
Abstract
Objective
The aim of this study was to evaluate the effect of vaseline gauze (VG) patching on the treatment of large traumatic perforation of tympanic membrane (TM).
Material and methods
90 patients with traumatic perforation larger than 25% of the TM were randomly allocated into the control group of observation only, VG group, and Gelfoam patch alone group. The closure rate and closure time among the 3 groups were compared at 3 months.
Results
In total, 82 large traumatic perforations were analyzed in this study. The closure rates in the control, VG, and gelfoam patch groups were 84.6%, 100.0%, and 89.3%, respectively (P = 0.637). Post-hoc multiple comparisons showed that the difference between the control and VG groups was significant (P = 0.047), but the difference wasn’t significant between gelfoam alone and control groups (P = 0.699) or VG groups (P = 0.236). The mean closure times were 5.41 ± 1.47, 2.14 ± 0.93, and 3.00 ± 0.62 weeks for the control, VG, and gelfoam patch groups, respectively (P < 0.001). Post-hoc multiple comparisons showed that the difference was significant between the control and VG groups (P < 0.001) or gelfoam alone group (P < 0.001) or VG and gelfoam groups (P < 0.05).
Conclusions
VG improved the closure rate and shortened the closure time compared with observation only, which could be an effective patch material for repairing traumatic lager perforations in the outpatient setting, which is readily available and convenient.
Introduction
Traumatic perforation of tympanic membrane (TM) is the common entity in otology clinics. 1 Although traumatic perforations tend to spontaneous healing, the treatment is still challenging. Most of the small-medium perforations require long healing time of 3–4 weeks, while some large perforations usually fail to heal.1,2 It is well known that the healing of TM perforations depends on the scaffold to support the epithelial migration and thereby close the perforation. Thus, various biological patches have been always used as exogenous biological scaffolds, including paper patching, 3 gelfoam, 4 and egg shell 5 . In recent years, some novel biological materials had been developed to repair traumatic perforations and facilitate the closure.6-9 However, they had not been widely applied in otology clinics because these bioscaffolds are expensive and the ototoxicity is unclear.
Vaseline (petroleum jelly) is known as a lubricant. Vaseline gauze (VG), which is widely used in clinics, possesses the moisture-retention ability and can reduce the pain and prevent synechia formation.10,11 Since VG has no toxic side effects, it has been used to treat burn wound and diabetic chronic wound.12,13 In addition, VG is readily available, convenient, and inexpensive, which is the common medical material in otolaryngology and usually used for nasal and ear packing.14-16 However, to date, little was reported about the effect of VG on repairing traumatic perforations of TM. The aim of this study was to evaluate the effect of VG patching of large traumatic perforation and to compare it with conservative treatment and gelfoam alone patching.
Materials and Methods
Ethical Considerations
The study protocol was reviewed and approved by the Institutional Ethical Review Board of Yiwu central hospital. Written informed consent was obtained from all participants.
Methods
Study subjects were recruited consecutively from patients diagnosed with traumatic perforation who visited between January 2018 and January 2022. Inclusion criteria were the patients older than 18 years, traumatic perforation larger than 25% of the pars tensa who visited within 3 days after injury. Subjects were excluded if there was total perforation, the history of otitis media, TM remnant with myringosclerosis, middle ear infection or hyperplasia of granulation tissue at the initial hospital visit, or ossicular disruption suspected by endoscopical examination or imaging study. The assessment of the history of otitis media was based on the patient’s oral presentation and endoscopic examination. Age, sex, duration, cause, side, and inverted edge were recorded during the first hospital visit. Each patient was endoscopically examined after cerumen and/or blood clots in the external auditory canal (EAC) were removed. The TM was photographed at the same time using a digital video camera, and the perforation size was recorded using ImageJ software(NIH, Bethesda, MD, USA) and expressed as a percentage of the entire TM area. 17 A large perforation was defined as a perforation larger than 25% of the pars tensa (PT) 18 . However, as healing of a perforation is always associated with successful closure of the air-bone gap,1,3,5,19 we didn’t obtain audiometric data.
Sample size and Randomization
For calculation of the sample size, the study was powered at 80% and a type I error of 5% (α = 0.05) was used. A 10% difference of closure rates between the treatment groups was predicted. Using these values for the calculation, it was determined that 17 patients are required in each study arm. 19 Considering a 20% loss to follow-up, a total of 90 participants will be sufficient for randomization.
The principal investigator, aided by a registered nurse, allocated patients to various treatments, using simple random sampling. Specifically, consecutive subjects who met the inclusion criteria and signed the consent form were assigned random numbers generated by the SPSS for Windows software package (version 19.0; SPSS, Inc., Chicago, IL, USA) that allocated them to one of the control group of observation only, VG, and gelfoam patch alone groups.
Technical Methods
All the techniques were completed endoscopically in the hospital outpatient settings.
Control Group
No intervention was offered, but all patients underwent regular follow-up.
Vaseline Gauze Group
The EAC was cleaned with a cotton bud soaked in 0.1% povidone-iodine solution. A modified vaseline gauze
Gelfoam patch alone group
The EAC was cleaned with a cotton bud soaked in 0.1% povidone-iodine solution. A dry modified compressed Gelfoam sheet alone
Follow-Up
Follow-up was scheduled weekly until complete closure was achieved, or for up to 3 months. VG and Gelfoam were removed and a fresh piece was replaced at each visit. The TM was examined endoscopically at all follow-up visits. The perforation closure was evaluated based on the color photographs by an independent blinded clinician.
Statistical Analyses
Results are given as mean ± standard deviation or as a percentage. For statistical analysis of the results of the 3 groups, 1-way analysis of variance or Kruskal–Wallis testing was performed for continuous data, and the χ2 test was used for categorical data. A2-sample t test or the Mann–Whitney U test was used to compare the results of 2 groups. A P value of < .05 was considered to indicate statistical significance. Statistical analyses were carried out using SPSS software (version 11.0 for Windows; SPSS, Inc).
Results
Demographics Data
Demographics Data of Control, VG, and Gelfoam Alone Groups.
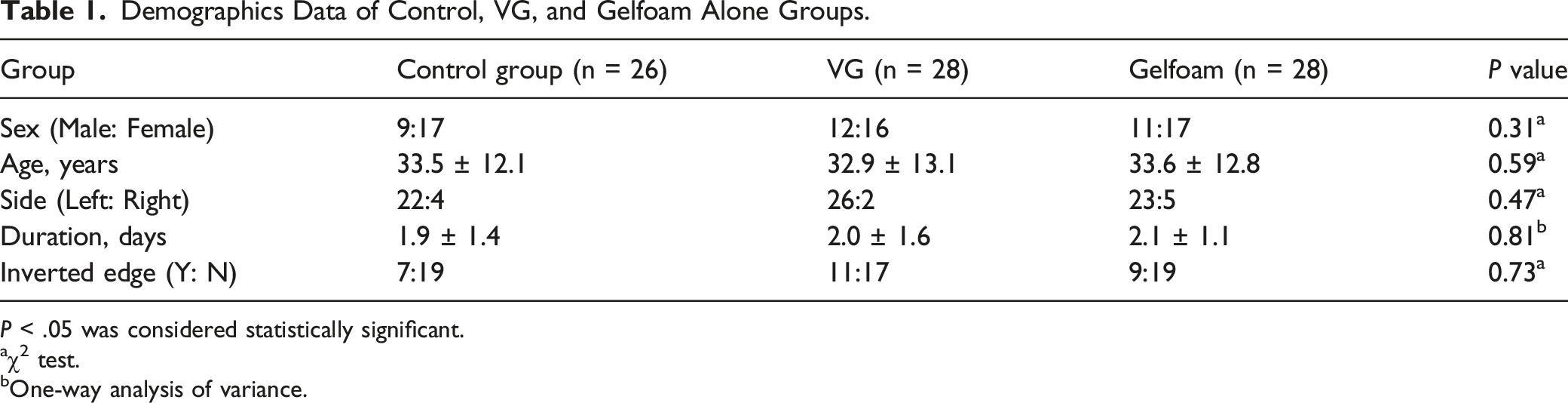
P < .05 was considered statistically significant.
aχ2 test.
bOne-way analysis of variance.
The Closure Outcome Among 3 Groups.

P < .05 was considered significant.
aχ2 test.
bOne-way analysis of variance.
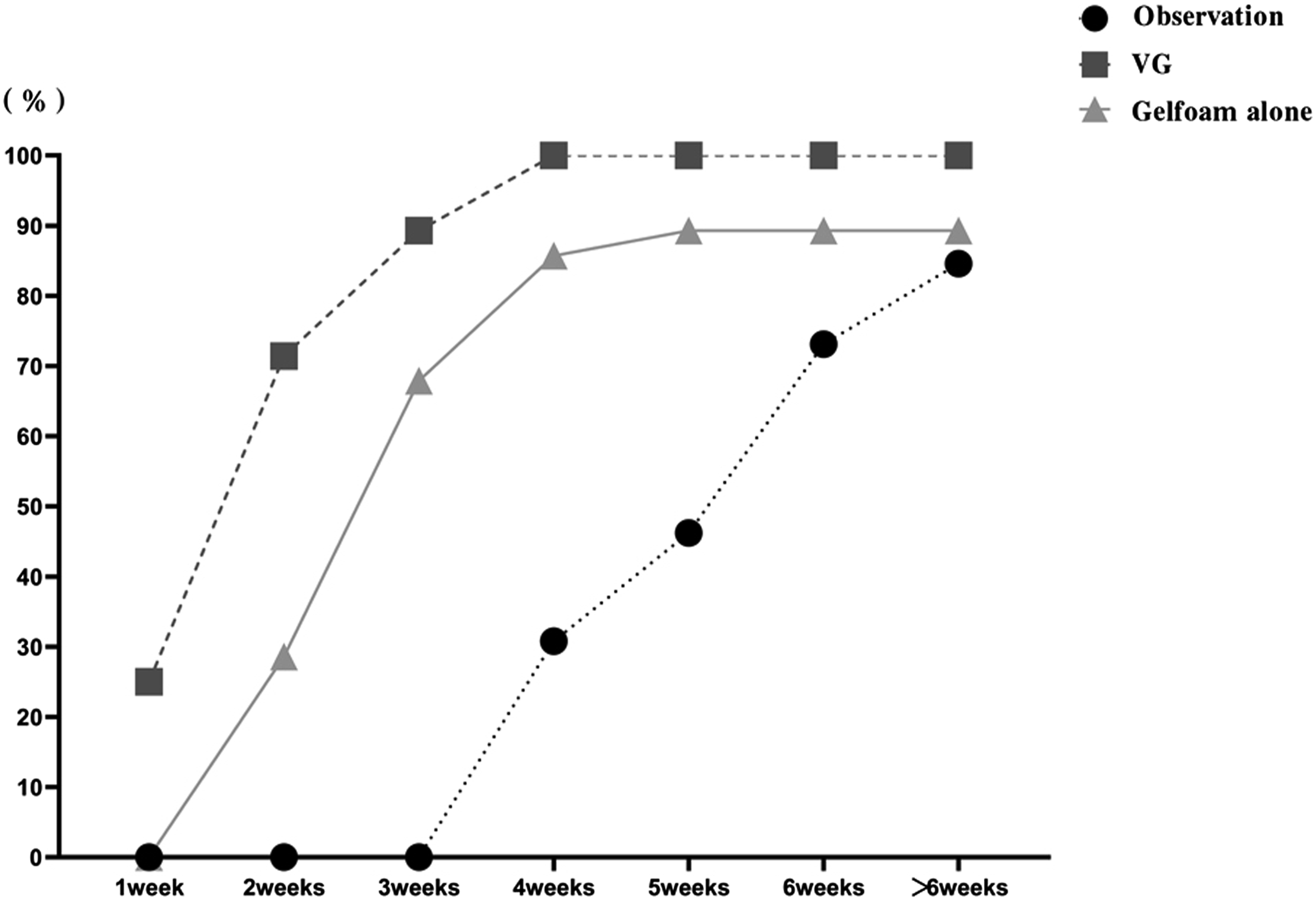
The closure rate at different time points among 3 groups.
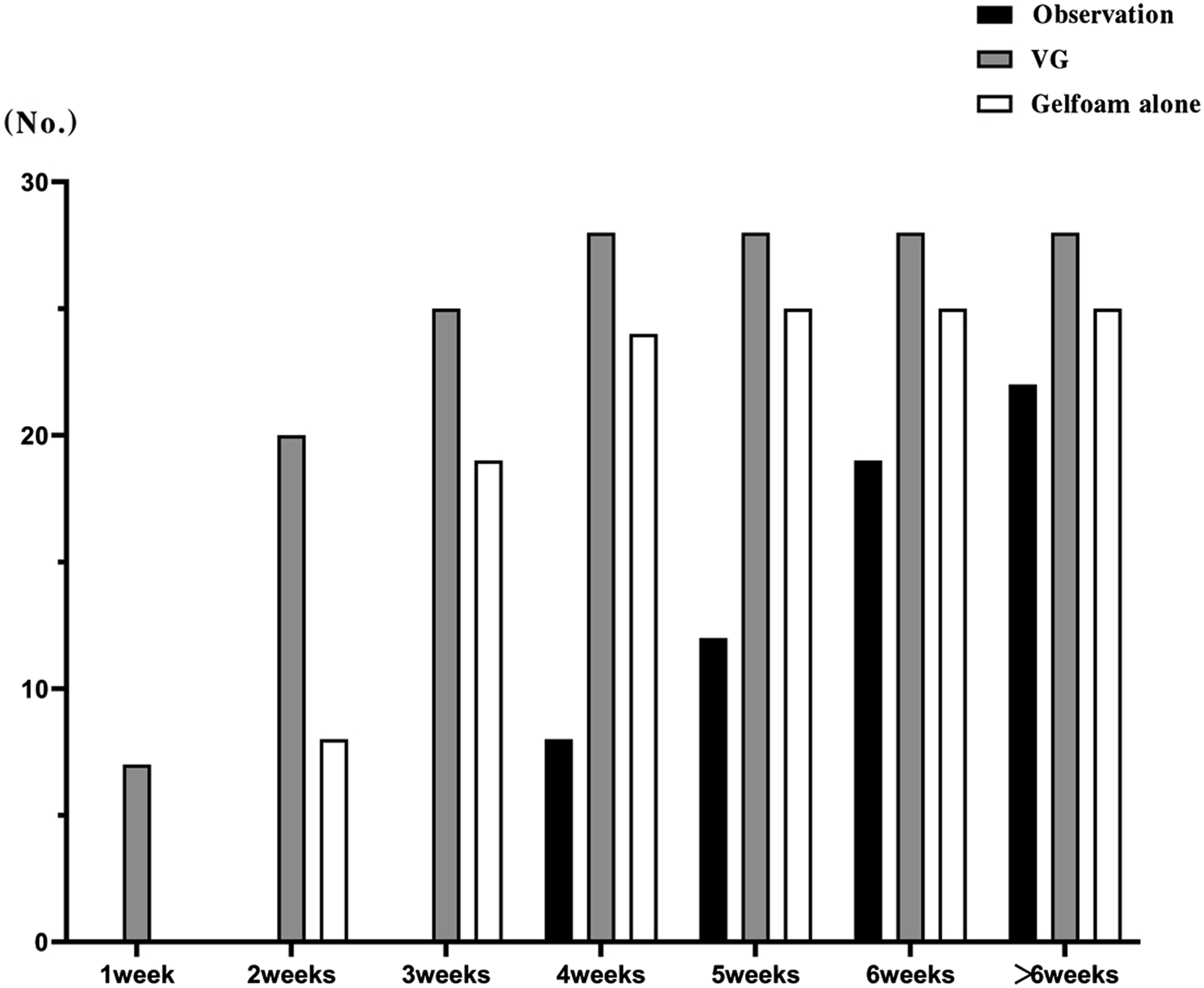
The closure number at different time points among 3 groups.
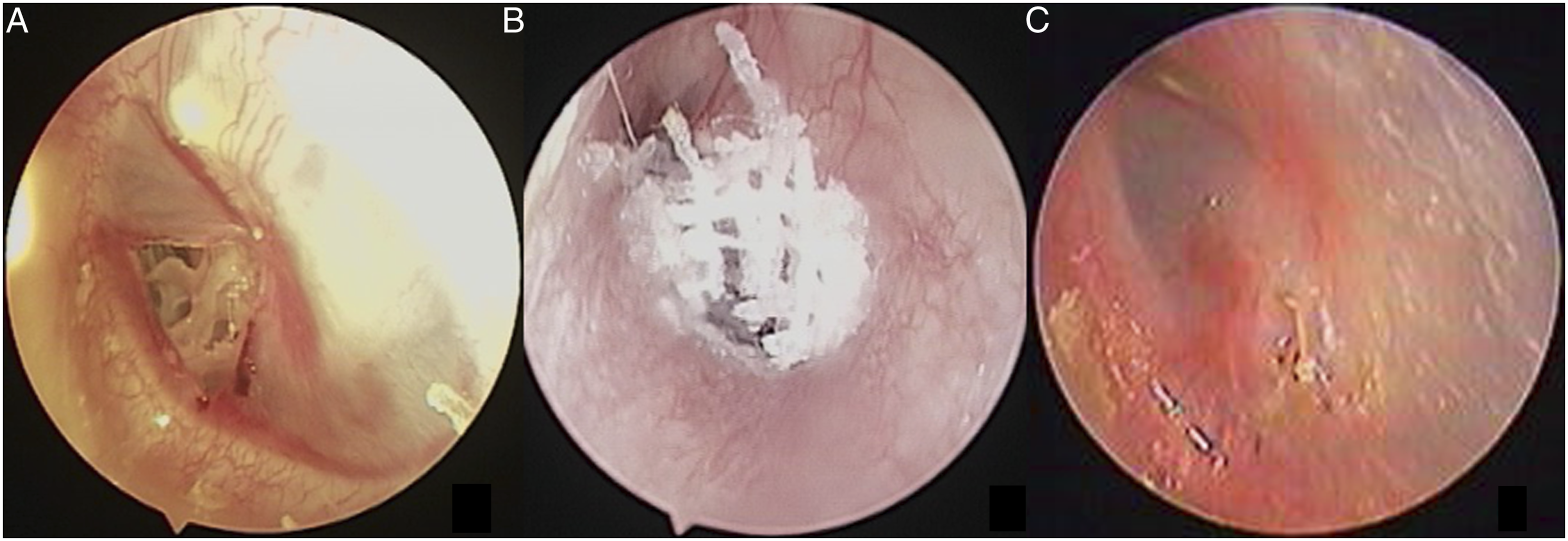
The mean closure times were 5.41 ± 1.47, 2.14 ± 0.93, and 3.00 ± 0.62 weeks for the control, VG, and gelfoam patch groups, respectively. The closure times among the 3 groups were significantly different (P < 0.001) (Figure 3 and Figure 4). Post-hoc multiple comparisons showed that the difference was significant between the control and VG groups (P < 0.001) or gelfoam alone group (P < 0.001) or VG and gelfoam groups (P < 0.05). The mean closure time among 3 groups. A 48-year-old female. Two days after perforation (A), vaseline gauze patch treatment (B), one week after treatment (C).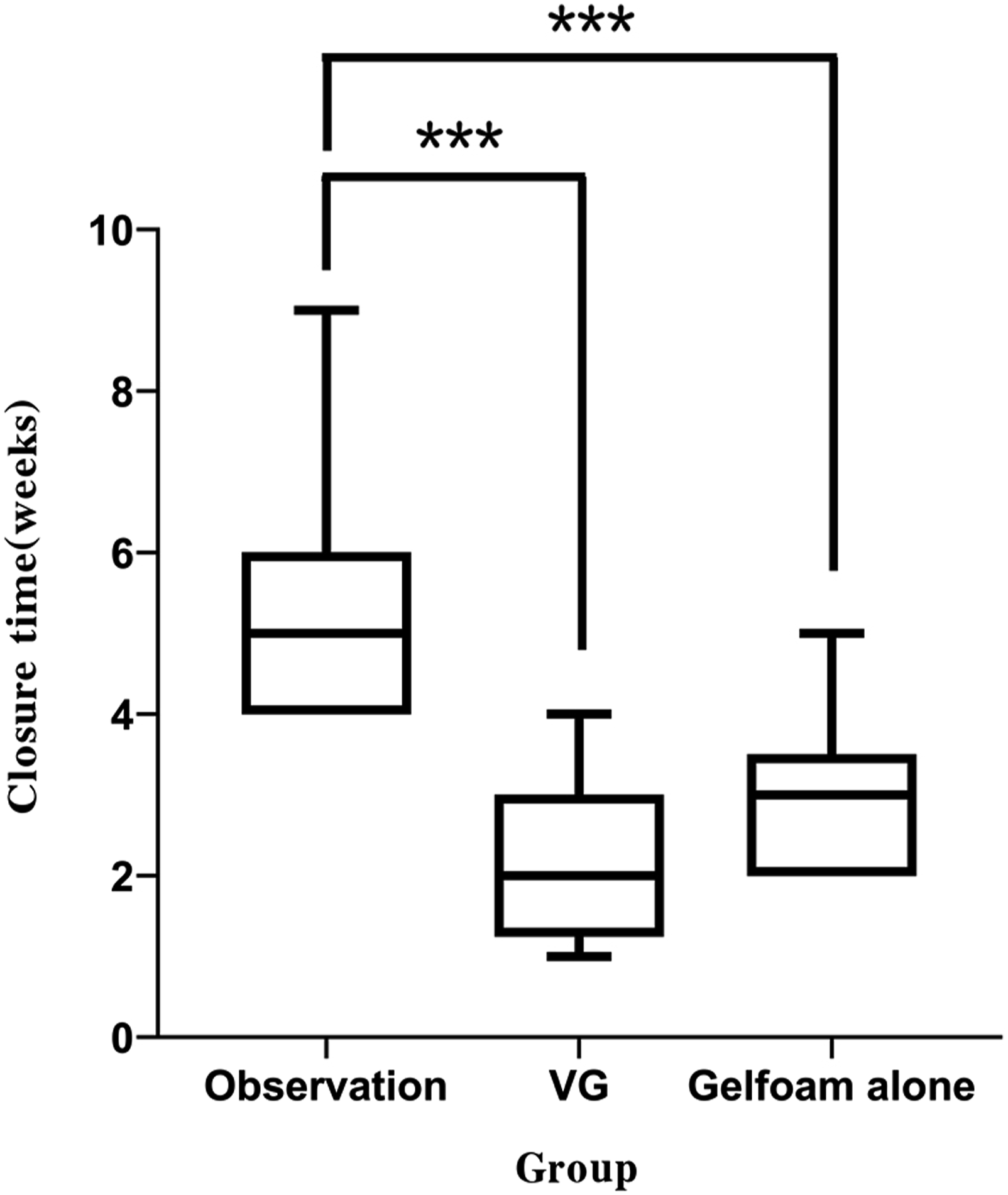
Discussion
Although traumatic perforation of TM tends to spontaneously heal, most of the perforations require long healing time, and a few large perforations almost fail to heal in the clinic.1,2 On the other hand, some symptoms of traumatic perforations (including tinnitus and aural fullness) affected the patient’s life quality. In addition, bathing and hair washing would be limited because the patients worry about the water entering into the ear and inducing middle ear infections. Thus, the patients demand to seek medical intervention to close the perforation early. The common intervention included paper patching, 3 gelfoam patch, 4 followed by egg shell 5 and Steri-Strips patch. 19 However, it only shortened the closure time but did not improve the closure rate.3-5,19 In recent times, novel biological scaffold materials had been sustainably developed by some scholars, including vivosorb and epifilm, 6 collagen scaffold 7 and acellular dermal allograft patch, 8 and bacterial cellulose, 9 which had been experimentally demonstrated to facilitate the TM healing and improve the closure rate.6-8 Nevertheless, they had not been widely applied in the otology clinic because of indeterminacy of biological properties and expensive costs.
Vaseline gauze is known as a lubricant and the common biological materials in otolaryngology, which is used for the nasal and ear packing;14-16 its advantage is readily available and inexpensive. This study suggested that the VG group significantly improved the closure rate and shortened the mean closure time compared with only observation group. In addition, although the VG group didn’t improved the closure rate, it significantly shortened the mean closure time. VG possesses the moisture-retention ability and can reduce the pain and prevent synechia formation.10,11 The application of VG created a moist environment of perforation margins. The moist environment is critical to wound healing, 20 which can prevent the further necrosis of tissue and crust formation at the edges. In addition, moist environment facilitates the action of growth factors, cytokines, and chemokines. This promotes cellular growth and collagen proliferation. In addition, a moist wound increase in available nutrients and reduction in evaporative loss make the micro-metabolic balance favor repair, thereby accelerating the TM healing.20-22
Recent clinical application also demonstrated that ofloxacin ear drops created a moist environment and accelerated the healing of TM perforations. 23 The experimental study of burn wound suggested that VG could facilitate the granulation tissue growth and accelerate the wound healing. 13 Wang XF et al. 12 believed that VG provides an appropriate microenvironment for cell migration and wound healing. In addition, the gauze of VG adhesion to perforation margin not only keeps the perforation margins in the same plane but also acts as the scaffold of epithelial migration and prevents the outward migration of epithelium. Some studies showed that crust and outward migration of epithelium at the edges resulted in the failure and delayed closure.24,25
Gelfoam is a dry biological material, which hasn't moisture-retention ability for the perforation margins. Gelfoam only acts as the scaffold of epithelial migration and keeps the centripetal migration of proliferating epithelium but does not create the moist environment of perforation margins. Unfortunately, gelfoam lacked the adhesive capacity and was detached from the TM after sneezing, coughing, yawning, shaking one’s head, chewing, or swallowing. Gelfoam would not effectively act as a scaffold for epithelial migration once it was detached from the perforation. In this study, all the patients experienced gelfoam detaching from the TM at least once during follow-up period. Clinically, gelfoam combined with antibiotic ointments was suggested to repair the traumatic perforation. 26 The study of wound healing suggested that VG has no toxic side effects,12,13 however, its ototoxicity is unknown. Nevertheless, VG adhered to the surface of perforation margin, which was almost impossible to enter into the middle ear and cause the ototoxicity. The drawback of this study was small sample. A large perforation was defined as a perforation larger than 25% of PT rather than 50% of PT in this study. In addition, this study performed the follow-up once a week and didn’t accurately evaluate the closure time; some perforations may have been closed before follow-up time point. Thus, we should perform the follow-up every other day or every three days to more accurately compare the closure time in future.
Conclusion
VG improved the closure rate and shortened the closure time compared with observation only, which could be an effective patch material for repairing traumatic lager perforations in the outpatient setting, which is readily available and convenient.
Footnotes
Author Contributions
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Health Commission of Zhejiang province, China (Grants#2021KY1186). None of the authors have any conflict of interest to declare.
Ethical Approval
The study protocol was reviewed and approved by the Institutional Ethical Review Board of Yiwu central hospital. Written informed consent was obtained from all participants.
Data Availability statement
Data for this study are available on request.