
Abstract
Patients with vertigo and facial nerve palsy as initial symptoms are rarely diagnosed with multiple sclerosis. A 43-year-old woman presented to our department with symptoms of vertigo and right facial nerve palsy (Yanagihara 16-point system [total score, 40] or House– Brackmann grade IV [obvious facial weakness]). On the day of the visit, she presented with right eye abduction, left eye adduction, and complaints of diplopia. Based on magnetic resonance imaging findings, she was diagnosed with clinically isolated syndrome, which is an early manifestation of multiple sclerosis. She was treated with intravenous methylprednisolone. Otolaryngologists often suspect Hunt’s syndrome in patients who present with facial nerve palsy combined with vertigo. However, herein, we report our experience with an extremely rare case of a patient with atypical nystagmus symptoms, eye movement disorder, and diplopia secondary to facial palsy and vertigo, who presented with a clinical course different from that of Hunt’s syndrome.
Introduction
Otolaryngologists often suspect Hunt’s syndrome in patients who present with facial nerve palsy combined with vertigo. However, herein, we report our experience with an extremely rare case of a patient with atypical nystagmus symptoms, eye movement disorder, and diplopia secondary to facial palsy and vertigo, who presented with a clinical course different from that of Hunt’s syndrome. Moreover, we indicated the uniqueness of this course and summarized the previously reported cases of multiple sclerosis with facial paralysis and vertigo. Further, we reported the case of a patient with multiple sclerosis, with facial paralysis and vertigo as the initial presentation. In cases of peripheral facial nerve palsy, otolaryngologists should consider the possibility of ocular motility disorders to differentiate it from multiple sclerosis or other central disease. Right abducens nerve palsy and left adduction.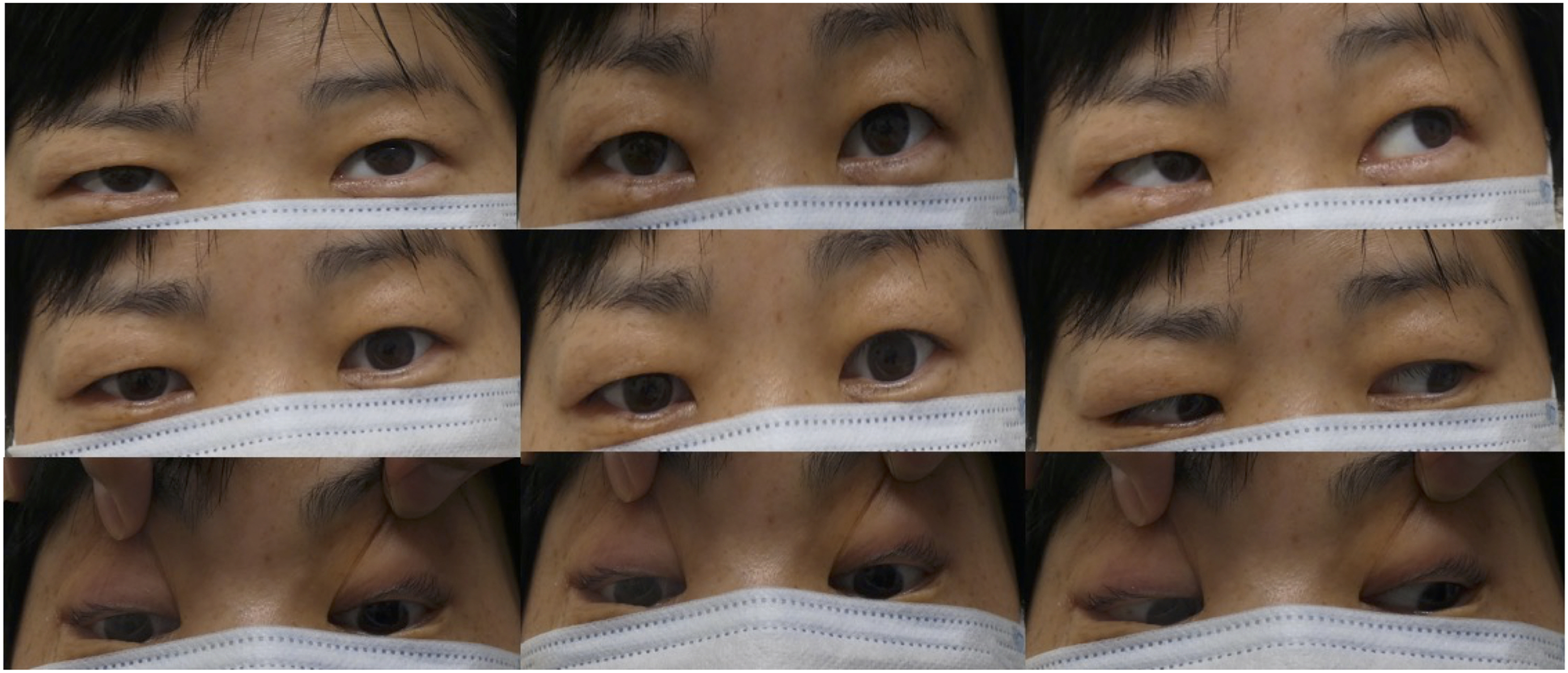
Case Report
A 43-year-old woman who had been experiencing dizziness since day 1 underwent magnetic resonance imaging (MRI) at her doctor’s office on day 3, but no significant findings were reported. On day 4, she experienced right facial nerve palsy and visited her doctor on day 5. On the same day, she was referred to our hospital for further examination. Our initial examination revealed right peripheral facial nerve palsy (Yanagihara 16-point system [total score, 40] or House–Brackmann grade IV [obvious facial weakness]). No significant nystagmus was observed. An auditory test revealed normal results. She was admitted to our hospital as she experienced relatively intense vertigo. MRI fluid-attenuated inversion recovery (FLAIR): hyperintense lesions in the right pontine tegmentum (arrow).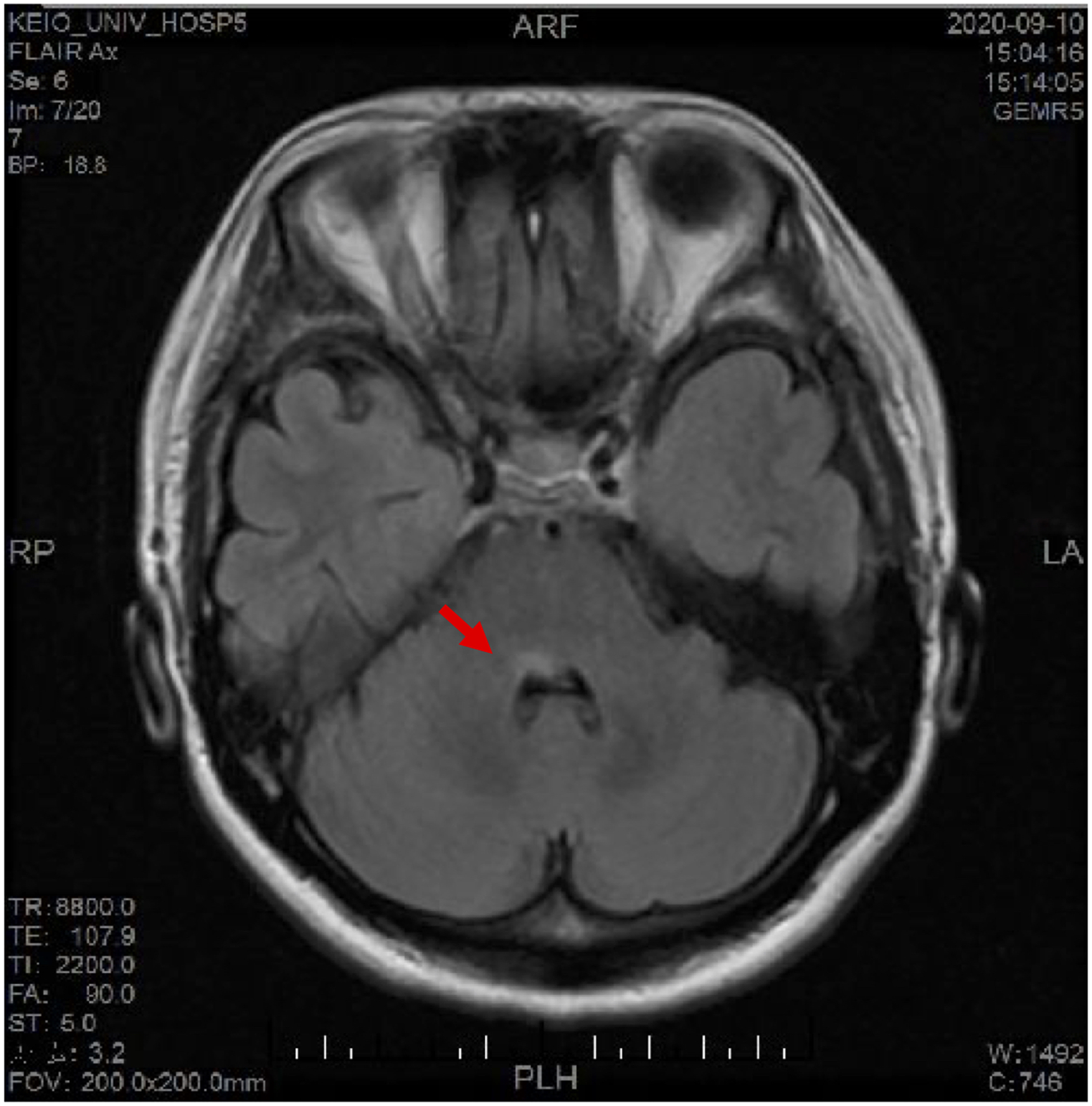
A 10-day tapered infusion of prednisolone (120 mg/day) and famciclovir (1500 mg/day) for 7 days was initiated after the diagnosis of zoster sine herpete. In the afternoon on the same day, she presented with right eye abducens nerve palsy, left eye adduction, and diplopia (Figure 1). Therefore, we performed MRI to evaluate the intracranial lesion. A hyperintense lesion was detected in the right pontine tegmentum using fluid-attenuated inversion recovery (Figure 2). Examination using a charge-coupled device camera revealed horizontal leftward nystagmus on abduction. Upbeat upward gaze nystagmus was noted.
Encephalitis or a demyelinating disease was suspected because of the progressive symptoms and hyperintense lesion in the pons. She was transferred to the neurology department on the same day, and intravenous methylprednisolone pulse therapy was initiated. She showed improvement in the Yanagihara test score to 36 points on day 11, and neurologic examination on day 12 revealed significant improvement in both eye movements.
Discussion
The oculomotor nucleus (III), trochlear nucleus (IV), and abducens nucleus (VI), which control eye movements, are located in the pons. The facial nucleus (VII) is located in the proximity of the pons. Because of the proximity of these nuclei, demyelinating lesions of the brainstem are often associated with facial nerve palsy and eye movement disorders. 1 The symptoms of vertigo appeared initially in this patient. The mechanism of the vertigo was strongly associated with deep perceptual–spinal motor systems, which are responsible for equilibrium, and visual–oculomotor movements. The vestibular labyrinth interferes with these 2 systems. The network including the vestibular labyrinth is defined as the vestibular system, which is responsible for maintaining balance. In this patient, demyelinating lesions were mainly located around the vestibular nucleus and paramedian pontine reticular formation (PPRF). We believe that the impaired equilibrium caused vertigo.
The appearance of upbeat nystagmus may be attributed to a disturbance of the supranuclear mechanism, leading to disturbances of conjugate eye movements and neural integrators, thus resulting in an inability to maintain eye position. 2 PPRF generates horizontal oculomotor velocity signals and causes horizontal eye movements. 3 The vestibular nucleus acts as a neural integrator and alters the positional signal to maintain eye position. 4 In this case, the demyelinating lesion mainly involved the PPRF and vestibular nuclei. Therefore, we believe that the disruption of these lesions caused difficulty in maintaining eye position, resulting in gaze palsy and horizontal nystagmus.
Clinically isolated syndrome (CIS), a demyelinating symptom, is considered a prodromal manifestation of multiple sclerosis. The McDonald criteria are often used for the diagnosis of multiple sclerosis. The 2017 McDonald criteria are used for evaluating patients experiencing a typical CIS; they define the dissemination in time and space for the diagnosis of lesions in the central nervous system. 5 Early treatment of CIS with a disease-modifying drug is known to suppress the transition to multiple sclerosis.6,7 The initial symptoms of CIS, such as facial nerve palsy and vertigo, are commonly observed in the otolaryngology department; thus, early diagnosis is crucial. Overall, 50%–70% of adult patients with CIS have multiple asymptomatic white matter brain lesions suggestive of demyelination, as determined using T2-weighted MRI. 8 Even if routine imaging is not recommended when Bell’s palsy is suspected, based on the guidelines for Bell’s palsy, 9 an aggressive MRI feature may help in ruling out multiple sclerosis and other central lesions when patients present with dizziness and eye movement disturbances.
However, in some cases, we cannot detect lesions during the initial period of CIS using MRI. In such cases, visual simulation tests, such as eye tracking and optokinetic nystagmus tests, may be effective.10,11 Although the incidence of cochlear paralysis is estimated to be approximately 13%–44%, 12 visual simulation tests may help in diagnosing CIS when the detection of the lesion is difficult using MRI.
Multiple sclerosis often presents with visual disturbances, numbness, and motor paralysis. It is rarely diagnosed during a visit to otolaryngology department.1,8 The incidence of peripheral facial nerve palsy in patients with multiple sclerosis is estimated to be approximately 0.2%.13,14 In addition, there is a low probability that multiple sclerosis is the cause of peripheral facial nerve palsy, considering the symptom of facial paralysis. A previous study reported that multiple sclerosis was the cause of peripheral facial nerve palsy in approximately 0.1% of patients with facial paralysis (n = 1989). 15 The findings of nystagmus are also diverse, and the appearance of nystagmus may vary depending on the location of the demyelinating lesion. 12 Here, we report the rare case of a patient with CIS who presented to our clinic with facial nerve palsy as the initial presentation. In addition, her lesion was located in the pontine tegmentum. It has been reported that infarction or demyelinating lesions of the pons may cause abducens and facial nerve disorders because nerve fibers from the facial nerve nucleus encircle the abducens nerve nucleus in the pontine tegmentum. 16 As there was no oculomotor disturbance at the time of the initial examination, it was considered important to not only observe nystagmus but also monitor oculomotor disturbance over time for symptoms such as dizziness and facial paralysis.
Conclusion
Otolaryngologists rarely suspect multiple sclerosis in patients who present with vertigo and facial nerve palsy. They should consider the possibility of ocular motility disorders in patients with peripheral facial nerve palsy to differentiate it from multiple sclerosis or other central disease. Moreover, it is essential to understand the importance of continued follow-up of patients with ocular motility disorders because of the possibility of a progressive condition.
Footnotes
Acknowledgments
We thank Dr Kenji Kufukihara and Dr Masahiro Katsumata (Department of Neurology, Keio University School of Medicine) for their helpful comments.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
Our institution’s Research Ethics Board does not require a review or approval for case reports. Our investigation is in accordance with the Code of Ethics of the World Medical Association (Declaration of Helsinki).