
Abstract
Nasopharyngeal stenosis is a rare condition and occurs usually secondary to nasopharyngeal or oropharyngeal surgery and radiotherapy. It may cause obstructive symptoms in patients and is diagnosed usually with nasopharyngoscopy. Treatment is difficult and requires different surgical techniques including balloon dilatation. Even after a successful surgery, recurrence is very common.
Introduction
Nasopharyngeal stenosis (NPS) is rare. In case of an NPS, there is a scar tissue that narrows and obstructs the nasopharyngeal passage. In the past, it usually occurred as a complication of some infections like tuberculosis rhinoscleroma, syphilis, or diphtheria. 1 Other than infection cicatricial pemphigoid, an autoimmune disease can also cause NPS. Today, usually adenoidectomy, uvulopalatopharyngoplasty, pharyngeal reconstruction for velopharyngeal insufficiency, or other procedures in the pharynx and radiation therapy are the major causes. 2 The obstruction is observed at various levels in the nasopharynx, from posterior choanae to eustachian tubes, from the roof to floor of the nasopharynx. Most common stenosis is between these structures: posterior edge of the soft palate, tonsillar pillars, and posterior pharyngeal wall. 1 The form of NPS can vary from a thin membrane to a thick, obliterative mass of fibrous tissue. 3
Transnasal fiberoptic nasopharyngoscopy is usually sufficient for diagnosis and it is also very useful in therapeutic planning. 1,4 Computed tomography and MRI can also give information about the extent, location, and thickness of the stenotic area, especially if thin slices are taken, otherwise a membranous stenosis may not appear on the images. 5
Definitive treatment is often very difficult, different flap techniques or balloon dilatations are the surgical methods, but every new surgery has the potential of more scarring and restenosis. 2,6 Because every oropharyngeal and nasopharyngeal surgery carries the risk of stenosis, during surgery attention should be paid not to leave exposed tissue surfaces in contact with each other. In addition, excessive use of cautery and other devices like laser should be avoided. 7
In the present article, we are reporting a 43-year-old female NPS patient that presented with several obstructive complaints and had no history of surgery or trauma.
Case Presentation
A 43-year-oldfemale patient presented to the Otorhinolaryngology clinic with complaints of bilateral nasal obstruction, facial pressure, oral dryness, sleeping with an open mouth, snoring, and a 5-year history of sleep apnea. A physical examination and nasal endoscopy revealed extensive synechiae between the nasal septum and inferior and middle turbinates, and a near complete nasopharyngeal stenosis. The patient did not have a history of pharyngeal surgery or trauma. Magnetic resonance imaging (MRI) of the paranasal sinuses and nasopharynx revealed a membranous thin soft tissue along nasal floor extending posterosuperiorly to the right and left nasal passages and obstructing the nasopharynx (Figure 1). Sagittal T2-W, post-contrast sagittal and axial T1-W MR images show a membranous thin soft tissue (arrows) along nasal floor extending posterosuperiorly to the right and left nasal passages and obstructing the nasopharynx. All of MR images reveal membranous nasopharyngeal stenosis.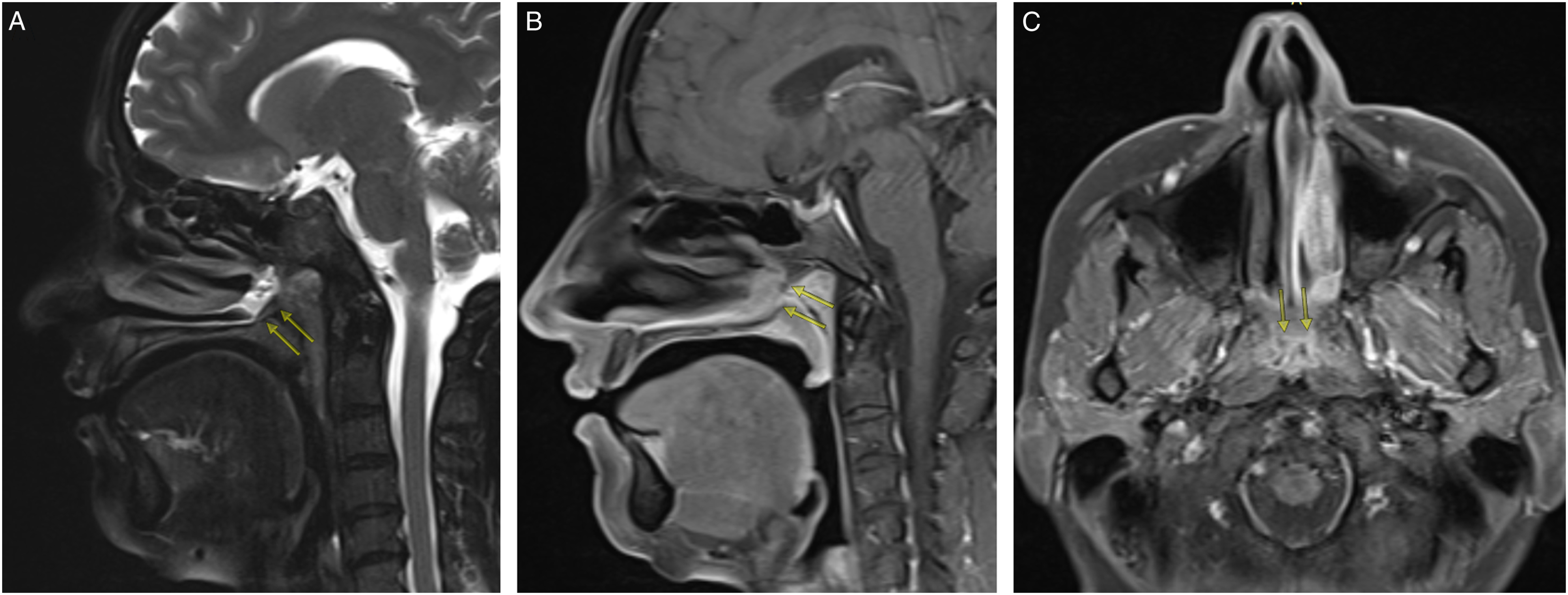
Conclusion
Nasopharyngeal stenosis is a rare condition but may cause severe obstructive symptoms. Because it usually is secondary to an oropharyngeal and nasopharyngeal surgery, a careful approach during these surgeries is very important. In the treatment, multiple surgical interventions maybe necessary because recurrence is common.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.