
Abstract
Objective
Hypoglossal nerve stimulation (HNS) implantation in the US requires preoperative drug-induced sleep endoscopy (DISE) screening for complete concentric palatal collapse (CCC) to establish treatment candidacy. We hypothesized that supine pharyngeal width (SPW) in awake patients is associated with CCC and HNS therapy outcomes.
Methods
Adults with moderate to severe obstructive sleep apnea underwent awake measurement of SPW followed by DISE screening for CCC. Eligible patients electing for HNS implantation underwent postoperative polysomnography per standard of care.
Results
SPW was measured in 73 patients. For SPW >20 mm, the positive likelihood ratio for absence of CCC was 6.67 with pre- and post-test odds of 6.3 and 42.0, respectively. Postoperative PSG data were available from 31 of 44 (70.5%) patients subsequently implanted with HNS. Patients with SPW >20 mm had a greater rate of HNS response than those with SPW ≤20 (62 vs 30%; P < .05). Only SPW and BMI were significantly associated with CCC and HNS response in regression models.
Conclusion
In a retrospective cohort study, SPW was significantly associated with CCC and postoperative apnea-hypopnea index following HNS implantation. SPW may be a viable screening tool for HNS candidacy.
Keywords
Introduction
Obstructive sleep apnea (OSA) is a prevalent condition with moderate to severe OSA affecting approximately 10% of adults and is associated with an increased risk of motor vehicle and workplace accidents 1,2 as well as cardiovascular morbidity and mortality. 3 Treatment is recommended to reduce subjective symptom burden as well as long-term morbidity and mortality from associated comorbid conditions. 4 -6 Continuous positive airway pressure (CPAP) is the current first-line treatment 5,7 but patient adherence to therapy is problematic. 8 Hypoglossal nerve stimulation (HNS) therapy was approved by the US Food and Drug Administration (FDA) in 2014 for select CPAP-intolerant patients with moderate to severe OSA.
Drug-induced sleep endoscopy (DISE) screening to rule out complete concentric palatal collapse (CCC) is required to establish HNS candidacy. 9 Pivotal trial inclusion criteria originated in turn from early phase studies demonstrating decreased HNS therapy response in patients with CCC. 10,11 Nevertheless, DISE is time-consuming, expensive, requires general anesthesia, and only has moderate inter-rater reliability for assessment of palatal collapse patterns. 12 -15 Furthermore, CCC is only a partial predictor of HNS treatment response, as current selection criteria yields response rates of 66–75%. 9,16
We hypothesized that greater supine pharyngeal width (SPW) is associated with a lower probability of CCC during DISE after anecdotally observing that HNS-eligible patients with wider pharynges while laying supine and awake less frequently had CCC. We further hypothesized that greater SPW associates with a greater probability of HNS therapy response.
Methods
This study was a retrospective, single-center cohort study approved by the HonorHealth Institutional Review Board of the HonorHealth Research Institute (1793148-1).
Participants
Included patients had met standard clinical, demographic, and polysomnographic criteria for HNS eligibility and undergone DISE as part of their routine clinical care with a single surgeon (JW). Baseline polysomnography was completed with either in-laboratory (PSG) or home sleep apnea testing (HST) within the 24 months preceding consultation. SPW was measured during the initial office consultation (described below) but was not used for clinical decision-making.
DISE was performed using propofol sedation as previously described to evaluate for CCC per routine clinical care, 11 meaning a single unblinded rater (JW) documented the results but did not record the examination. A propofol infusion was continuously titrated intraoperatively to maintain flow-limited inspirations with a bispectral index score target of 65–75. The palatal scoring description from the VOTE classification was used to assess CCC status. 17 Patients without CCC who elected for HNS surgery underwent subsequent implantation of the Inspire HNS system (Inspire Medical Systems, Inc., Golden Valley, MN).
Data Analysis
Variable Definitions
The main independent variable was SPW. Secondary independent variables included demographic and polysomnographic factors known to associate with outcomes of interest, including preoperative apnea-hypopnea index (AHI), body mass index (BMI), age, and gender. 18,19 The primary dependent variables were CCC status and, in patients without CCC electing for HNS implant, postoperative AHI. Postoperative AHI represented the whole-night average number of respiratory events per hour from the first in-laboratory titration PSG.
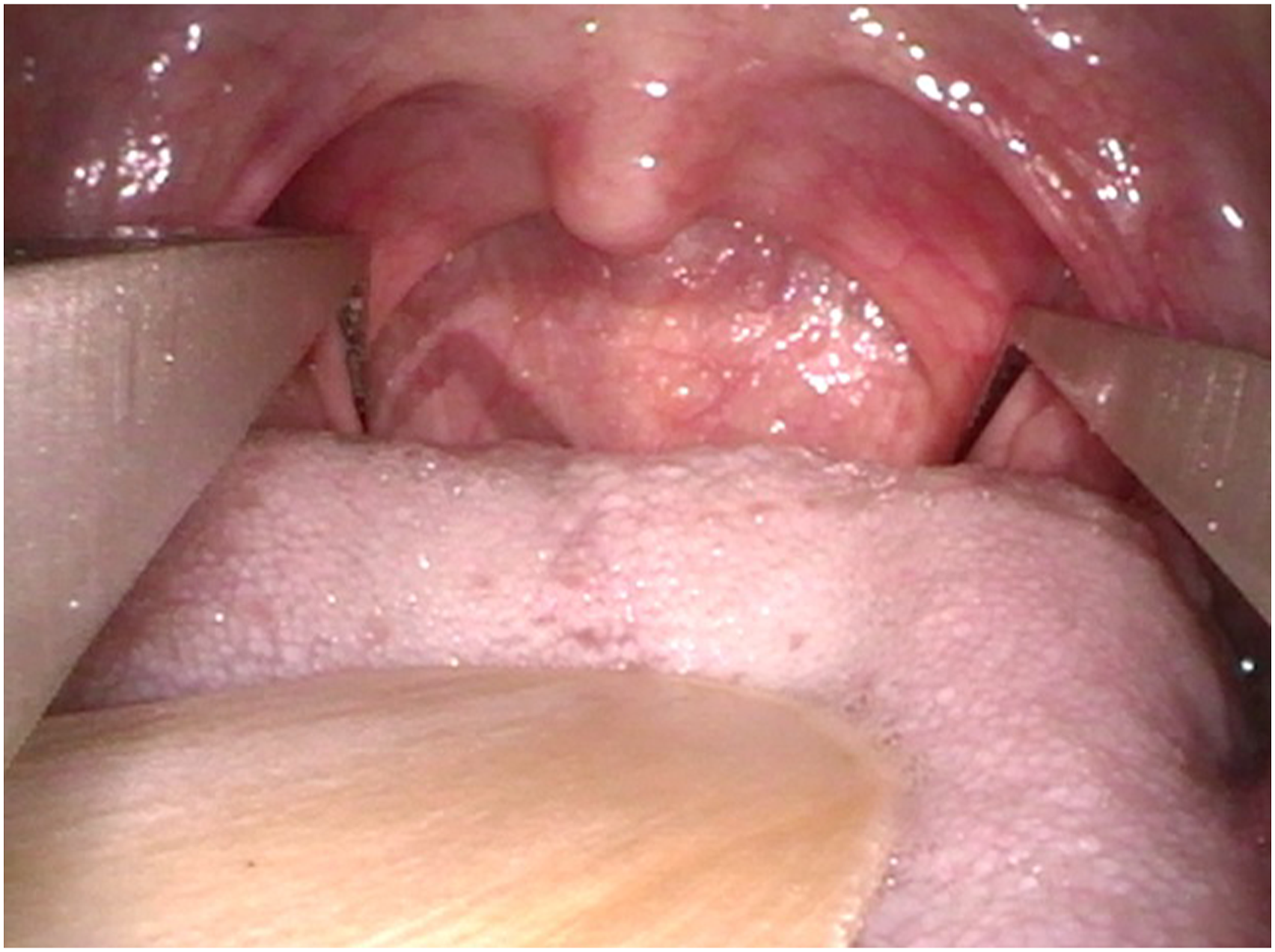
Supine Pharyngeal Width Measurement
Patients electing for DISE during their initial office consultation underwent SPW measurement with a Castroviejo caliper by a single surgeon (JW; Figure 1). The patient was laid supine and asked to breathe through the mouth without tongue protrusion to expose the palatopharyngeal arch of the soft palate. SPW was measured at the medial border of the posterior tonsillar pillar insertion into the lateral pharyngeal wall (Figure 2). If needed, a tongue depressor was used to aid visualization. If the patient gagged during the measurement, it was discarded and immediately remeasured during relaxed oral breathing as active muscle contraction from nasal breathing, gagging, or swallowing could potentially alter measurements. Castroviejo caliper used for measurement of supine pharyngeal width. Measurement of supine pharyngeal width. SPW was measured at the medial border of the posterior tonsillar pillar insertion into the lateral pharyngeal wall.
Statistical Analysis
Statistical analyses were designed to test the primary hypothesis that greater SPW is associated with a lower probability of CCC, and the additional hypothesis that greater SPW is associated with a greater probability of response to HNS therapy using the Sher criteria (postoperative decrease in AHI >50% and AHI <20).
Student’s t test, Barnard’s Exact Test, and analysis of variance (ANOVA) testing were used to assess for differences in clinical variables between patient cohorts. Bootstrapping is a statistical technique frequently used with sparse datasets to increase data density for statistical analyses by repeatedly and randomly resampling the underlying dataset. A receiver operating curve analysis was conducted to estimate the median sensitivity and specificity of SPW at different cutoff thresholds for CCC status and HNS response using 2000 bootstrap replicates to generate 95% confidence intervals (95% CI). Barnard’s Exact Test was used to assess for differences in HNS response rates at the final selected SPW threshold. Binary logistic and linear regression models were evaluated in a stepwise fashion to assess the association between the independent variables, CCC status, and postoperative AHI. Statistical significance was inferred throughout at a P value <.05. All statistical tests were completed in the R statistical programming language (version 4.1.2). 20 A priori power calculations could not be completed for this pilot study as there were no preexisting data regarding supine pharyngeal width effects on HNS outcomes to make assumptions regarding effect size.
Results
Complete Concentric Palatal Collapse Analysis
Baseline Characteristics of Patients Undergoing Drug-Induced Sleep Endoscopy.
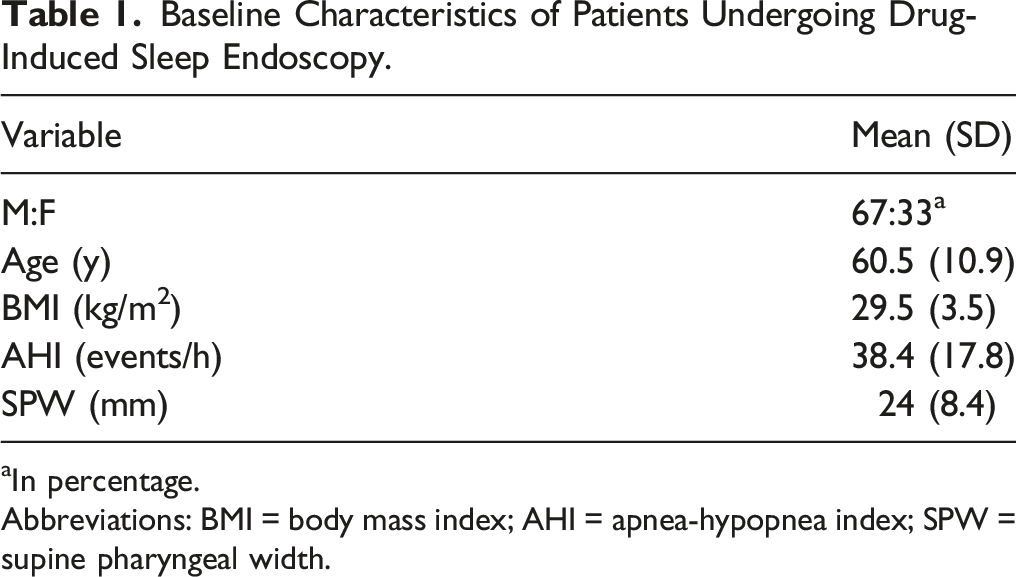
aIn percentage.
Abbreviations: BMI = body mass index; AHI = apnea-hypopnea index; SPW = supine pharyngeal width.
Mean Baseline Characteristics of Patients With and Without Complete Concentric Palatal Collapse (CCC) During Drug-Induced Sleep Endoscopy. Standard deviations in parentheses.
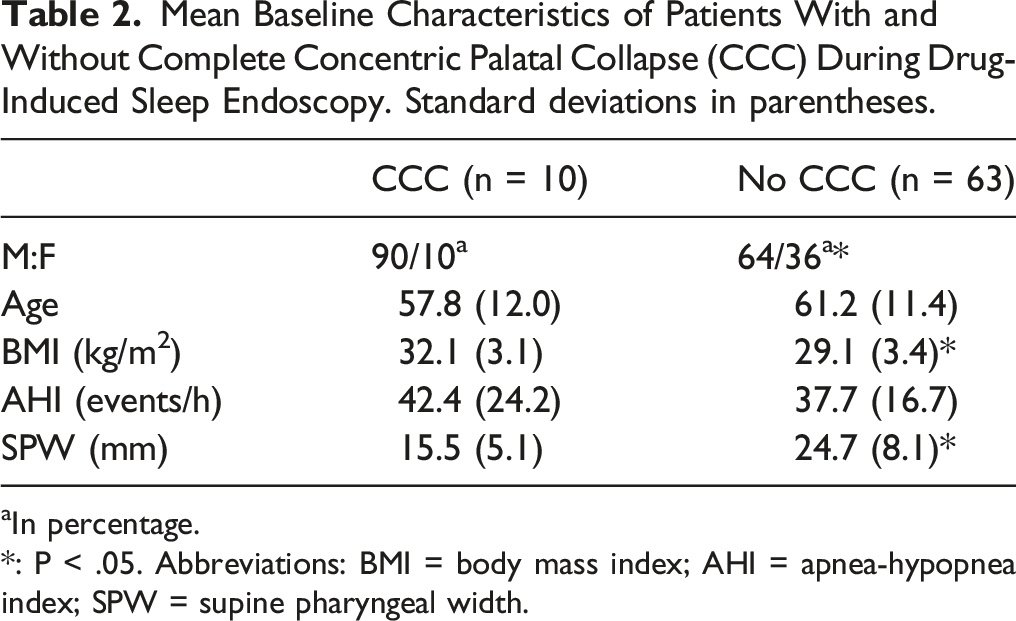
aIn percentage.
*: P < .05. Abbreviations: BMI = body mass index; AHI = apnea-hypopnea index; SPW = supine pharyngeal width.
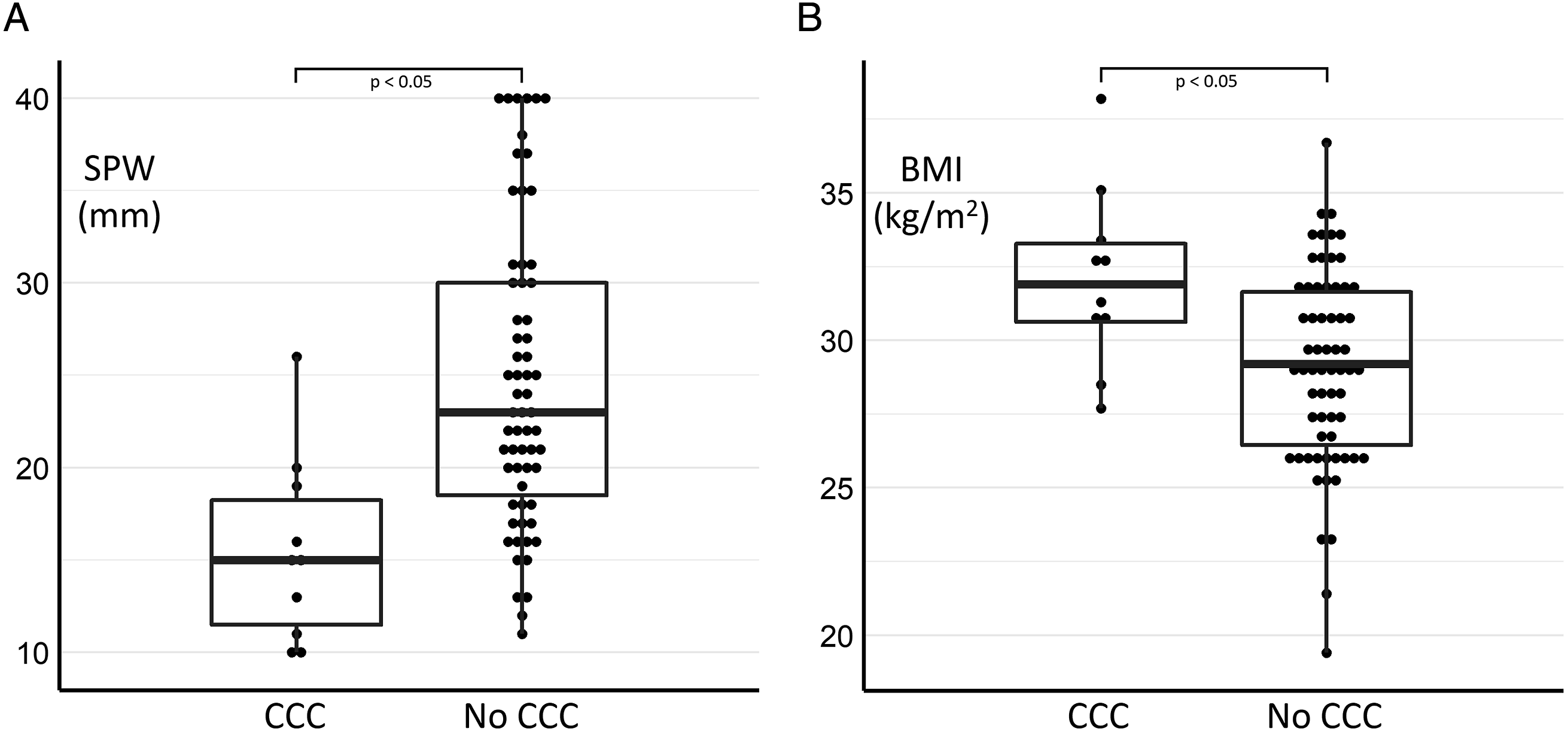
A. Supine pharyngeal width (SPW) and B. body mass index (BMI) measurements in patients with and without complete circumferential palatal collapse (CCC). Data are depicted as median (line), interquartile range (box), and whiskers showing outliers for each group, with patient counts for different values as dots.
The receiver operating characteristic curve analysis (Figure 4) had an area under the curve of .88. SPW >20 mm yielded a median sensitivity and specificity of .67 [95% CI: .54 – .78] and .90 [95% CI: .7 – 1.0] for absence of CCC, respectively. Forty-three (58.9%) patients had SPW >20 mm, with a positive likelihood ratio (LR+) of 6.67 for absence of CCC. All patients in this study had pretest odds of 6.3 for non-CCC during DISE, but the patients with SPW >20 mm had post-test odds of 42.0 for absence of CCC. Patients with SPW >20 mm did not differ significantly in age, BMI, preoperative AHI, or neck circumference from those with SPW ≤20 mm. Receiver operating characteristic curve analysis for supine pharyngeal width (SPW) and complete circumferential palatal collapse (CCC). SPW >20 (black circle) had a sensitivity of .67 and specificity of .9 for absence of CCC.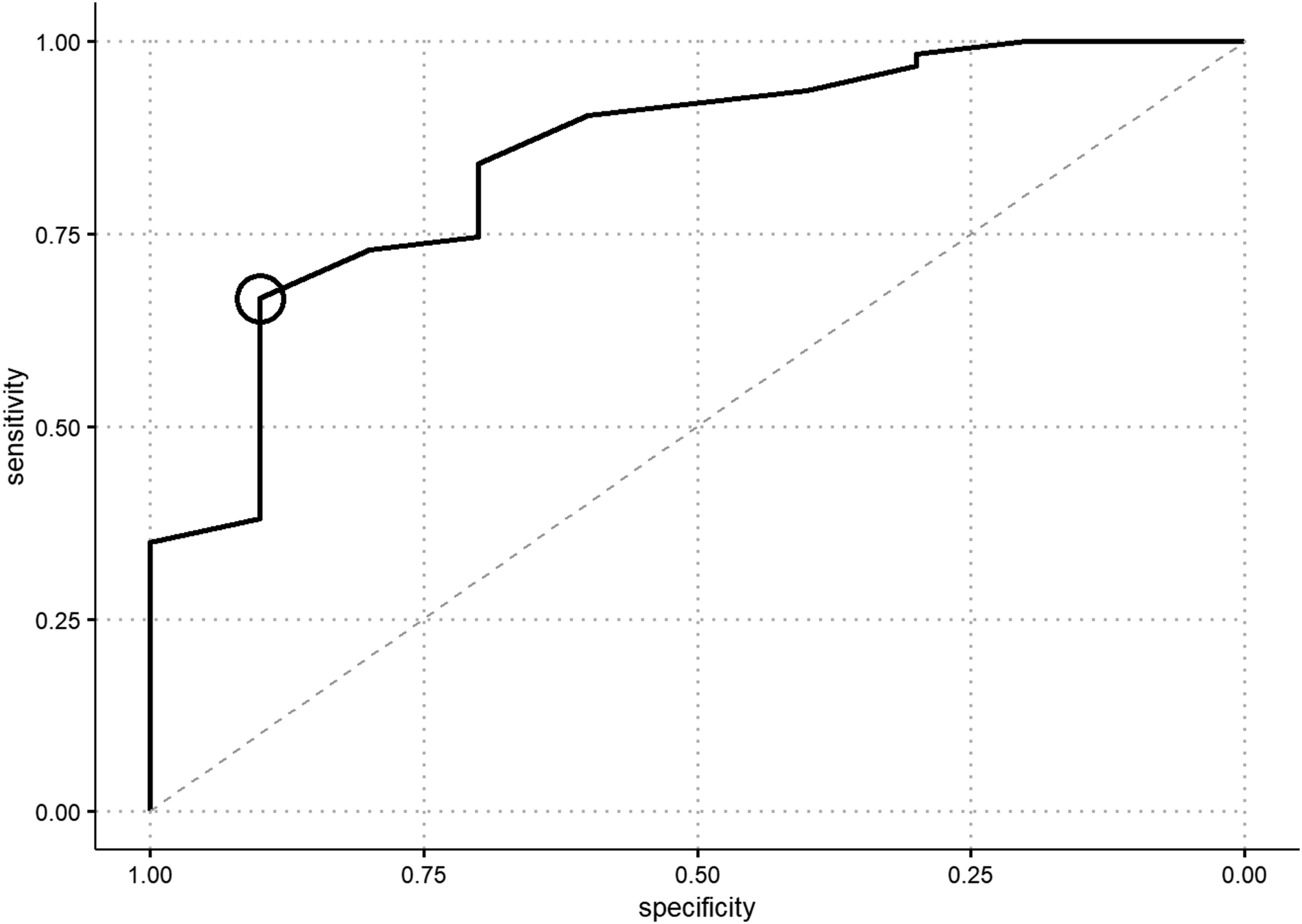
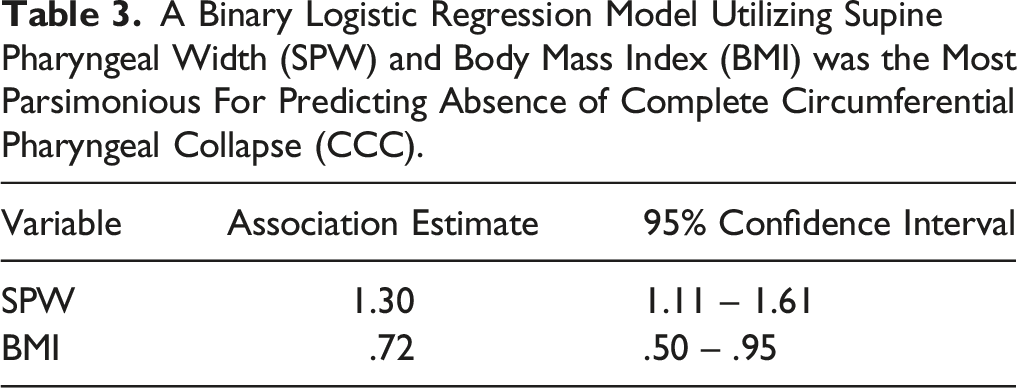
A Binary Logistic Regression Model Utilizing Supine Pharyngeal Width (SPW) and Body Mass Index (BMI) was the Most Parsimonious For Predicting Absence of Complete Circumferential Pharyngeal Collapse (CCC).
HNS Response Analysis
Mean Postoperative Apnea-Hypopnea Indices (AHI) and Sher Therapy Response Rate (postoperative AHI <50% and AHI <20 events/h) for Implanted Patients With Supine Pharyngeal Width >20 and <20 mm. Standard deviations in parentheses.

*: P < .05.
Mean Baseline Characteristics of HNS responders and Non-Responders. Standard deviations in parentheses.
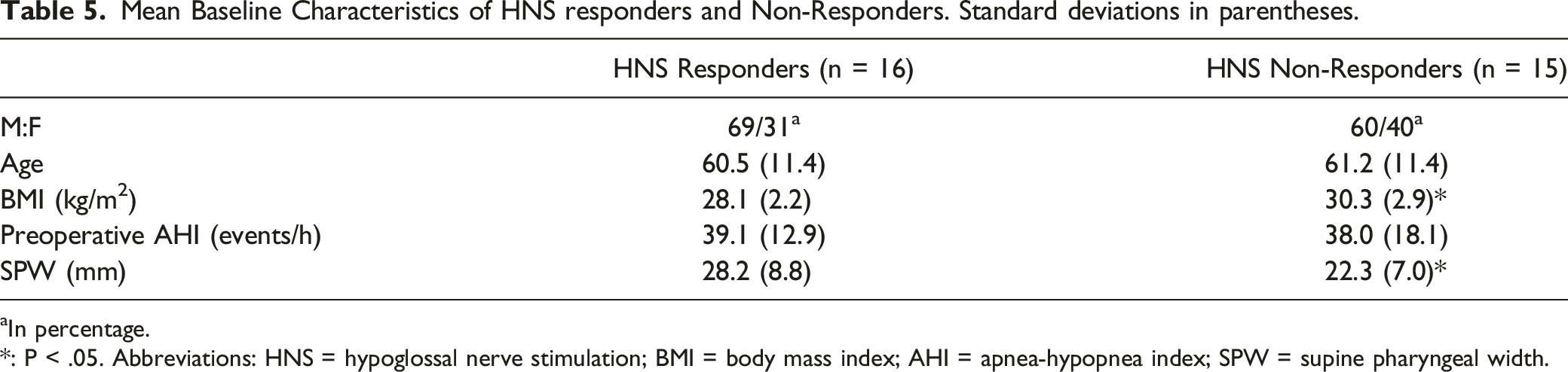
aIn percentage.
*: P < .05. Abbreviations: HNS = hypoglossal nerve stimulation; BMI = body mass index; AHI = apnea-hypopnea index; SPW = supine pharyngeal width.
SPW was significantly associated with AHI outcomes in a univariate linear regression model (P = .017), whereas BMI was not (P = .07). Stepwise elimination of the least significant independent variable determined that the most parsimonious model for predicting AHI outcomes was the univariate SPW model, in which each millimeter increase in SPW was associated with a .72 events/hr decrease in AHI (95% CI: 1.30 – .14). Additionally, SPW was the only variable significantly associated with AHI outcomes across each model (P < .05). Variance inflation factor testing did not exceed 1.1 for SPW in any model, suggesting only modest collinearity with other examined variables.
Discussion
This study demonstrates that supine pharyngeal width associates with CCC status during DISE. In non-CCC patients implanted with HNS, supine pharyngeal width additionally associated with HNS therapy response. Moreover, SPW independently predicted CCC status and HNS therapy response in regression analyses of independent variables previously associated with HNS outcomes.
Other studies have attempted to predict CCC using tools outside of DISE. Steffen et al found that BMI correlated with CCC, with a specificity of .71 at BMI >32 kg/m2, and .81 at BMI >35 kg/m2. 21 Moving beyond anthropomorphic measurements, Yalamanchi et al. examined the relationship between endoscopy findings with supine volitional snore vs DISE. 22 Based on their reported findings, the specificity of volitional snore for absence of CCC was .66. We found a greater specificity of .90 for absence of CCC using SPW >20 mm in this study. DISE costs are estimated to range between US$2,861 and US$7,942, 12 and CCC is currently the only exclusionary finding for HNS candidacy. A test that sufficiently increases the pretest probability for the absence of CCC might reduce healthcare costs by reducing the need for DISE evaluation in every patient.
Others have sought to correlate clinical or polysomnographic findings to HNS response with variable success. An early HNS feasibility study found that BMI <32 kg/m2 and AHI <50 events/h were associated with therapy success, leading to the HNS implant candidacy requirements for the STAR trial. 10 Retrospective analyses of larger patient cohorts found that thinner, older, and female patients tended to be more successful with HNS therapy, although no clear thresholds for patient selection were reported. 18,19 Conversely, Huntley et al found no significant differences in HNS response rates between those with BMI <32 kg/m2 and those with BMI of 32–35 kg/m2. 23 A more recent analysis of a large, international multicenter registry demonstrated a similar reduction in AHI between patients with BMI <32 kg/m2 and BMI 32–35 kg/m2 although a reduced percentage of patients in the latter group were Sher responders. 24 Lee et al reported that a mean therapeutic CPAP pressure <8 cmH2O had a high specificity for HNS response (.96), but a relatively low sensitivity of .39 that might eliminate many potential HNS therapy responders from implant candidacy. 25 Schwab and colleagues found that HNS non-responders had greater soft palate volume as measured by computed tomography, but no threshold analyses were performed. 26 SPW was significantly different between HNS responders and non-responders in this study, whereas other previously predictive variables from larger cohorts including age, gender, and BMI did not. Further prospective research is required to ascertain whether SPW carries valuable prognostic information regarding potential HNS response, although the substantial differences in mean postoperative AHI and Sher response rates between the two groups in this study suggest that it may.
The physiologic mechanisms underpinning the associations between SPW, CCC, and HNS response are unclear. HNS dilates the airway by protruding the tongue, but anterior displacement of the soft palate best associates with HNS success. 27,28 HNS effects on the retropalatal space are thought to be due primarily to mechanical anterior traction on the palate, as the hypoglossal nerve does not innervate any of the palatal muscles. CCC at the level of the soft palate is currently a contraindication for HNS therapy due to a lack of therapeutic response in early feasibility studies, 10,11 which suggests that a lateral collapsing component of the velopharynx may be less sensitive to the anterior displacement forces of HNS therapy. A large multicenter study found that complete lateral oropharyngeal wall collapse during DISE was associated with lower odds of HNS response compared with patients with partial or no lateral collapse, 29 supporting the concept that laterally collapsing elements of the airway may ultimately be less responsive to HNS. We propose two separate possible explanations for the increased likelihood of CCC we observed in patients with lower SPW. The first is normal velopharyngeal soft tissues but an underlying maxillary deficiency that creates a lower baseline SPW such that even a small degree of lateral velopharyngeal collapse during DISE is more likely to create the visual phenotype of CCC. The second is an increased collapsibility of the lateral velopharyngeal soft tissues leading to a lower SPW even when the underlying maxillary width is sufficient, which may explain some of the association between BMI and SPW in our data. Regardless of the underlying mechanism, we posit that the anterior-posterior increase in retropalatal space from HNS does not sufficiently make up for the narrow lateral dimension of the airway in low SPW patients. Further study is necessary to elucidate whether the correlations between SPW, CCC, and HNS response observed in this small cohort are generalizable to a larger population, and what the underlying mechanisms of action may be.
Several limitations of this pilot study must be acknowledged. First, data were collected in an unblinded fashion by a single examiner and DISE video was not recorded, preventing assessments for intra- and inter-rater variability in DISE scoring and introducing the potential for examiner bias. Nevertheless, SPW independently associated with CCC status monotonically, suggesting a true relationship between the two. Second, other levels of the pharyngeal airway, such as the oropharyngeal lateral walls, were not assessed during DISE. Further study will be required to assess whether SPW correlates with other DISE findings. Lastly, postoperative AHI was recorded from the initial tPSG and was additionally missing for a subset of implanted patients. We have intentionally reported the full-night AHI to avoid introduction of bias from a partial-night “titration AHI,” and we suspect that full-night AHI from a suboptimal night in the laboratory might underestimate HNS efficacy achieved by patients after further device adjustment. Our independently managed sleep laboratory was also not able to provide patient-specific documentation for missing tPSG data, which might unintentionally bias our results. A prospective, multi-institutional study is currently being planned to validate SPW measurements across multiple examiners and a broader patient population, which should also help to mitigate potential bias from loss-to-follow-up.
In office measurement of SPW is easy, rapid, and inexpensive, and this pilot study suggests it may be predictive of CCC status and ultimately HNS therapy response. Further study is required to assess the true relationship between SPW, CCC status, and HNS response rates, and in what patients it may provide valuable prognostic information.
Footnotes
Author’s Note
This manuscript was not previously presented.
Acknowledgments
The authors thank Eahsan Shahriary, Ph.D., University of Arizona College of Medicine-Phoenix for assistance with statistical analyses. Drs. Weiner and Kent have both received support from Inspire Medical Systems, Inc. for sponsored research unrelated to this manuscript. Inspire Medical Systems, Inc was not involved in the conception, study design, data analysis, or preparation of this manuscript.
Author Contributions
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Jordan S. Weiner- Inspire Medical Systems (consultant); David T. Kent- Inspire Medical Systems (research support), Invicta Medical (consultant), and Nyxoah (scientific advisory board, patent royalties).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability
The participant-level data presented herein will be made available upon reasonable request to the corresponding author.