
Abstract
Squamous cell carcinomas predominate in laryngeal malignancies, while spindle cell tumors, typically derived from non-epithelial tissues, are uncommon, accounting for 0.3%–1% of all malignant laryngeal tumors. Low-grade malignant myofibroblastic sarcoma (LGMS) is an extremely rare, atypical myofibroblastic tumor classified as a spindle cell tumor that primarily affects the head and neck region. There have been few reports in the literature regarding the LGMS of the larynx. LGMS of the larynx was discovered during a pathological biopsy. There was no recurrence during the 6-month follow-up after the total laryngectomy.
Introduction
Myofibroblastic sarcoma, also known as a myofibroblastic tumor, is a soft tissue tumor with myofibroblastic differentiation. WHO has recently classified low-grade myofibroblastic sarcoma (LGMS) as intermediate (occasionally metastatic) fibroblastic/myofibroblastic tumors.1,2 Because of the non-specific clinical manifestations of this tumor, the pathological diagnosis of LGMS is difficult, thus, increasing the rate of misdiagnosis and missed diagnosis. Our department diagnosed and treated a rare case of LGMS of the larynx, described below.
Case Report
A 48-year-old male patient had been complaining of hoarseness for six months. Electronic laryngoscopy revealed a pink mass with a smooth surface in the right vocal cord and subglottis, a grayish pseudomembrane on the surface of the left vocal cord, the disappearance of the laryngeal ventricle, fixation of the right vocal cord, and fair movement of the left vocal cord. On contrast-enhanced scans, neck CT showed cricoid cartilage destruction, soft tissue thickening of the laryngeal cavity, anterior commissure thickening, laryngeal ventricle stenosis, and significant heterogenous enhancement. The patient had more than 20 years of smoking history, with an average of one pack of cigarettes per day, and a drinking history of 5 years, with an average of 0.15 kg of liquor per day. After his admission, a biopsy under general anesthesia revealed spindle cell lesions and LGMS of the larynx. Immunohistochemistry showed that he was positive for vimentin and SMA markers, CD68 (partially positive) and Ki-67 (20% positive), but negative for CK, CK (5/6), p40, H-Caldesmon, Desmin, S-100, Melan-A, CD34, Melan-A, and CD34. According to neck CT, the patient was diagnosed with LGMS of the larynx, which had invaded the cricoid cartilage, and total laryngectomy was chosen.
LGMS of the larynx was the postoperative pathological diagnosis; the patient was discharged two weeks after surgery. Six months later, the patient was readmitted to the hospital for stenosis release due to post-tracheostomy stenosis, and the tumor indicators were reexamined, which revealed no recurrence or metastasis Figure 1. CT shows a tumor of the vocal cords, narrowing of the laryngeal compartment.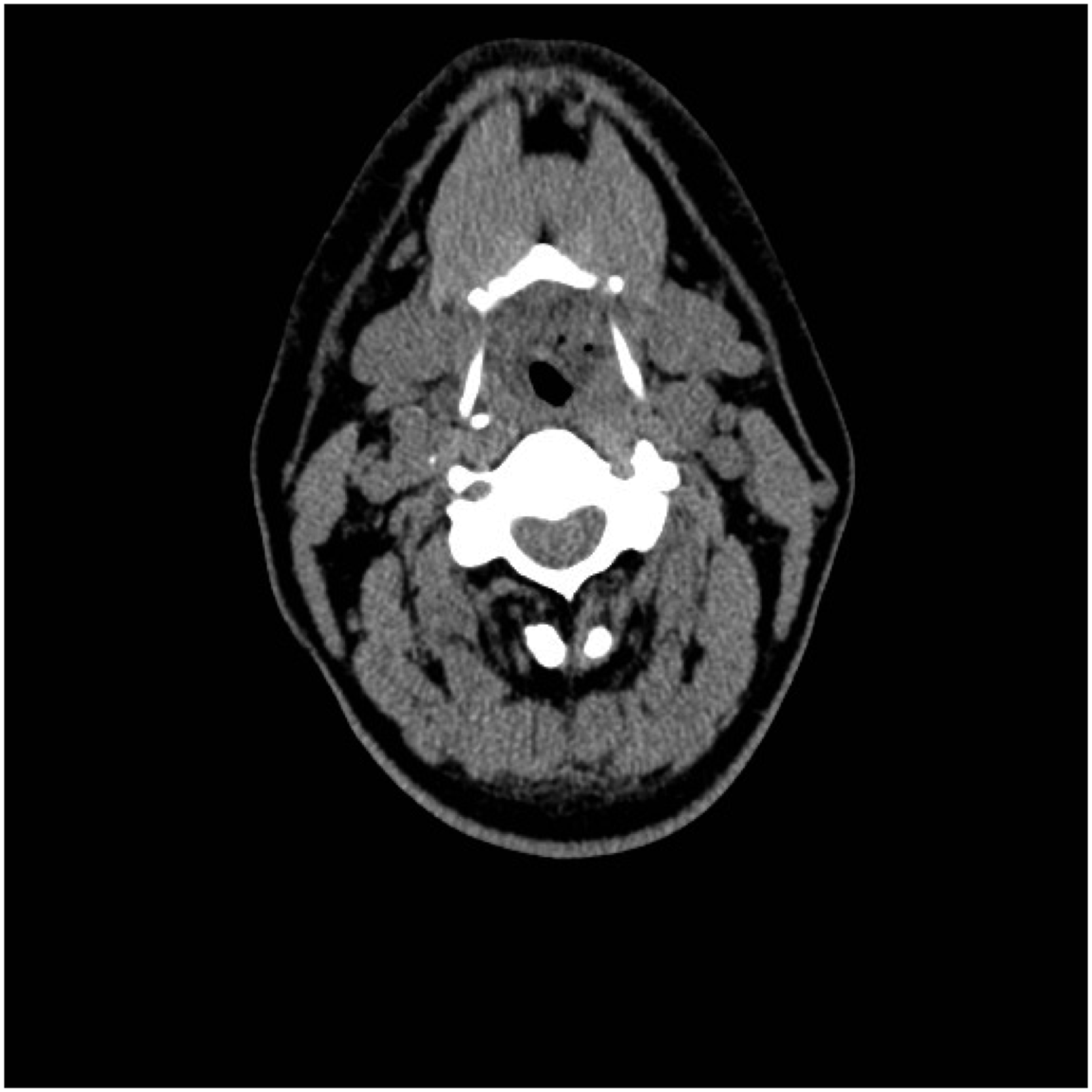
Discussion
More than 80% of malignant laryngeal tumors arise from squamous epithelium; thus, the incidence of mesenchymal tumors is low, with myofibroblastic sarcoma being extremely rare, and LGMS occurring in the larynx being rarely reported in the literature to date.
3
LGMS was first described in 1978 by Vasude et al.
4
then confirmed in 1998 by Mentzel et al.2-4 and finally recognized as a distinct entity after Montgomery et al. reported and described its morphological standard in 2001.
5
LGMS is a malignant mesenchymal neoplasm with myofibroblastic differentiation most commonly found in the head, neck, and extremities. The oral cavity (particularly the tongue) is the most commonly affected area. It has also been reported in the skin, breast, mandible, maxilla, face, paranasal sinuses, scalp, thyroid, and mastoid tissues.6-8 According to Hirotaka Yonezawa et al., LGMS accounts for approximately 51.5% of the head and neck region, 25.2% of the trunk, and 23.3% of the extremities Figure 2.
9
A:HE staining showed obvious atypia, spindle arrangement, eosinophilic cytoplasm and insignificant nucleoli. B: Desmin (negative) C: SMA (positive) D: Vimentin (positive).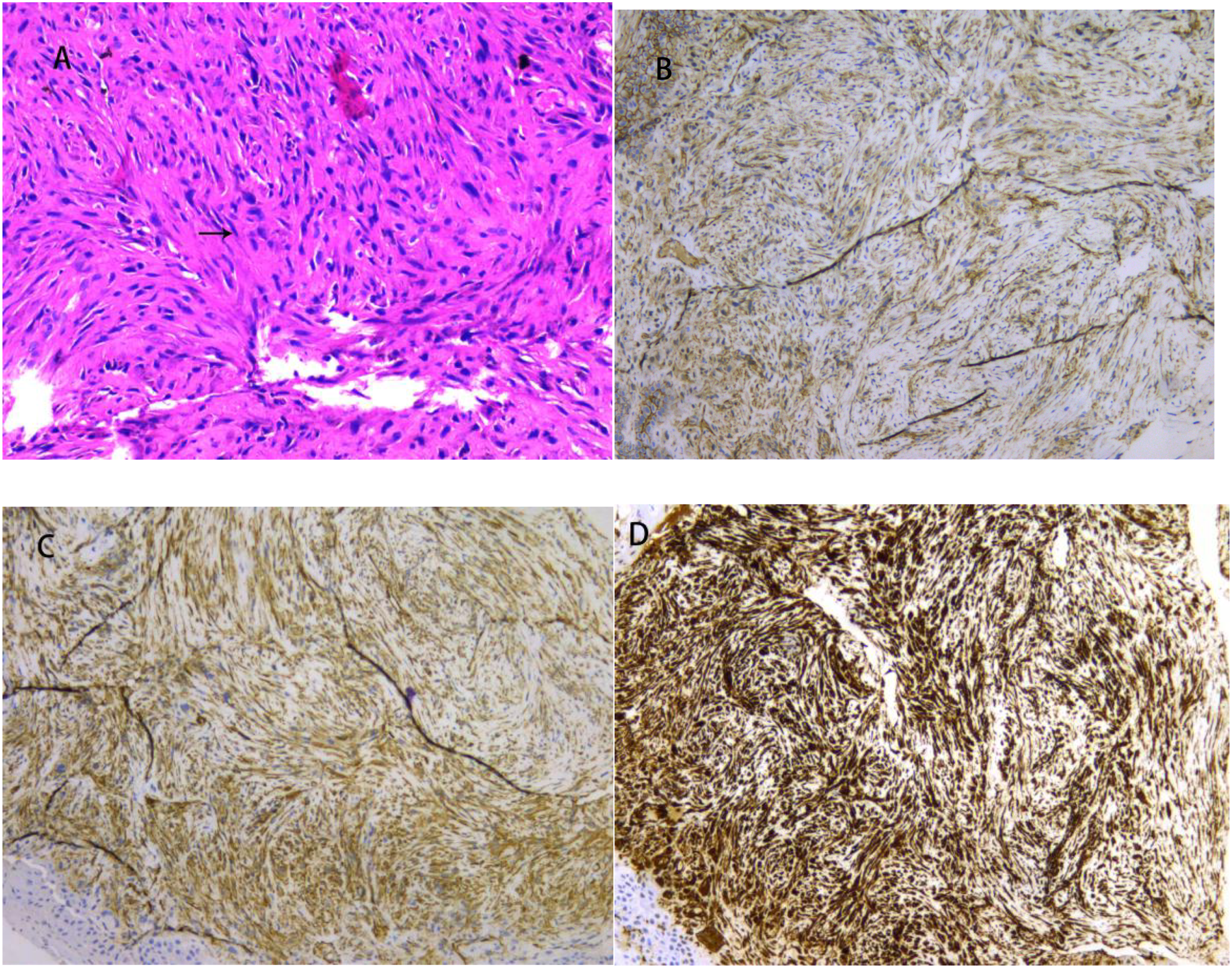
The optimal treatment regimen for LGMS is still unknown. According to the currently reported cases, surgery is the primary treatment modality for LGMS, with radiotherapy and chemotherapy being used less frequently. After surgical treatment, most LGMS patients have a good prognosis and a high survival rate, while radiotherapy and chemotherapy are only used in a small number of cases.10-12 Long Peng reported that a patient with LGMS of the pancreas had no recurrence after surgery and 2-week chemotherapy even after five years
13
; Tessho Maruyama proposed that the recurrence rate of LGMS cases after surgery alone is 18.8%, while the recurrence rate after surgery plus radiotherapy is 71.4%, demonstrating that postoperative radiotherapy for LGMS may contribute to tumor recurrence
14
; According to Xueling Wu, LGMS rarely invaded the thoracoabdominal membrane and multiple organs of the head and neck, and the patient survived well after symptomatic treatment without surgery, indicating that LGMS is not highly malignant Figure 3.
15
Total laryngeal (including tumor) specimen.
LGMS is difficult to diagnose and may be misdiagnosed as a benign and malignant tumor because it is uncommon in clinical practice and typically manifests as a painless, progressively enlarging mass. As a result, it needs to be distinguished from certain myofibroblasts or benign diseases, such as fibromatosis, nodular fasciitis, and other pseudosarcomas. LGMS is primarily diagnosed through the pathological identification of myofibroblasts using light microscopy and immunohistochemistry. Using light microscopy, myofibroblasts can be seen as large and spindle-shaped, with long cytoplasmic processes, taking up the light stain with cytoplasmic dichroism or eosinophilia. LGMS cells differ from smooth muscle cells and fibroblasts in that they have atypia, with less well-defined cytoplasmic borders and often thin filaments, which mainly run under the membrane and are parallel to the cell’s long axis; nuclei of LGMS cells tend to be longer as compared to smooth muscle cells and sharpened at both ends, often with pseudoneural-like curves (which reflect contractile properties of the cells), finely granular chromatin, and frequently prominent nucleoli. The tumor, in this case, had histologic and immunohistochemical characteristics of LGMS, primarily in the larynx, and belonged to a rare group of laryngeal LGMS. Desmin, S-100 protein, laminin, or epithelial markers such as pan-cytoadhesin or EMA are not stained in LGMS cells. 16
LGMS is more common in adult males and tends to recur locally, but rarely metastasizes distantly, and its pathological diagnosis must be combined with the immunohistochemical examination; LGMS is insensitive to chemoradiotherapy, and the most effective treatment for this tumor is wide surgical resection, where recurrence is related to whether the tumor is completely removed, so resection of the tumor should be performed in a large range during surgery while achieving complete removal. 17 Despite its slight invasiveness, LGMS is considered low-grade malignant in the clinic, and its prognosis is good after clinical surgical treatment. The disease course was short in this case, the local tumor invasion range was broad, and no local or distant metastasis was discovered during the operation. Upon pathological results and imaging examination, this tumor had a node metastasis (TNM) stage of T3N0M0, and its growth characteristics matched literature reports. Furthermore, the surgical approach was total laryngectomy, and the intraoperative frozen surgical margin was negative. Radiotherapy and chemotherapy were not required after the surgery.18-20 However, the patient’s follow-up observation should be closely monitored because the tumor has the propensity to recur locally.
Conclusion
This report describes a rare case of laryngeal LGMS. It emphasizes the importance of histopathology and choosing a rational surgical approach for the patient’s prognosis and survival. However, because the number of LGMS reported in the literature is small, more research into the clinical characteristics, malignancy, and treatment of this tumor is needed.
Footnotes
Author’s Contribution
“Yang G-L compiled the patient’s data, reviewed the literature, and wrote the manuscript; Li C-L was the patient’s surgeons and provided the patient’s information; Long Y-L helped perform the analysis with constructive discussions. Liu Z-H was responsible for the review and revision of the manuscript; and Rao C, Zhang Y-C, Liu Y, Yang H-H helped perform the data collection. All authors have given final approval of the submitted version of the manuscript.”
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
The study was reviewed and approved by the Ethics Committee of Affiliated Hospital of Zunyi Medical University (KLL-2022-730). All participants gave their informed consent to participate.
Informed Consent
A written informed consent was obtained from patients (participants) to publish this paper
Data Availability
The data presented in this study are available on request from the corresponding author.