
Abstract
Hypopharyngeal fibroepithelial polyp is a rare entity. It could extend along the esophagus, leading to dysphagia. In rare cases, this polyp could present as airway compromise due to occlusion of the inlet of the larynx. The treatment of choice is surgical resection. Accurate defining of the origin of such polyp is mandatory in order to achieve complete resection and avoid recurrence. Although hypopharyngeal FEP is rare, physicians must keep this in mind when a patient presents dysphagia or airway compromise. In the current case, we present a rare case of giant hypopharyngeal FEP originating from the right pyriform sinus detected in a Caucasian female. The patient threw up the polyp after severe vomiting. This case should be the fourth and largest case of hypopharyngeal FEP reported in the literature.
Background
Fibroepithelial polyps (FEPs) are rare entities resulting from hyperplasia of fibrous connective tissue. 1 Most of them are seen in men between 40 and 70 years of age. 2 Fibroepithelial polyps are benign tumors and the rate of malignant transformation is low.1,3 These polyps are most commonly originating from the skin. However, some cases have been reported to arise from the mucosa of the oropharynx, hypopharynx, and oral cavity. 4 Hypopharyngeal FEP can vary significantly in size. It can grow slowly and extend along the esophagus leading to dysphagia. In some cases, it could be life-threatening due to obstruction and subsequent respiratory distress. In some rare situations, large polyps can cause asphyxiation if regurgitated or bleed.5,6 These lesions may manifest with dyspnea, choking, and sleep-disordered breathing. 7 In the present case, we reported a giant FEP originating in the right pyriform sinus. To the best of our knowledge, this is the fourth and largest case of hypopharyngeal FEP reported in the literature, making our case unique. We presented our patient along with the review of the current literature.
Case presentation
A 56-year-old Caucasian woman came to the emergency department shocked and afraid because a tissue mass was coming out of the mouth after severe vomiting. On examination, the patient was in a state of extreme fear and confusion due to the view of the mass, but was hemodynamically stable and systemically well. There was no stridor or dyspnea. The patient reported a history of foreign body sensation in her throat with difficulty swallowing solid food two months ago. She denied any symptoms of difficulty breathing or airway compromise. According to her medical records, the patient had a negative medical history, except for hypertension, which was medically controlled. Flexible fiber optic laryngoscopy was performed. We discovered a giant pedunculated polyp with a thin stalk originating from the right pyriform sinus. The polyp was extending from the pyriform sinus and protruding outside the mouth. The patient denied previous surgeries in the oropharynx, hypopharynx, or upper aerodigestive tract. Magnetic resonance imaging (MRI) revealed a giant mass arising from the right pyriform sinus with a thin stalk and extending out of the oral cavity. The mass was isointense in the T1-weighted images (T1WI) and hyperintense in the T2-weighted images (T2WI) (Figure 1). Laboratory tests were unremarkable. The larynx was not compressed by the polyp, therefore, the decision was made to remove the polyp through endoscopic laryngeal surgery under general anesthesia with endotracheal intubation (Figure 2). We moved the patient to the operating room. Using bipolar diathermy, the polyp stalk was coagulated and then resected. After resection, we performed a rigid pharyngoesophagoscopy that revealed complete resection of the mass. The patient was placed on a semi-liquid diet and discharged on the next postoperative day. A week later, the patient was re-evaluated by flexible fiber optic laryngoscopy and all findings were within normal limits. Axial T1-weighted (A) and T2-weighted (B) images show a lobulated mass originating from the right pyriform sinus with a thin stalk (yellow arrow) and extending out of the oral cavity (red arrow). The mass was isointense on T1WI and hyperintense on T2WI. Intraoperative photos.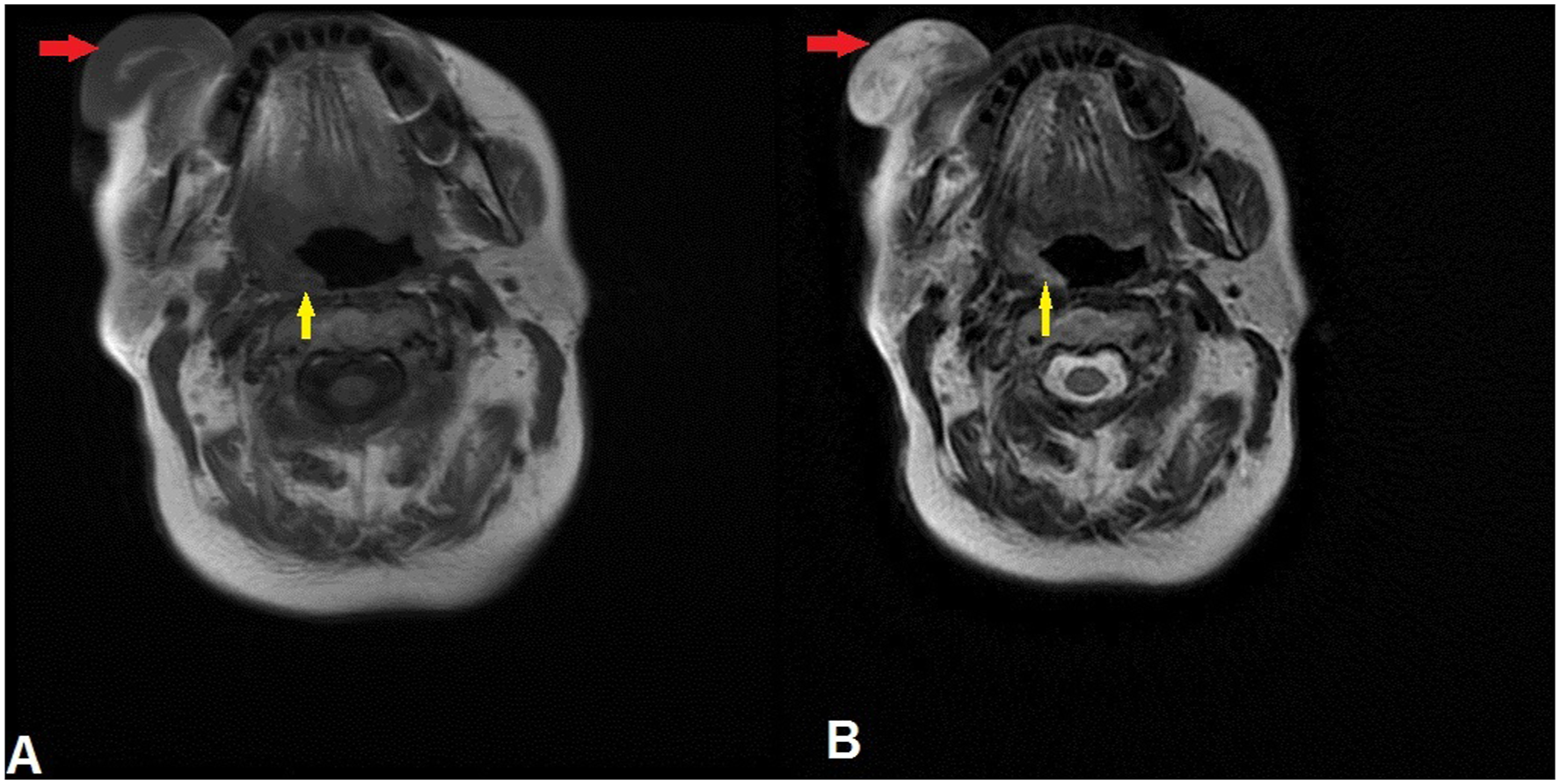

Pathological findings
Macroscopic examination showed a giant soft tissue polyp measuring approximately 21 × 4 × 5 cm. The specimen was sectioned and multiple sections were submitted for histologic examination. Microscopic examination revealed inflammatory changes covered with reactive hyperplastic squamous epithelium without neoplastic changes. The mentioned findings consist with benign FEP.
Discussion
Previous reported cases of hypopharyngeal fibroepithelial polyps.
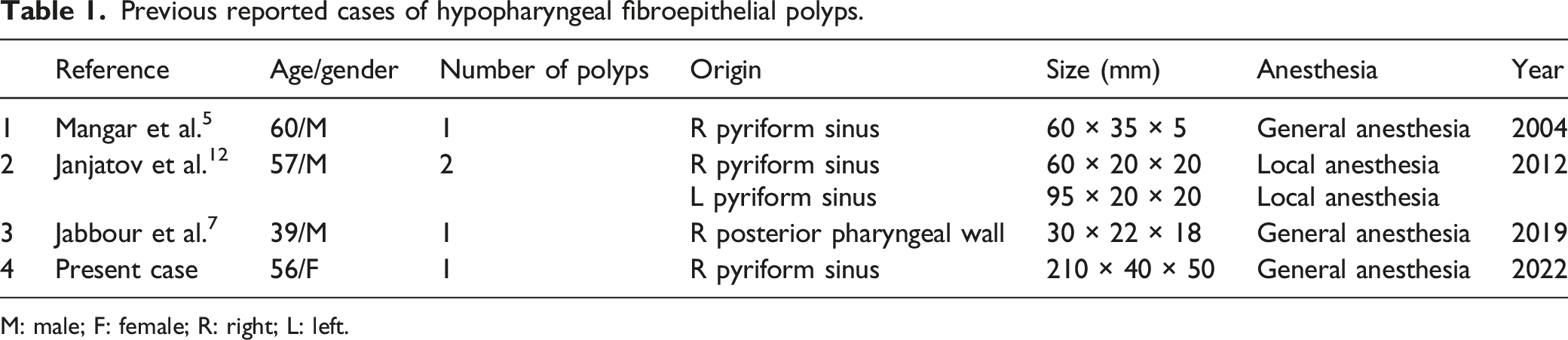
M: male; F: female; R: right; L: left.
Conclusion
Hypopharyngeal FEPs are extremely rare and those originating in the pyriform sinus are even rarer. Physicians should keep these cases on the list of differential diagnoses when complaints such as dysphagia or airway compromise are found. Surgical excision is the treatment of choice and should be performed as soon as possible to avoid sudden airway obstruction. When possible, general anesthesia is preferred to local anesthesia to accurately define the origin of its stalk, which is necessary to achieve complete resection of these lesions and decrease the rate of recurrence.
Footnotes
Acknowledgments
The authors acknowledge the patient and her family for their cooperation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Statement of informed consent
Verbal informed consent was obtained from the patient for their anonymized information to be published in this article.
Data availability
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.