavity and anterior ethmoid sinuses with erosion of the cribriform plate and intracranial extension. (D–E): Case 4, Heterogeneously enhancing nasoethmoidal mass with intracranial extension abutting the inferior surface of the frontal lobe. [White Arrows]. Panel 2. (A–B): Case 5, Lesion involving the posterior nasal cavity extending into the sphenopalatine foramen. No intracranial extension. (C–D): Case 6, Large multilobulated heterogeneously enhancing mass centered at the level of the anterior skull base, involving the anterior cranial fossa and nasal cavity. [White Arrows] (E–F): Histology of case 6, Compact hypercellular Antoni A areas and myxoid hypocellular Antoni B areas, nuclear palisading around fibrillary process (Verocay bodies) is seen in cellular areas. Hemosiderin deposition can also be seen as brownish deposits (white circle).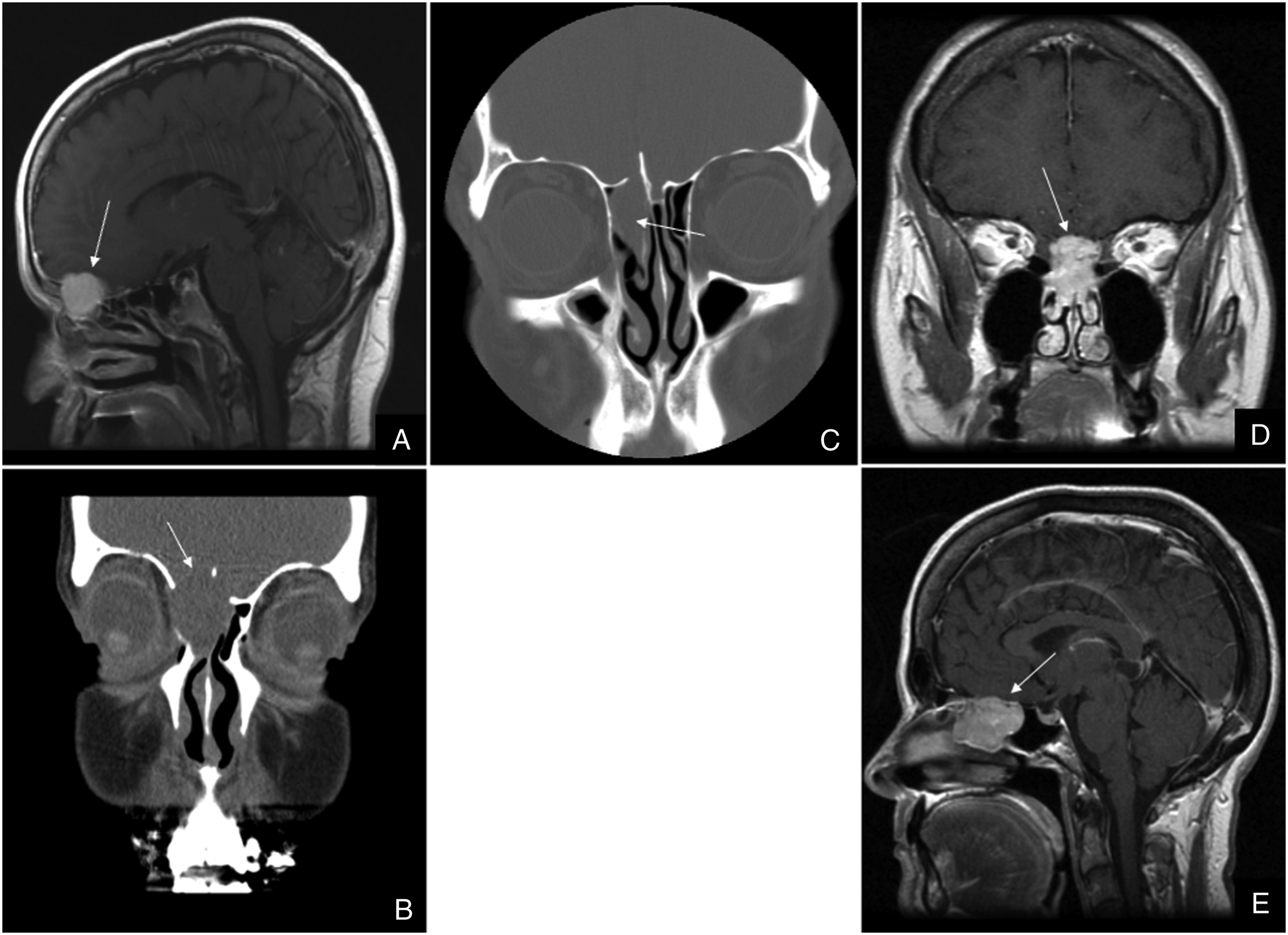
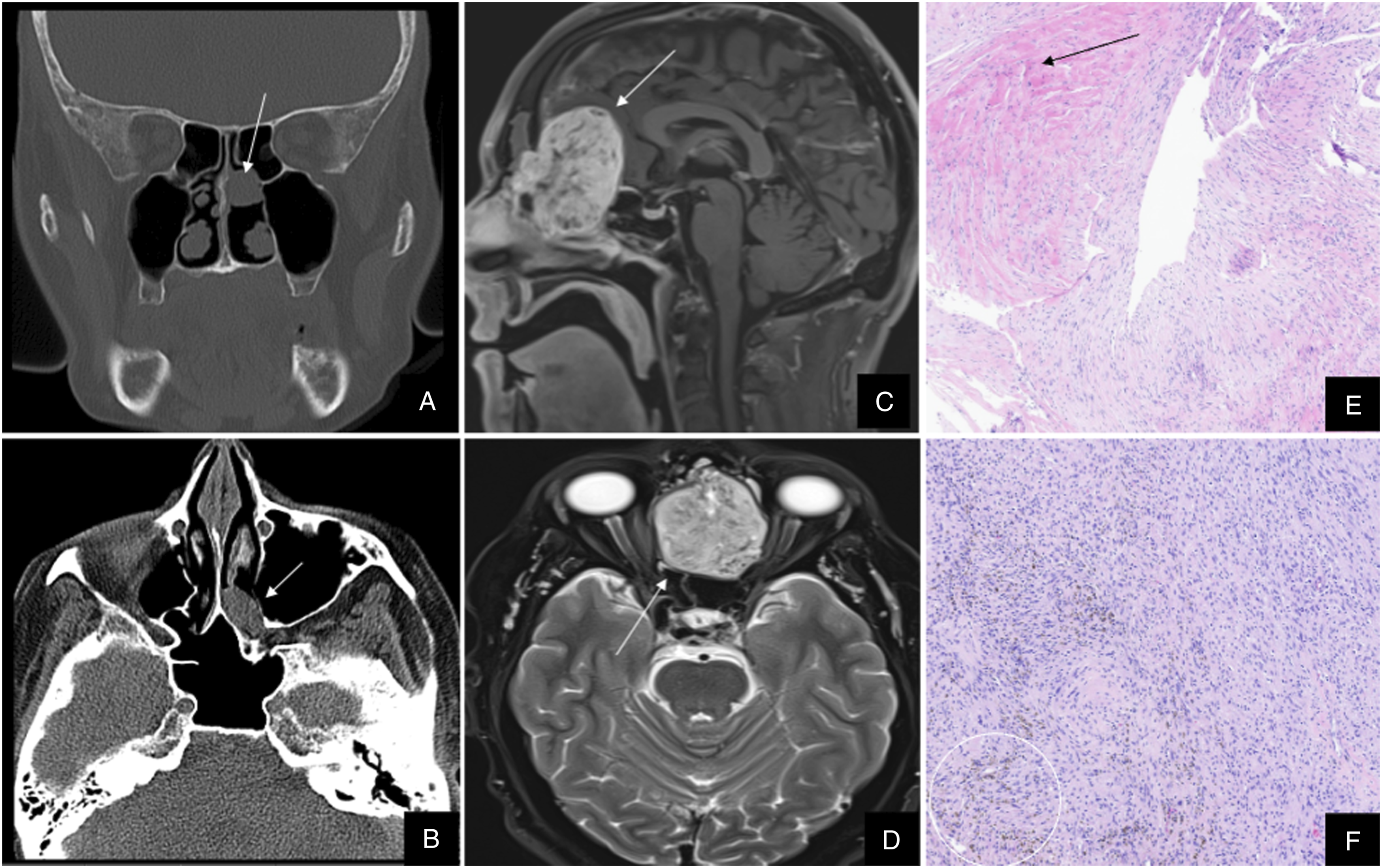
Histologically, schwannomas present with 2 distinct architectures: Antoni Type A and Antoni Type B. Verocay bodies are zones lacking any nuclei amidst areas of organized elongated nuclei, a hallmark feature of Type A. Type B, on the other hand, demonstrates an array of cells with no organization amongst loose stroma and lipid vacuoles in a microcystic pattern. Interestingly, the 2 architectures are not exclusive, and Type A may transition into a structure more similar to Type B.7,8,10 (Figure 2). Schwannoma cells can also be characterized by a + S-100 immunohistochemical stain, further narrowing the differential of nasal tumors. 10
On CT, the schwannomas appear isodense to the brain with moderate enhancement with contrast. Intratumor cystic areas, if present, are hypodense and can help differentiate them from other masses such as esthesioneuroblastomas. MRI findings on T1 reveal iso- to hypointense masses with prominent heterogeneous enhancement and T2 hyperintensity. Furthermore, on T2*, hemosiderin deposition can be visualized in some schwannomas offering a critical diagnostic clue (Figures 1 and 2).11-14
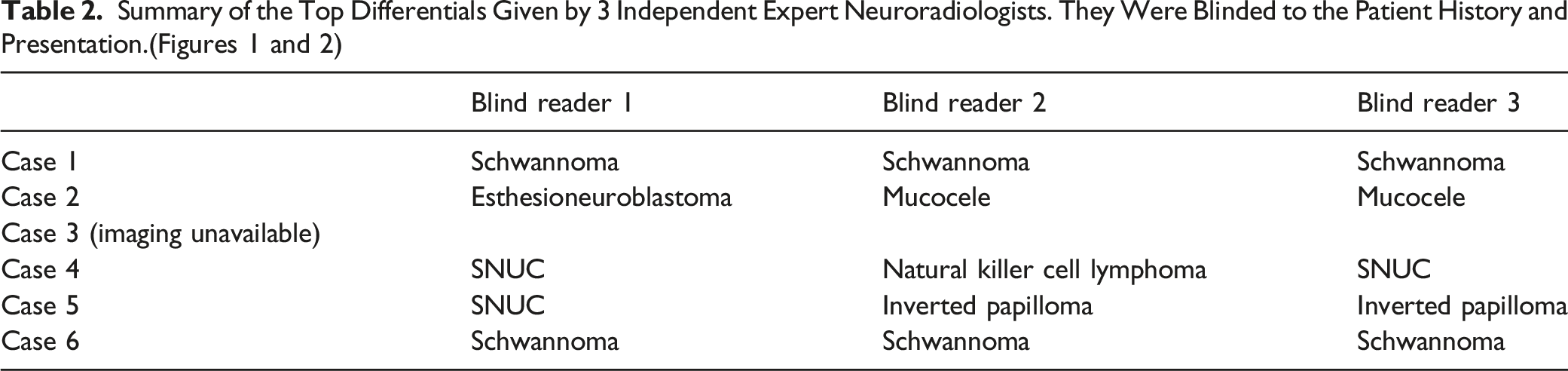
Due to their unusual location and rarity, sinonasal schwannomas are low on the differential diagnosis of masses in the anterior skull base or nasal cavity. Many lesions have overlapping nonspecific symptoms, including esthesioneuroblastoma (ENB), adenocarcinoma, sinonasal undifferentiated carcinoma (SNUC), squamous cell carcinoma, inverted papilloma, sinonasal neurofibromas, and olfactory ensheathing cell tumors (OECT).14-16 While radiographic clues may help with clinical differentiation, diagnosis hinges on a tissue biopsy. Of note, OECT and sinonasal neurofibromas are challenging to differentiate from schwannoma since all are S-100+ and have similar radiologic features. Specialized immunostaining can aid in a more accurate diagnosis.3,10
Summary of Sinonasal Schwannomas with Intracranial Extension as Described in the Literature. Presenting Symptoms of Sinonasal Schwannomas are Generally Nonspecific, Such as Headache and Anosmia, Similar to the Patients Described in Our Cohort.
Conclusion
Although rare, schwannomas in the sinonasal cavity can be easily misdiagnosed due to their indolent nature and nonspecific presentation. As their size increases, sinonasal schwannomas can extend into and remodel the anterior skull base tissues, leading to neurologic symptoms. We reported five cases of sinonasal schwannoma with extension into the cranium, bringing the total in available literature to seventeen. Our review highlights the fact that one must consider sinonasal schwannomas when evaluating nasal masses, resulting in earlier diagnosis and treatment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.