
Abstract
Objective
Mucormycosis is an opportunistic fungal disease that affects immunocompromised patients. With the advent of SARS-CoV-2, this opportunistic disease has increased.
Methods
A case series of 47 patients with COVID-19 associated mucormycosis have been analyzed. Demographic information, signs, symptoms, laboratory investigations, imaging studies, and their association with ICU admission and 30-day mortality were assessed.
Results
Total number of 47 consecutive rhino-orbital cerebral mucormycosis (ROCM) cases were analyzed. Periorbital swelling was the most common sign among patients. Majority of cases had diabetes. All patients received liposomal Amphotericin B. Debridement was performed for all cases.
Conclusions
SARS-CoV-2 increases the susceptibility to mucormycosis infection in various ways. Uncontrolled level of HbA1c in all patients, even non-diabetic individuals, indicates hyperglycemia over the past three months. Diabetes, orbital exenteration, ptosis, periorbital swelling, DKA, LOC, brain involvement, and mechanical ventilation all correlated with a higher rate of ICU admission and 30-day mortality. In addition, a higher white blood cell count is related to the higher probability of ICU admission. While considering all of the inflammatory laboratory data and HbA1c could help predict 30-day mortality.
Keywords
Introduction
Mucormycosis is a fungal infectious disease caused by Mucorales order. 1 The most-reported pathogens responsible for mucormycosis are Rhizopus spp, Mucor spp, and Lichthemia spp, respectively. 2 This fungal pathogen infects paranasal sinuses, orbit, and even cranial components. 1 Mucormycosis usually affects immunodeficient, diabetic, and patients who suffer from malignancies or are receiving immunosuppressive drugs. 3
SARS-CoV-2 is a virus that first emerged from Wuhan, China, and then spread throughout the world, causing a pandemic. 4 Different studies have confirmed that the incidence of fungal superinfection in COVID-19 patients ranges from 14.8 up to 33% varying based on disease severity. 5 In Iran, only 98 cases of mucormycosis were detected in the whole literature until 2015. 6 Coronavirus, through various pathways, can predispose the infected patients to mucormycosis infection. SARS-CoV-2 directly causes immune system dysregulation and hyperglycemia. In addition, the use of immune-modulatory drug agents makes patients more susceptible to mucormycosis infection.7-10
Rhino-orbital cerebral mucormycosis (ROCM) is a type of mucormycosis infection in COVID-19 patients. ROCM is a fatal disease with an approximate mortality rate of 40%. 11 Mucormycosis infection is manifested by symptoms such as visual deterioration, nasal black discharge or bleeding, facial or periorbital swelling, facial pain, and neurologic symptoms.12-14
There are various modalities to diagnose mucormycosis. The most accurate are histologic specimen and microscopic evaluation. 15 In addition, imaging modalities are helpful and less invasive. Magnetic resonance imaging (MRI) with gadolinium contrast is the imaging of choice. 16
The management of this disease has 2 components: medical and surgical management. The medical treatment consists of administering Amphotericin B, Psoconazole or Isavuconazole, and glycemic control.2,13,17 Surgical debridement is utilized to control infection spread and manage the disease. 18
The aim of this study is to find the relation between symptoms, signs, risk factors, investigations, pathology, and mortality or intensive care unit (ICU) admission of COVID-19 associated mucormycosis (CAM) patients in a single tertiary-center Loghman Hakim Hospital, Tehran, Iran.
Method
Study Design
A case series study was conducted on COVID-19 patients with mucormycosis infection. The inclusion criteria were reverse transcriptase-polymerase chain reaction (RT-PCR)-proven cases of COVID-19 in Loghman Hakim Hospital in Tehran, Iran from 20th of December to 25th of August, plus infection with mucormycosis. The ethics committee of Shahid Beheshti University of Medical Sciences approved this survey. The study protocol was in accordance with the Declaration of Helsinki. All the included patients were informed about the purpose of the study, and written consent was obtained.
Case Definition, Data Collection Laboratory, and Histopathological Surveys
All patients with (RT-PCR) confirmed coronavirus infection, who were diagnosed with histopathological proven sinonasal mucormycosis were included. The interval between 2 infections was not more than 4 weeks. Nasopharyngeal and oropharyngeal swab specimens of patients were evaluated by RT-PCR. Biopsies from paranasal sinuses and nasal mucosa were obtained for histopathological examination.
The diagnosis is confirmed by revealing broad non-septate hyphae with rectangle branching and twisting morphology. The fungal hyphae are seen in the tissue with vascular and neural invasion, thrombotic infarction, and variable inflammatory cells in the background (Figure 1). Nasal biopsy shows broad non-septate hyphae with rectangle branching and twisting morphology and necrosis (PAS*100).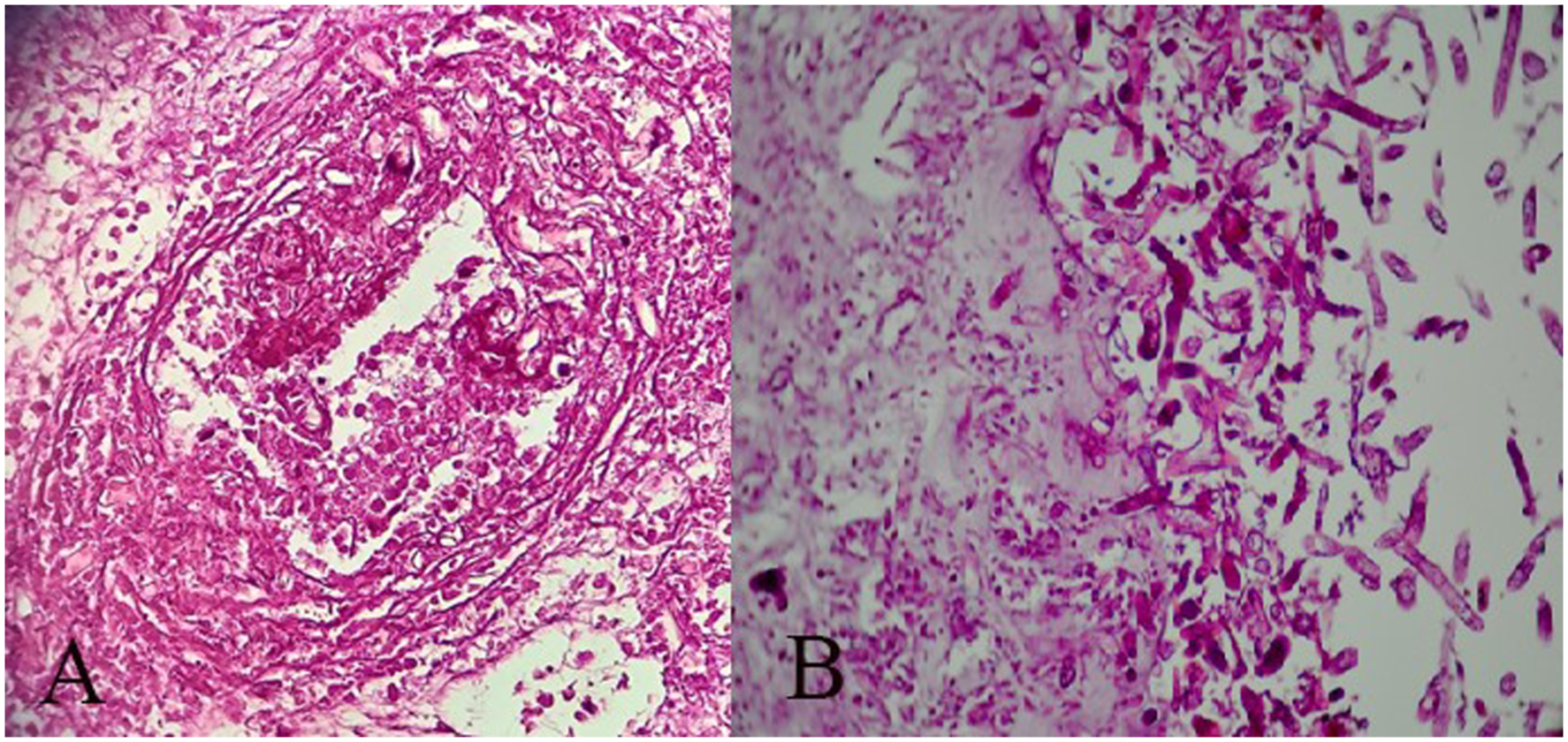
Demographic, clinical manifestations, and infection sites of each included patient were recorded. Clinical symptoms were divided into 2 groups: primary and secondary symptoms. Secondary manifestations were defined as symptoms that were developed during the disease course. ICU admission, means of oxygen administration, and medical and surgical treatments were all studied. ICU admission was considered as a parameter for disease severity. Moreover, patients were followed up for 30 days to analyze the mortality rate.
Computed tomography (CT) and MRI with gadolinium contrast of orbits, paranasal sinuses, and brain were also performed and the data was analyzed. In addition, pathological and laboratory data including cell blood count (CBC), erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), ferritin, and HbA1c were also analyzed.
The statistical analysis was conducted using SPSS version 22. Chi-square test and binary logistic regression tests were conducted to assess the association of nominal and quantitative variables and ICU admission or 30-day mortality. P-value less than .05 was considered to be statistically significant.
Results
Forty-seven patients were included in the study, 22 (47%) and 25 (53%) were female and male, respectively. This was significantly higher in comparison to the 98 cases reported from 199 to 2015. 6 The average age was 57.0 ± 10 (SD) years. The mean interval between early COVID-19 infection and sinonasal mucormycosis was 12.7 ± 4.6 days. Thirty-four (74%) patients suffered from diabetes mellitus as their underlying medical disease. Based on medical documents, the rest 26% did not suffered from diabetes. Interestingly 11 out of 47 patients (23%) had no significant past medical history. Other frequent underlying diseases were hypertension, ischemic heart disease, end-stage renal disease (17%, 4%, and 4%, respectively). Approximately 30% of patients were diagnosed with more than one underlying disease.
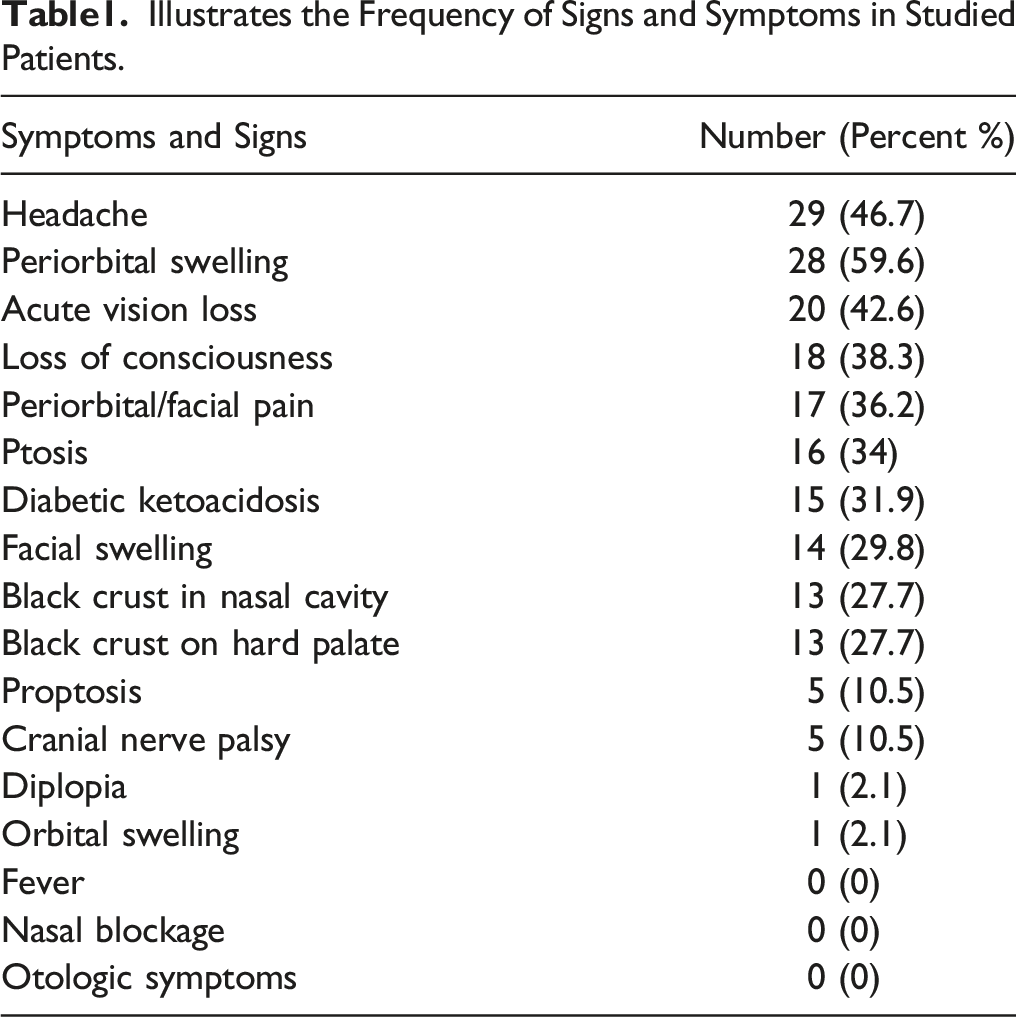
The most frequent symptom noted among cases was headache (29 patients or 62%), 28 patients (59%) had periorbital swelling (Figure 2). Other symptoms frequencies and percentages are reported in Table 1 in detail. Fever was not reported in any of the cases. Patients with periorbital edema and proptosis. Illustrates the Frequency of Signs and Symptoms in Studied Patients.
Indicates the Frequency of Paranasal Sinus Involvement.
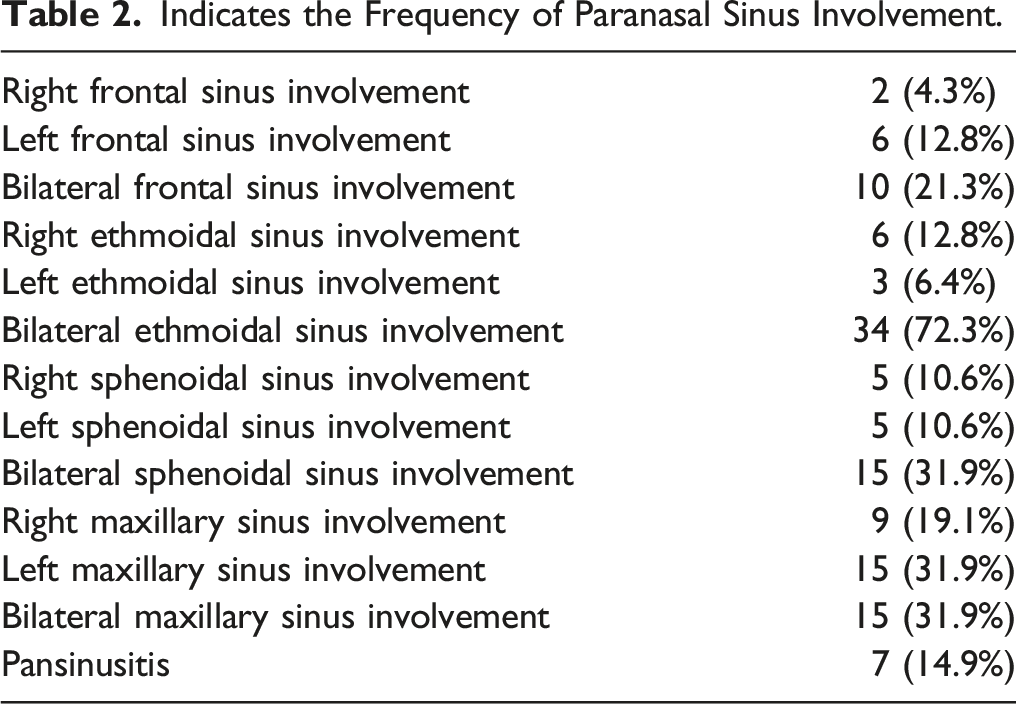
As illustrated in Table 2, most cases had bilateral ethmoidal involvement. 91% of cases experienced ethmoidal involvement, which was mostly bilateral. In addition, 14.9% of cases had pansinusitis.
Brain complications including infarction and ischemic events (17%), brain involvement (29.8%), and brain abscess (2.1%) were also reported.
Various laboratory investigations were performed for all cases, including cell blood count (CBC) ferritin, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and Hemoglobin A1c (HbA1c).
Illustrates the Laboratory Data of Included Individuals.

All cases were treated with systemic corticosteroids, liposomal Amphotericin B, and antibiotics. The average dexamethasone dose administered during hospitalization was 121.7 ± 79.7 milligrams. Minimum and maximum doses administered were 30.0 and 576.0 milligrams, respectively.
Sinus debridement (endoscopic sinus surgery was used to removed crust and debris) was performed for all patients since none responded solely to antifungal treatment. In addition, orbital exenteration was performed on 14 cases (29.8%).
All patients received oxygen via mask or mechanical ventilation. In addition, 10 patients (21.3%) were mechanically ventilated. Twenty-two (47%) cases were admitted to the ICU.
Illustrates the Evaluation of ICU Admission and Possible Related Comorbidities.
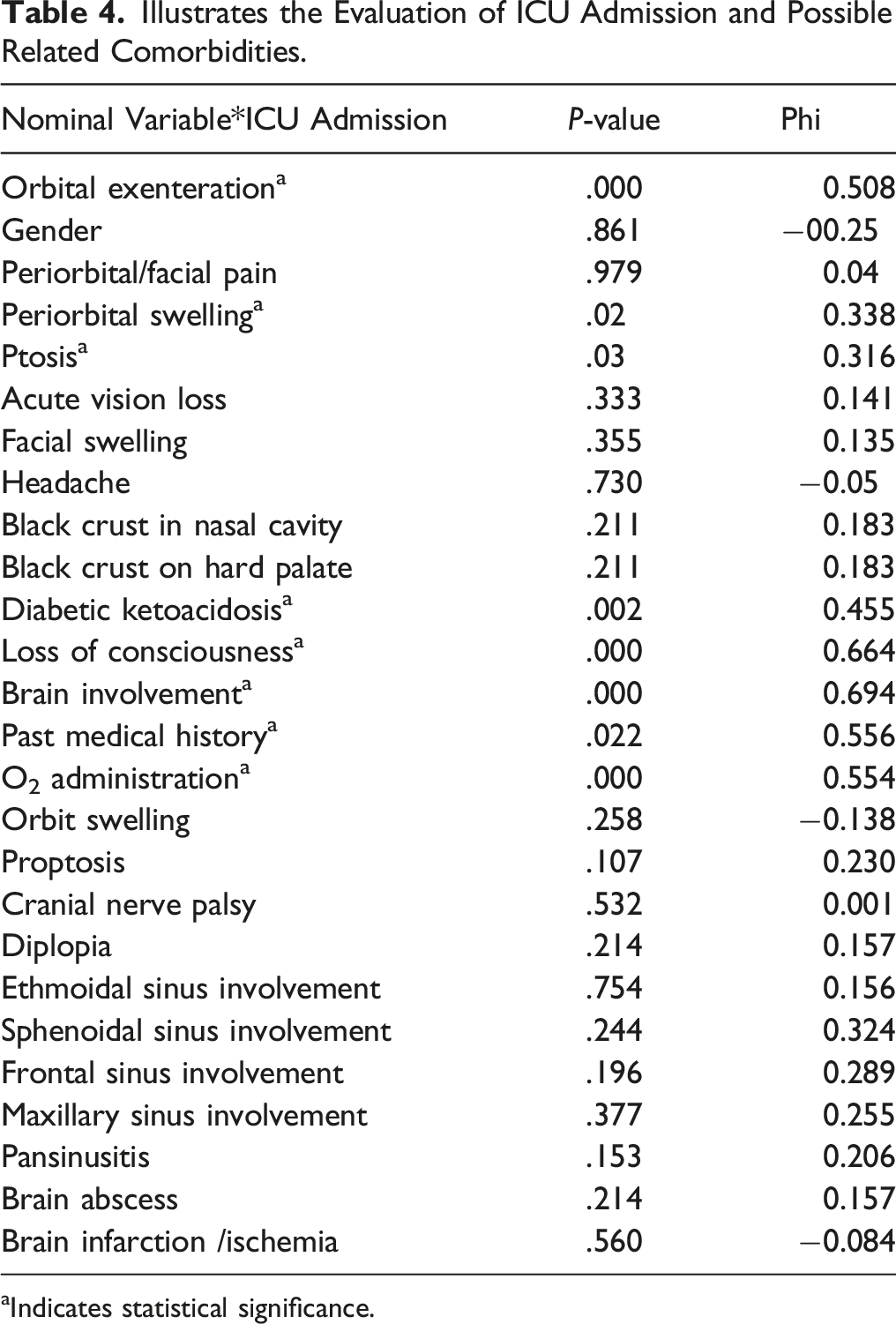
aIndicates statistical significance.
As is illustrated in Table 4, orbital exenteration, ptosis, periorbital swelling, diabetic ketoacidosis, loss of consciousness, brain involvement, past medical history (diabetes), and O2 administration (mechanical ventilation) were all statistically related to ICU admission. Brain involvement had the highest Phi score (0.694), which indicates the highest rate of association with ICU admission.
Shows Evaluation of 30-day Mortality and Possible Related Comorbidities.
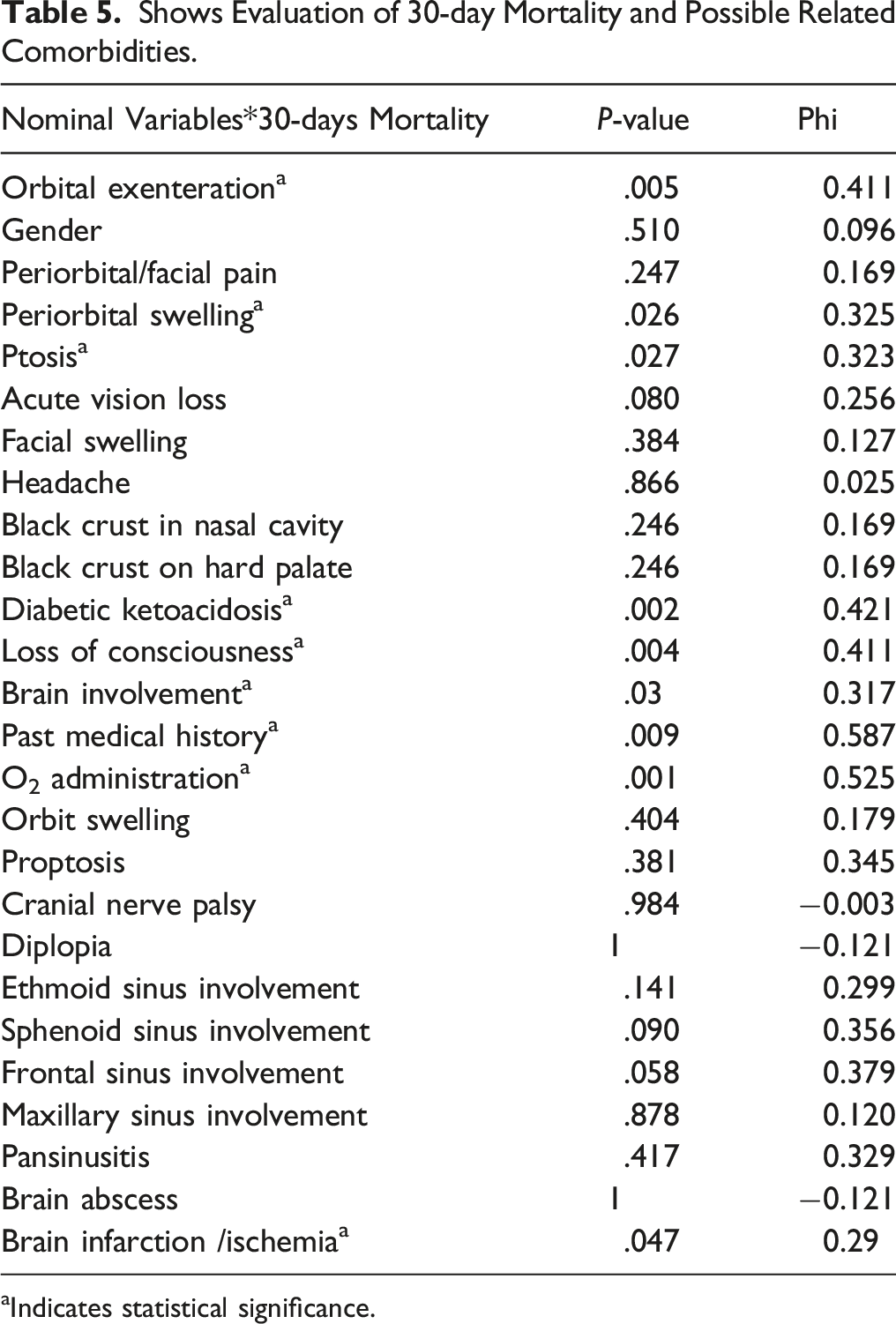
aIndicates statistical significance.
Logistic regression test was conducted to determine if quantitative variables (including white blood cell count, HbA1c, ferritin, ESR, CRP, and the interval between first COVID-19 infection manifestation and mucormycosis) could predict the likelihood of ICU admission and 30-day mortality separately.
Except for white blood cell count (P = .025), none of the quantitative variables had a statistically significant relation with ICU admission.
The result of logistic regression conducted to predict 30-day mortality was statistically significant (P-value = .033, Chi-square (7) = 15.230). Although the combination of all quantitative variables could help predict 30-day mortality, none solely was a significant indicator of 30-day mortality. This model explained 27.7% (Cox and Snell R Square) and 37.4% (NagelkerkeR Square) of variance mortality and correctly classified 68.1% of the cases. Sensitivity and specificity were 57.9 and 75%, respectively.
Discussion
SARS CoV-2 virus has caused a worldwide disease that, besides diffuse alveolar damage, causes immunological system dysregulation and decreases the CD4 and CD8 T cells, eventually leading to immunosuppression. 20 Before the COVID-19, mucor was a rare event. 21 Pathogens exist in the environment and commensal on the body surface. By inhalation, the spores enter the nasal cavity and inoculate paranasal sinuses and nasopharynx. 1 While Mucorales order does not threaten immunocompetent individuals' health, 22 for immunocompromised patients, this infection may lead to pathogen germination in paranasal sinuses, nasopharynx, and eventually spreading to the central nervous system(1). SARS-CoV-2 virus can directly invade pancreatic islet cells or vessels that nourish them, thus causing new-onset diabetes.23,24 Inflammatory reaction also causes insulin resistance which eventually leads to hyperglycemia.8,25 COVID-19 related hyperglycemia, corticosteroid use in COVID-19 management, increase in ferritin level, hypoxia, and COVID-19 induced immune dysregulation predispose patients to mucormycosis co-infection.5,26 The most common form of mucormycosis in patients infected by SARS CoV-2 is ROCM which accounts for 90% of cases. 27
Following previous studies, the majority of the cases in our survey were middle-aged with the mean age of 57 ± 10 years. Previous studies have demonstrated that most patients suffering from ROCM after COVID-19 infection were male.28-30 As a result, hypothesizing that estrogen has a protective role. Despite previous studies, no statistically significant difference was observed between the 2 genders in ours. The interval between COVID-19 infection and ROCM ranged from 10 to 14 ± 10 days. 29 We have reported a 12.7 ± 4.6 days delay between these 2 infections. Delayed COVID-associated ROCM was also reported, emphasizing the importance of following the mucormycosis susceptible cases for over three-month period. 30 Iron overload, malignancies of any type, consuming corticosteroids, organ transplantation, immunosuppressive drugs, immunodeficiencies, and diabetes were all considered classical risk factors of mucormycosis.14,31 Diabetes was reported as the major risk factor in COVID-19 associated ROCM.32-35 Other risk factors included prolonged corticosteroid use, hyperglycemia, hypertension, and chronic renal failure.26,33,36-39 The reason that diabetes makes patients vulnerable to infection could be due to abundant free iron in blood, poor immune response, high level of blood glucose, and acidic PH of the blood. 40 In our study, diabetes was an essential risk factor either for ICU admission or 30-day mortality. No relation between the dose of corticosteroid and ICU admission or 30-day mortality was found.
Patel et al. reported that disseminated and ROCM, shorter duration of symptoms, shorter duration of antifungal therapy, using Amphotericin B deoxycholate instead of liposomal Amphotericin B are related to the higher rate of mortality rate in CAM. 32 In our study, diabetes, orbital exenteration, ptosis, periorbital swelling, DKA, LOC, brain involvement, and mechanical ventilation were indicators of 30-day mortality and ICU admission. Although 25% of patients had no past medical history, all had HbA1c higher than 7 (with the mean of 11.4 ± 1.44), indicating high blood sugar during the past three months. Naruka et al. performed a single center study in India, including 79 patients with COVID-19 and associated ROCM. In their survey, only 67 patients reported suffering from diabetes, and 12 newly-onset diabetes were recognized. 41 This phenomenon could be due to injudicious use of a glucocorticoid, hyper-inflammation status, or COVID-19 new-onset hyperglycemia in patients' bodies.
Although the RECOVERY trial has shown the positive impact of corticosteroids in the management of patients suffering from moderate to severe COVID-19, prolonged and high doses of glucocorticoids predispose patients to mucormycosis infection.42,43 The mean Dexamethasone dose prescribed totally for patients was 121 ± 79 mg. Despite previous studies, there was no meaningful relationship between the dose of dexamethasone and the rate of mortality.
Nasal stuffiness, fuel smell, epistaxis, nasal discharge, nasal mucosal erythema/inflammation/blue or purple discoloration/ eschar or white ulcers, eyelid/periocular/facial edema or discoloration, regional pain, facial pain, worsening headache, sudden loss of vision, facial paresthesia, sudden ptosis, proptosis, ocular motility restriction, diplopia, facial palsy, fever, altered sensorium, focal seizure, ophthalmoplegia, sinuses involvement, cranial nerve palsy, palatine involvements, and even retinal artery occlusion were observed in CAM.2,14,44-48
In an observational study of 2826 patients in India, orbital/facial pain (23%) and periocular/facial edema (33%) were the most frequent primary symptom and sign, respectively. 30
In this survey, periorbital edema and headache were most common among affected patients accounting for 59.6% and 46.7% of studied patients, respectively. None of the patients surprisingly had a fever or nasal blockage.
No laboratory examination could solely predict the probability of 30-day mortality in CAM patients, but rather the combination of all mentioned laboratory data to project patients' prognosis.
On the other hand, the only useful laboratory data to predict ICU admission is WBC count.
Ethmoid and maxillary sinuses are the most involved paranasal sinus in CAM.21,33 By previous studies, bilateral ethmoid, maxillary, and sphenoid were mostly affected by mucormycosis among our patients (72.1%, 31.9%, and 31.9%, respectively). Ethmoid sinuses were affected in 91% of cases, making the ethmoid sinuses the most infected among all.
Mucormycosis can spread to the central nervous system causing infarction, brain and cavernous sinus involvement. 21 49% of the studied cases suffered from central nervous system involvement.
Early diagnosis and multi-disciplinary management of COVID-19 associated ROCM improve the prognosis. Tight control of predisposing factors especially hyperglycemia, proper antifungal medication (liposomal Amphotericin B), and appropriate debridement are essential in CAM management. 30
ROCM is a progressive and opportunistic infection with variable mortality rates from 30 to 90% in cases with brain involvement.30,49 In COVID-associated cases, the overall mortality rate was estimated at 30.1%. 26 In this study, 40.4% of cases passed away during 30 days of follow-up.
Limitation
This study was conducted as a single-center survey. A multi-center study with more patients is required to have more precise results. A longer period of follow-up helps to determine the exact rate of mortality and other possible delayed complications.
Conclusion
COVID-19 associated ROCM is a lethal opportunistic infection with a bad prognosis. Therefore, early diagnosing is lifesaving and requires a high level of suspicion. Uncontrolled level of HbA1c in all patients, even non-diabetic individuals, indicates hyperglycemia over the past three months which could be the result of SARS-CoV-2 or injudicious use of steroids. Diabetes, orbital exenteration, ptosis, periorbital swelling, DKA, LOC, brain involvement, and mechanical ventilation all correlated with a higher rate of ICU admission and 30-day mortality. In addition, a higher WBC level is related to the higher probability of ICU admission. While considering all of the inflammatory laboratory data and HbA1c together could help predict 30-day mortality. To contain and control the infection, rapid multi-disciplinary management, including debridement and an adequate amount of proper antifungal medication is required.
Footnotes
Author Contribution
NAD and MK conceptualized the study; NB, MK, and KE acquisition of data and drafting the manuscript; and KE and MF revising for critical intellectual concept and approved the version to be submitted.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
This study was ethically approved by ethical committee of Shahid Beheshti University of Medical Sciences (date of approval: January 21, 2021). Written informed consents were obtained from all included patients.
Data Availability
All analyzed data during this study are included in this article and its supplementary material files. Further enquiries can be directed to the corresponding author.