
Abstract
Objectives
Rhinitis, one of the most common inflammatory conditions of the nasal mucosa, is known to affect a large proportion of people worldwide. It is generally classified into allergic and non-allergic types and both are associated with several unpleasant symptoms. Several medications prescribed for different medical conditions can cause unpleasant rhinitis as an adverse effect, which is known as drug-induced non-allergic rhinitis. The aims of this article were to review the literature to identify drugs that could induce rhinitis, prevalence of drug-induced rhinitis, and the associated pathogenic mechanisms if known.
Methods
Literature search screening for eligible papers published up to December 31st, 2021, in Medline (via PubMed) and Embase was conducted. The search included the following combination of keywords and terms: rhinitis, sneezing, congestion, allergic, non-allergic, rhinorrhea, vasomotor, medication, drug-induced.
Results
The review findings suggest that 12 subtypes of drugs potentially could induce rhinitis. Based on their mechanisms of action, the pathogenic causes for the induction of rhinitis have been recognized for some drugs, while others remain unknown.
Conclusion
Awareness of the list of drugs that reportedly induce non-allergic nasal symptoms, along with taking the patient’s medication history, is important in the diagnosis of rhinitis.
Introduction
Rhinitis is a common inflammatory condition of the nasal mucosa that typically leads to several unpleasant symptoms, such as itching, runny nose, nasal congestion, sneezing, and irritation or discomfort in or around the nose. 1 Rhinitis affects the quality of life of a large proportion of the population worldwide and can lead to decrease in performance and productivity at work and school and adversely affect social interactions secondary to its unpleasant symptoms. These unpleasant symptoms may vary between mild conditions such as irritability, and embarrassment to more debilitating conditions such as tiredness, snoring, and obstructive sleep apnea syndrome. 2 Therefore, rhinitis importance as a medical condition has increased and gained more attention of healthcare workers.
In 2020, a study conducted in Al-Baha, Saudi Arabia, showed a prevalence of allergic rhinitis in the Saudi population of 32% in males and 38.6% in females, and a greater association of more symptoms in females than in males. 3 In the United States, the prevalence of allergic rhinitis ranges from 9% to 42%, with 58 million people overall and 19 million who have non-allergic rhinitis (NAR). 4 Similar evaluations in Europe indicate that 50 million Europeans have non-allergic rhinitis. The absolute predominance of NAR is more than 200 million persons worldwide. 5
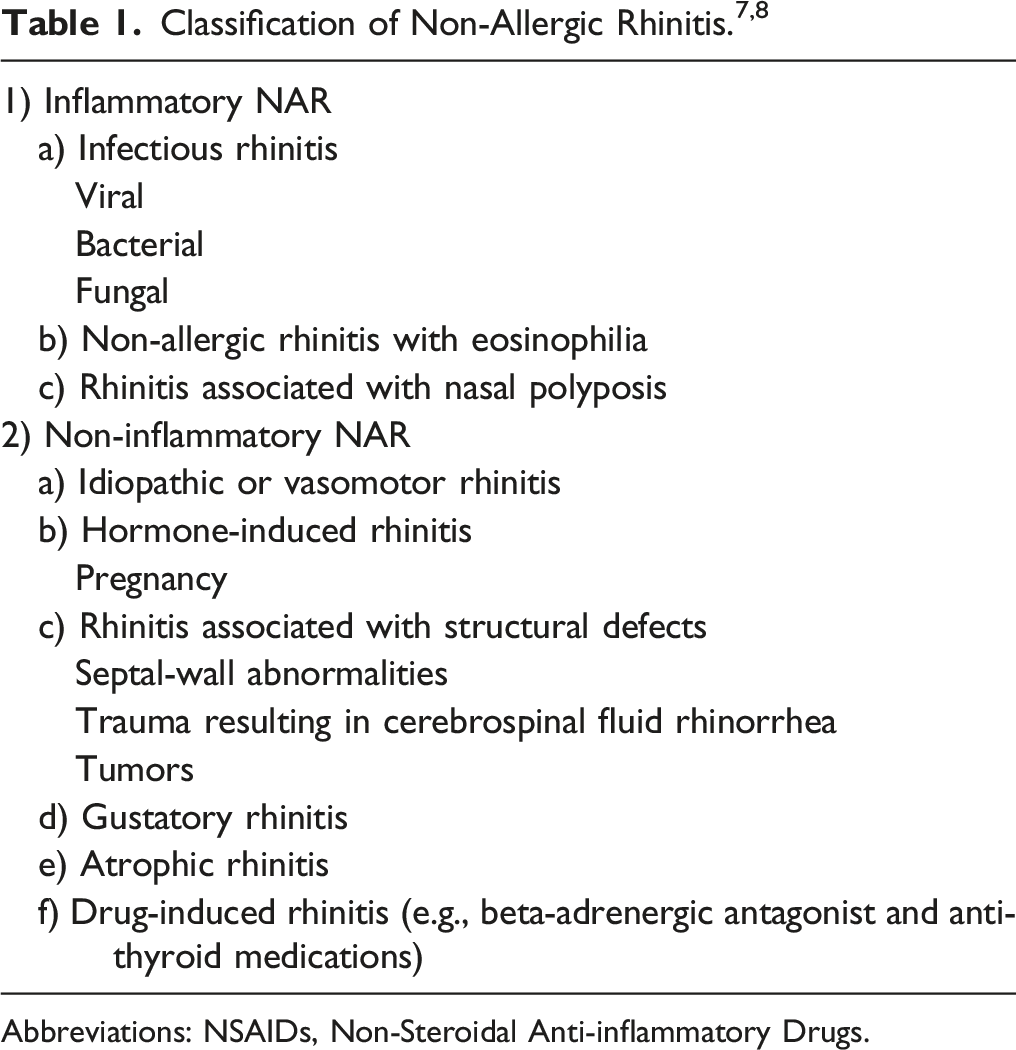
Abbreviations: NSAIDs, Non-Steroidal Anti-inflammatory Drugs.
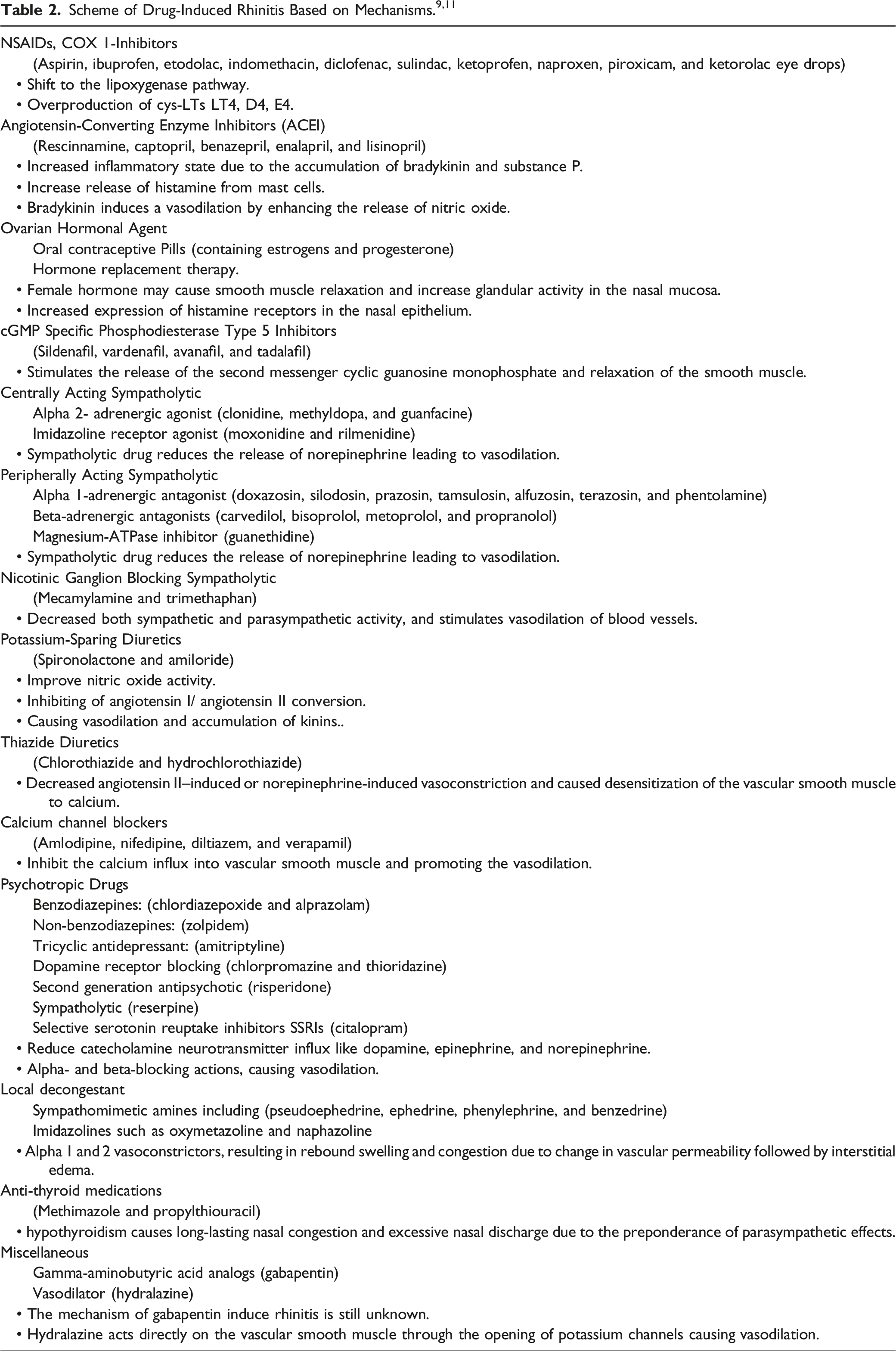
Drug-induced rhinitis is a type of non-allergic rhinitis that is caused by a range of reported drug classes (e.g., NSAIDS, alpha- and beta-adrenergic blockers, local decongestant) resulting in rhinitis related symptoms such as nasal congestion, itching or runny nose. M. Varghese et al. had classified drug-induced rhinitis into 3 main types: local inflammatory type, neurogenic type and idiopathic (unknown) type. However, the documented drugs to induce rhinitis were further categorized into subgroups based on their mechanisms of action. 4,8,9 Despite the fact that a wide variety of medications may cause nasal symptoms, there is a noticeable lack of information on its prevalence as well as a deficiency in researches describing the pathogenesis of these drugs to induce rhinitis, and most of the available data are based on separate case reports. Therefore, the goal of this study is to evaluate and summarize all drugs that may cause rhinitis and, if applicable, to identify any associated pathogenic pathways.
Methodology
A narrative literature search, screening for eligible papers published up to December 31st, 2021 via the databases Medline (via PubMed) and Embase was carried. Moreover, google scholar was searched to identify any non-indexed relevant publication. The search included the following combination of keywords: rhinitis, drug-induced, sneezing, medication, congestion, allergic, non-allergic, rhinorrhea, and vasomotor to identify studies that reported drugs associated with rhinitis. The narrative review methodology as described by Green et al. was used to conduct this non-systematic narrative review of the literature regarding drug-induced rhinitis. 10 Those articles were included in the study that had done research on the pathogenic mechanism associated with drugs that reported to be potentially associated with rhinitis, which were of cross-sectional, cohort, case–control, interventional, and review article types. Moreover, a narrative data synthesis regarding these pathogenic mechanisms was conducted. Exclusion criteria for articles were non-English language, improper research design or statistical methods, and studies in non-human populations.
Result
The prevalence of non-allergic rhinitis was unclear until very recently with a study that was done in the Netherlands and published in 2022 showed that the approximated prevalence of drug-induced rhinitis was 1% while hormonal induced rhinitis was around 4%. 12 However, there are no reported studies done in Saudi Arabia to quantify drug-induced rhinitis prevalence.
Non-Steroidal Anti-Inflammatory Drugs
Acetylsalicylic acid (ASA or Aspirin), ibuprofen, etodolac, indomethacin, diclofenac, sulindac, ketoprofen, naproxen, piroxicam, and ketorolac eye drops are members of the NSAIDs that have been commonly reported to cause nasal inflammatory responses. 11,13
Pathogenic Mechanism
NSAIDs introduce rhinitis by an adverse effect of the inhibition of cyclooxygenase 1 (COX 1). This inhibition elevates the rate of metabolism of arachidonic acid through the lipoxygenase pathway, while decreasing the expression level of prostaglandin 2 (PGE2), thereby actually inhibiting the production of cysteinyl leukotrienes (Cys-LTs) which are inflammatory mediators. Therefore, the reduction in the PGE2 level is associated with overproduction of the Cys-LTs LT4, D4, E4, and LTC4 as products of the lipoxygenase pathway. LTC4 is then stimulated after its interlinkage with Cys-LT receptors. LTC4 synthase is the enzyme responsible for the stimulation of Cys-LT, which is overexpressed in aspirin-induced rhinitis. 4,9,11
Angiotensin-Converting Enzyme Inhibitors
Angiotensin-Converting Enzyme Inhibitors (ACEIs) are one of the most commonly used drugs for the management of diseases including hypertension and heart failure and for improving kidney function in diabetic patients. Pinargote et al. mentioned that most physicians know about ACEI-initiated dry cough but are less aware of ACEI-initiated upper respiratory implications, such as nasal blockage, rhinitis, or postnasal drainage. 12 Among ACEIs, rescinnamine, captopril, benazepril, enalapril, and lisinopril are the most frequently reported ACEIs to cause nasal congestion or postnasal drainage. 5,9,11,14
Pathogenic Mechanism
The pathogenic mechanism is suggested to reflect that of ACEIs-induced dry cough, which is associated with an increased inflammatory state due to the accumulation of bradykinin and substance P. bradykinin is a vasodilator and inflammatory peptide that is broken down by Angiotensin-Converting Enzyme (ACE). The inhibition of the ACE activity causes an accumulation of bradykinin in the lungs and also the release of histamine from mast cells. Bradykinin and histamine, acting as inflammatory mediators, increase the vascular permeability leading to bronchoconstriction and nasal discharge. Conversely, bradykinin may also induce a vasodilation effect by enhancing the release of endothelial nitric oxide causing rhinitis-related symptoms
15
-17
(Figure 1). Angiotensin-converting enzyme inhibitors mechanism and side effects.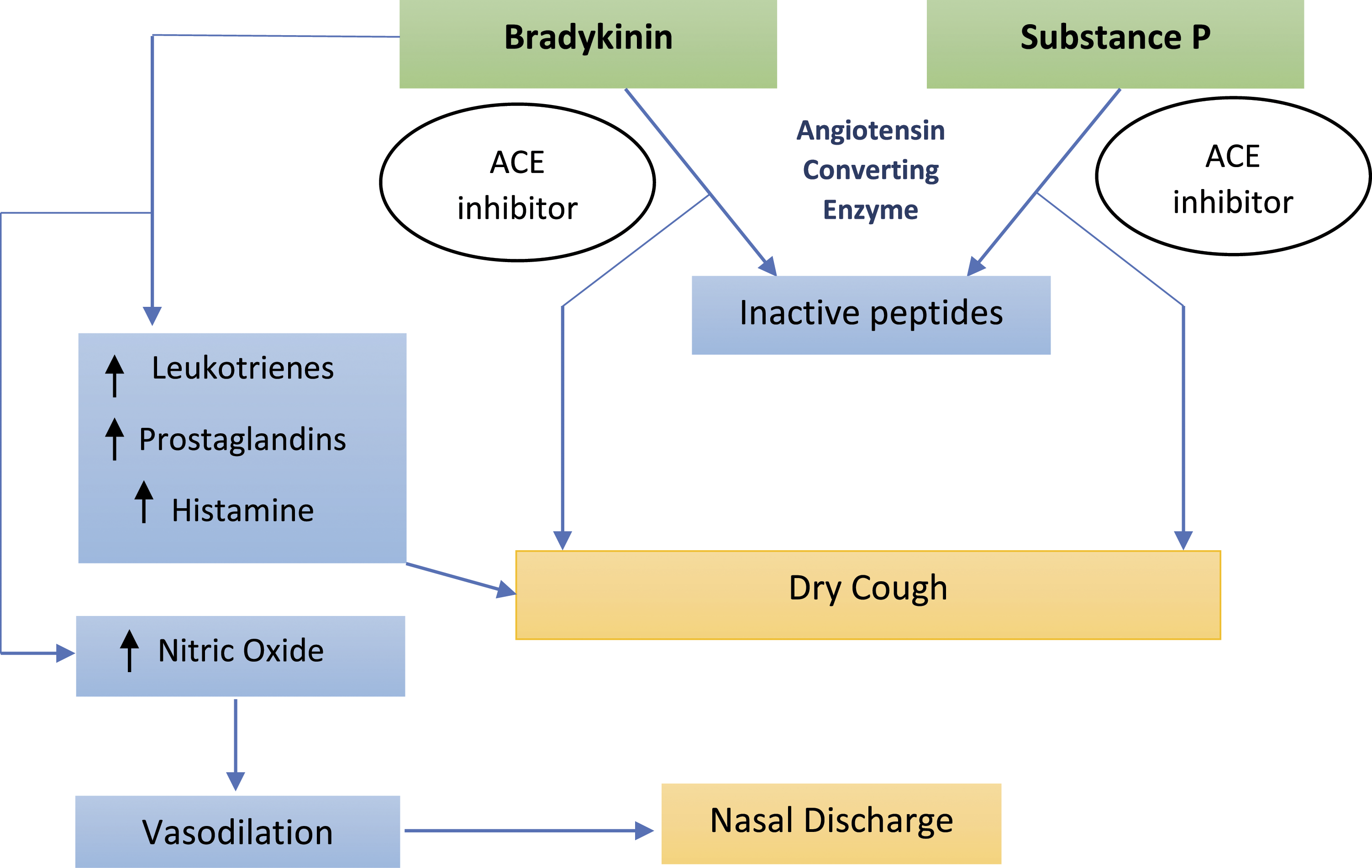
Ovarian Hormonal Agent
The appearance of nasal symptoms following the use of exogenous estrogens and oral contraceptives has been reported in some articles. 4,11 The Korean national health and nutrition examination survey showed that menopausal hormone therapy can also cause non-allergic rhinitis and posterior nasal drip. 18,19
Pathogenic Mechanism
Initially it is important to know the fact that estrogen receptors are spread over the nasal mucous membrane, thereby explaining the effect of ovarian hormones on the nose. 20 Philpott et al. found that nasal congestion is commonly associated with an elevation of the estrogen levels in the serum plasma. This elevation of female hormone levels may cause smooth muscle relaxation and increase glandular activity in the nasal mucosa where estrogen receptors are present. 21 However, the pathogenic cause is still debatable requiring more research. One other study suggested a different mechanism of sex hormone action involving an increased expression of histamine receptors in the nasal epithelium; “Estrogens and progesterone change neurotransmitter concentrations such as substance P to cause the symptoms of nasal stuffiness experienced.” 22 Toppozada et al. has also mentioned that the chronic use of oral contraceptives can create histological changes in the nasal mucosa secondary to epithelial edema, glandular hyperplasia, and increased secretory activity of the mucosal glands associated with hormones affect. 18 This adverse effect of hormones on nasal mucosa and induction of rhinitis-like symptoms deserve further research.
Phosphodiesterase Type 5 Inhibitors
Phosphodiesterase Type 5 Inhibitors (PDE5 inhibitors), include sildenafil, tadalafil, vardenafil and avanafil, are a group of dugs effective in the management of erectile dysfunction in men. These drugs are commonly reported to cause symptoms including runny nose, nasal congestion, sinus pain, sore throat, and other common rhinitis-like symptoms as side effects of using these medications. 4,5,9,11,23
Pathogenic Mechanism
PDE5 inhibitors work by improving the activity of the vasodilator nitric oxide, which stimulates the release of the second messenger cyclic guanosine monophosphate and relaxation of the smooth muscle in the corpus vessels, resulting in an increase in its blood flow. Nitric oxide (NO) transmitter is also present in the smooth muscle of blood vessels of the nasal mucosa and other erectile tissues present throughout the body. Guanylate cyclase is activated by NO to convert Guanosine Triphosphate (GTP) into Cyclic Guanosine Monophosphate (cGMP), which sets off a series of actions that are dependent on cGMP. The adverse effect of PDE5 inhibitors caused rhinitis is explained by the potent and selective inhibition of the cGMP PDE5 enzyme that destroys cGMP (Figure 2). The prevention of degradation of cGMP by PDE5 resulting in accumulation and increased level of cGMP which activate protein kinase resulting in smooth muscle relaxation, vasodilation, congestion, and rhinitis.
9,11,24
PDE5 inhibitor mechanism of action.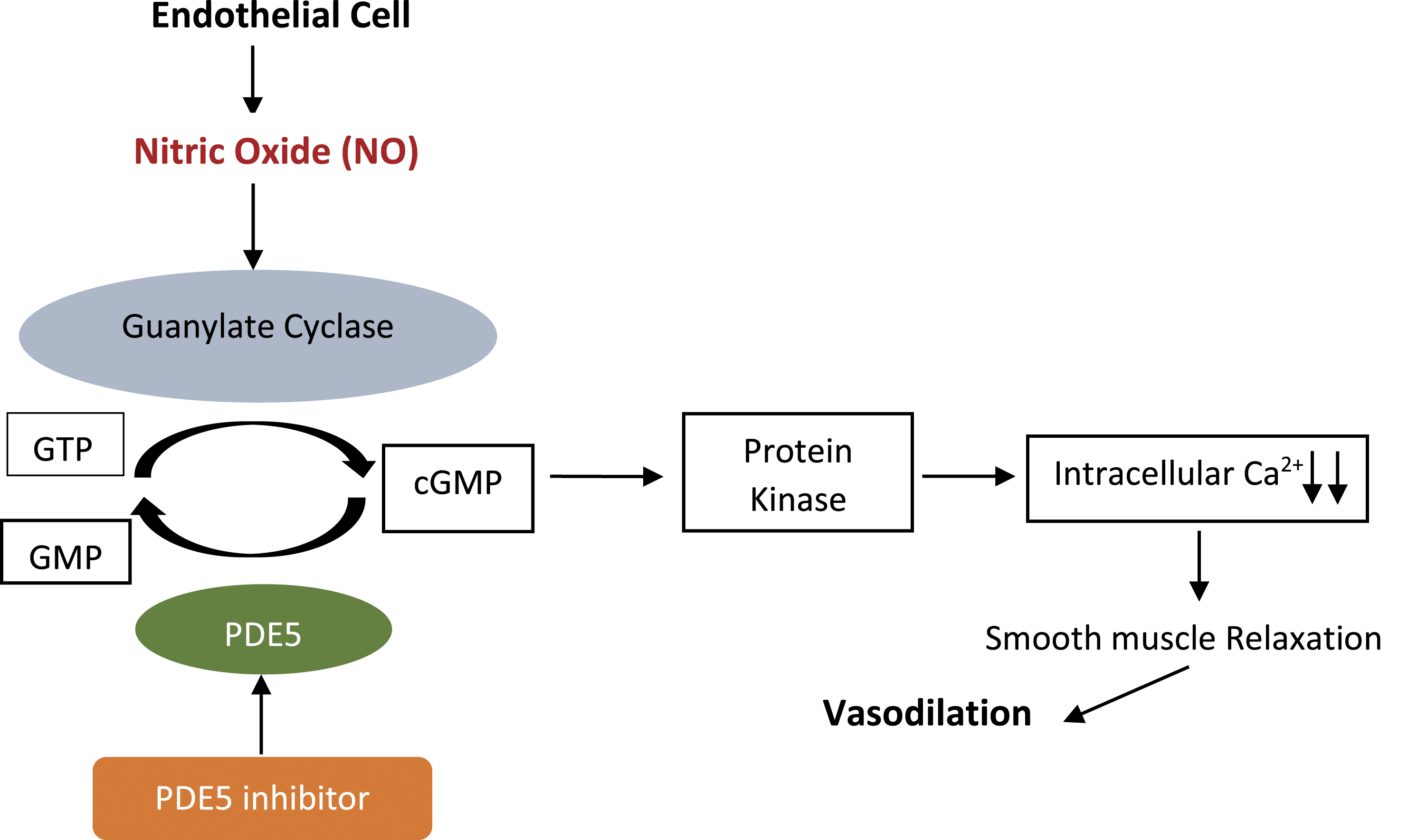
Centrally and Peripherally Acting Sympatholytic
Alpha 2-agonists (e.g., clonidine, methyldopa, and guanfacine) and imidazoline receptor agonists (e.g., moxonidine and rilmenidine) are centrally acting sympatholytic drugs that decrease endogenous norepinephrine by a negative feedback mechanism. Alpha 1-adrenergic blockers (e.g., doxazosin, silodosin, prazosin, tamsulosin, alfuzosin, terazosin, and phentolamine), some beta-adrenergic blockers (e.g., carvedilol, bisoprolol, metoprolol, and propranolol), and the magnesium-ATPase inhibitor guanethidine are considered peripherally acting sympatholytic. 5,8,9,11
Pathogenic Mechanism
Nasal congestion and rhinorrhea have been reported as a side effect of these medications by decreasing the sympathetic outflow in the nasal passages. Sympathetic and parasympathetic nerve fibers are abundantly found in the mucosa of the nose. Sympatholytic drug use affects the nasal blood vessels by reducing the release of norepinephrine from the sympathetic nerve terminals which acts as vasoconstrictor agent leading to vasodilation and increasing vascular permeability in the nasal blood vessels. 9,11,25
Ganglion Blocking Sympatholytic
Mecamylamine and trimethaphan are ganglionic blocking agents used to treat hypertension. Adverse effects of these medications are dose related and are decreased when dosage is decreased or drug is discontinued.
Pathogenic Mechanism
These drugs exhibit nicotinic cholinergic receptor antagonism. Upon binding of these drugs to the nicotinic receptor which is a cys-loop ligand-gated ion channels, they prevent its permeability to ions like Na+, K+, and Ca2+ and block the transmission of signals at the postganglionic neurons results in decreased both sympathetic and parasympathetic activity, and stimulates vasodilation of blood vessels including the capillaries of the nose, leading to nasal stuffiness. 9,11,26
Diuretics
Potassium-sparing diuretics are a class of widely used diuretics for the management of hypertension and heart failure. Nasal symptoms, including rhinorrhea, have been reported as side effects of spironolactone and amiloride. 27
Pathogenic Mechanism
An article stated that the spironolactone induces an improvement of nitric oxide activity, which acts as a vasodilating agent. Another theory is the effect of spironolactone in inhibiting of angiotensin I/ angiotensin II conversion causing accumulation of kinins, with a consequent nasal vasodilation triggering aqueous rhinorrhea. 27 -29
Chlorothiazide and hydrochlorothiazide are the most popular members of the thiazide diuretic class, and they cause rhinitis as an adverse effect of use. 26
Pathogenic Mechanism
Thiazide diuretics cause the diuretic effect by blocking the sodium-chloride channel in the proximal section of the distal convoluted tubule. The sodium-potassium (Na/K) pump’s efficiency is diminished when the Na/Cl channel is blocked, and the amount of Na and water that can enter the interstitium is also decreased. A study performed in 2005 discussed a novel mechanism of how thiazide diuretics induce vasodilation. Thiazide diuretics decreased angiotensin II–induced or norepinephrine-induced vasoconstriction and caused desensitization of the vascular smooth muscle to calcium by the opening of calcium-activated potassium channels and leading to smooth muscle relaxation and vasodilation resulting in nasal congestion. 30,31
Calcium Channel Blockers
A class of antihypertensive medications is called calcium channel blockers (CCBs) that includes both dihydropyrdine (e.g., amlodipine, nifedipine), and non- dihydropyrdine (diltiazem, verapamil) type of CCBs. 5,9,11
Pathogenic Mechanism
Through inhibiting the calcium influx into vascular smooth muscle and promoting the vasodilation and consequently decreasing blood pressure. This type of medication usually causes nasal congestion as a result of mucosal interstitial edema which is assigned to the permeability change in the vasodilated blood vessels. 9,11,32
Psychotropic Drugs
A wide range of antipsychotics is used for the treatment of psychiatric disorders, such as schizophrenia, psychosis, bipolar disorder, anxiety, and depression. These medications fall into several classifications, including benzodiazepines (chlordiazepoxide, alprazolam), non-benzodiazepines (zolpidem), tricyclic antidepressants (amitriptyline), dopamine receptor blockers (chlorpromazine, thioridazine), second generation antipsychotics (risperidone), sympatholytics (reserpine), and selective serotonin reuptake inhibitors (SSRIs; citalopram).
Pathogenic Mechanism
These drugs induce rhinitis and nasal congestion due to their autonomic nervous system effects, which reduce catecholamine neurotransmitter influx like dopamine, epinephrine and norepinephrine. Some also have alpha- and beta-blocking actions, these actions associated with vascular vasodilation including vasodilation of the nasal vascular smooth muscle which is mainly associated with nasal congestion and runny nose. 9,10,33,34
Local Decongestants
The phrase “rhinitis medicamentosa” is often employed to describe a subtype of drug-induced non-allergic rhinitis caused by chronic use of local decongestant drugs. The earliest nasal decongestant derived from ephedrine, and the effect of long-term use of local decongestants, was first observed in 1931. Nasal decongestants are classified as 2 types: sympathomimetic amines (such as pseudoephedrine, phenylephrine, ephedrine, and benzedrine) and imidazolines (e.g., xylometazoline, oxymetazoline, and naphazoline).
Pathogenic Mechanism
Sympathomimetic amines stimulate sympathetic tone through the release of norepinephrine, which binds to presynaptic alpha 1 receptors to cause vasoconstriction. By contrast, imidazolines act postsynaptically by binding to alpha 2 receptors and triggering vasoconstriction and decreased blood flow by a negative feedback mechanism that lowers endogenous norepinephrine levels.
The pathogenic mechanism of rhinitis medicamentosa is still not clear. However, it is associated with the long-term use of these intranasal alpha 1 and 2 vasoconstrictors, resulting in rebound swelling and congestion. This rebound blocked nose has been referred to as a change in vascular permeability followed by interstitial edema. Further, Ramey et al. suggested that it might reflect a negative feedback mechanism that reduces the release of norepinephrine. After chronic use and then cessation, the sympathetic nerves in the nasal mucosa may lose their ability to retain vasoconstriction. 35,36
Anti-Thyroid Medications
Anti-thyroid medications including methimazole and propylthiouracil have been reported to induce rhinitis symptoms.
Pathogenic Mechanism
Long-lasting nasal congestion and excessive nasal discharge are symptoms of hypothyroidism, which causes a preponderance of parasympathetic effects. Increasing in the volume of connective tissue and enlargement of the glands that secrete mucus are responsible for the observed nasal congestion. 11
Miscellaneous Drugs
Gabapentin
Gabapentin, one of the gamma-aminobutyric acid analogs, is efficient in treating persistent neuropathic pain and seizures. Some review articles have reported that gabapentin may induce rhinitis.
Pathogenic Mechanism
The actual mechanism is unknown. Further detailed investigational studies are needed. 10,37
Hydralazine
Hydralazine which is a vasodilating agent used to treat hypertension, has been reported to cause rhinitis-like symptoms.
Pathogenic Mechanism
It acts directly on the vascular smooth muscle through the opening of potassium channels. It also prevents myosin phosphorylation inside the arterial smooth muscle and inositol triphosphate (IP3)–induced calcium release from the sarcoplasmic reticulum of smooth muscle cells. This causes vasodilation and a decrease in peripheral vascular resistance. This action may also have an impact on the nasal mucosa, causing nasal congestion as a side effect. 9,38
Discussion and Conclusion
In contrast to a systematic review, which aims to collect all pertinent material, this study’s non-systematic narrative review objective was to give a comprehensive overview of the incidence of drug-induced rhinitis, most commonly reported drugs associated with rhinitis and what pathogenic mechanism behind rhinitis induced by the identified drugs. Searches in the electronic databases of Embase and Medline (through PubMed) were carried out to cover a broad spectrum of published literature. To find pertinent published works that were not included in either database, a generic Google scholar search was also carried out.
One kind of non-allergic rhinitis is drug-induced rhinitis that has been observed abundantly in many patients who take prescribed medications for other medical conditions. Patients frequently visit the otolaryngology clinic complaining of nasal symptoms but they show negative skin allergic tests and no evident cause, that makes their diagnoses controversial and incomprehensible. Therefore, taking the patient’s medication history, along with raising the awareness of patients and physicians toward this type of rhinitis, can be very useful in the primary evaluation in the otolaryngology clinic.
There is no treatment for this type of rhinitis other than stopping the causing medications if applicable or switch to another suitable medication (e.g., switching from ACE I to angiotensin receptor blocker ARBs, from thiazide diuretics to furosemide). Clinical experiences recommend the use of intranasal corticosteroids sprays and intranasal antihistamines alone or in combination to manage drug-induced rhinitis symptoms for long term, oral or parenteral corticosteroid for short term. If a nasal blockage has developed and being unresponsive to medical intervention, it may be necessary to treat this permanent alteration surgically. However, further clinical studies are needed to prove their efficacy and safety in chronically ill patients.
It is hoped that this review study can aid in making the correct diagnosis and providing suitable medical intervention for healthcare specialists in particular physicians and pharmacists treating patients with the different types of rhinitis. Knowing the mechanism of medicines induced rhinitis help physicians to treat the cause. For example, most of these drugs mechanism lead to the same end result, vasodilation such as alpha and beta blockers, PDE5 inhibitors and calcium channel blockers, which in turn causes nasal congestion, in this case local decongestant is the suitable choice. Other drugs may lead to histamine release such as ovarian hormonal agents or ACEIs and reversed by antihistamines. NSAIDs may result in overproduction of leukotrienes that controlled by antileukotriene or corticosteroids.
While certain medications that cause this disorder are known to induce rhinitis via a recognized mechanism, the pathophysiology of other medications is still unknown. However, healthcare specialists who encounter patients with rhinitis and rhinitis-like symptoms are encouraged to take all the reported medications used by patients into consideration when treating and diagnosing the reason for nasal congestion and rhinitis-like symptoms.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.