
Abstract

Significance Statement
Masses occupying the retrolabyrinthine space are uncommon and most often represent paragangliomas, choroid plexus papilloma, endolymphatic sac tumors (ELSTs) or distant metastasis. ELSTs are rare, locally invasive tumors of the inner ear, with less than 300 cases reported in the literature. ELSTs are associated with von-Hippel Lindau (VHL) disease. Patients diagnosed with an ELST should undergo genetic testing for VHL disease, and individuals with confirmed VHL disease should be screened for ELST(s).
Case Report
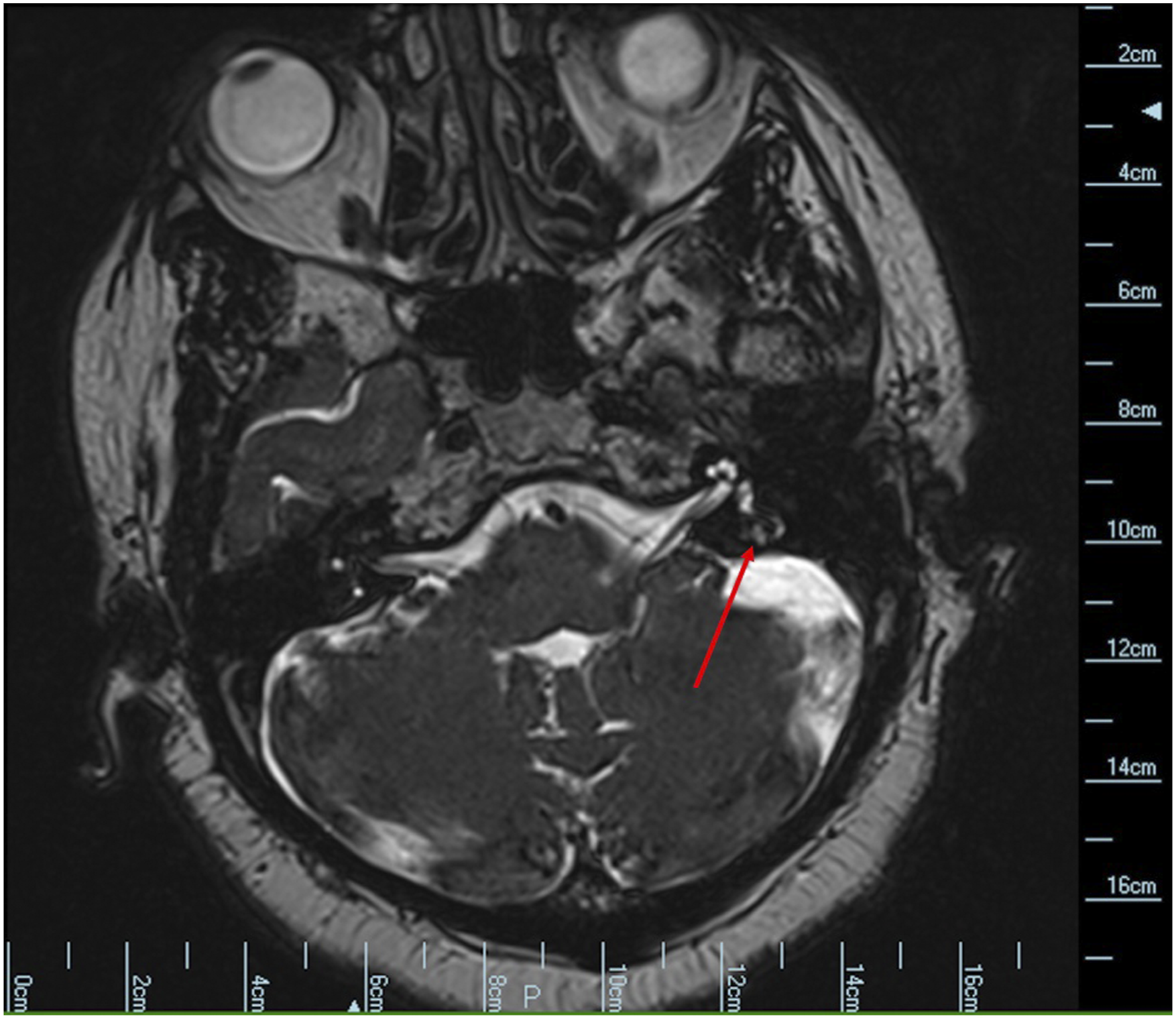
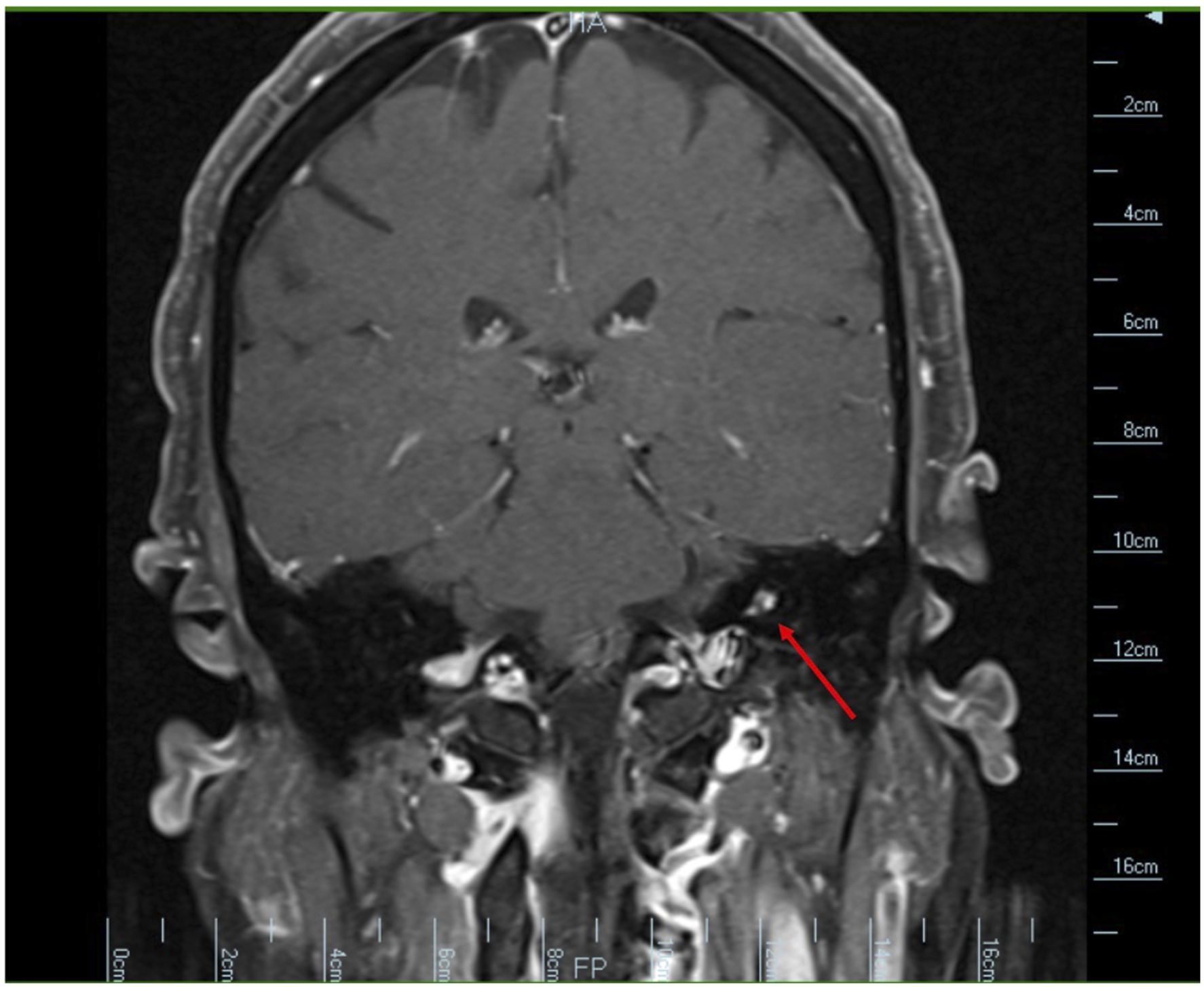
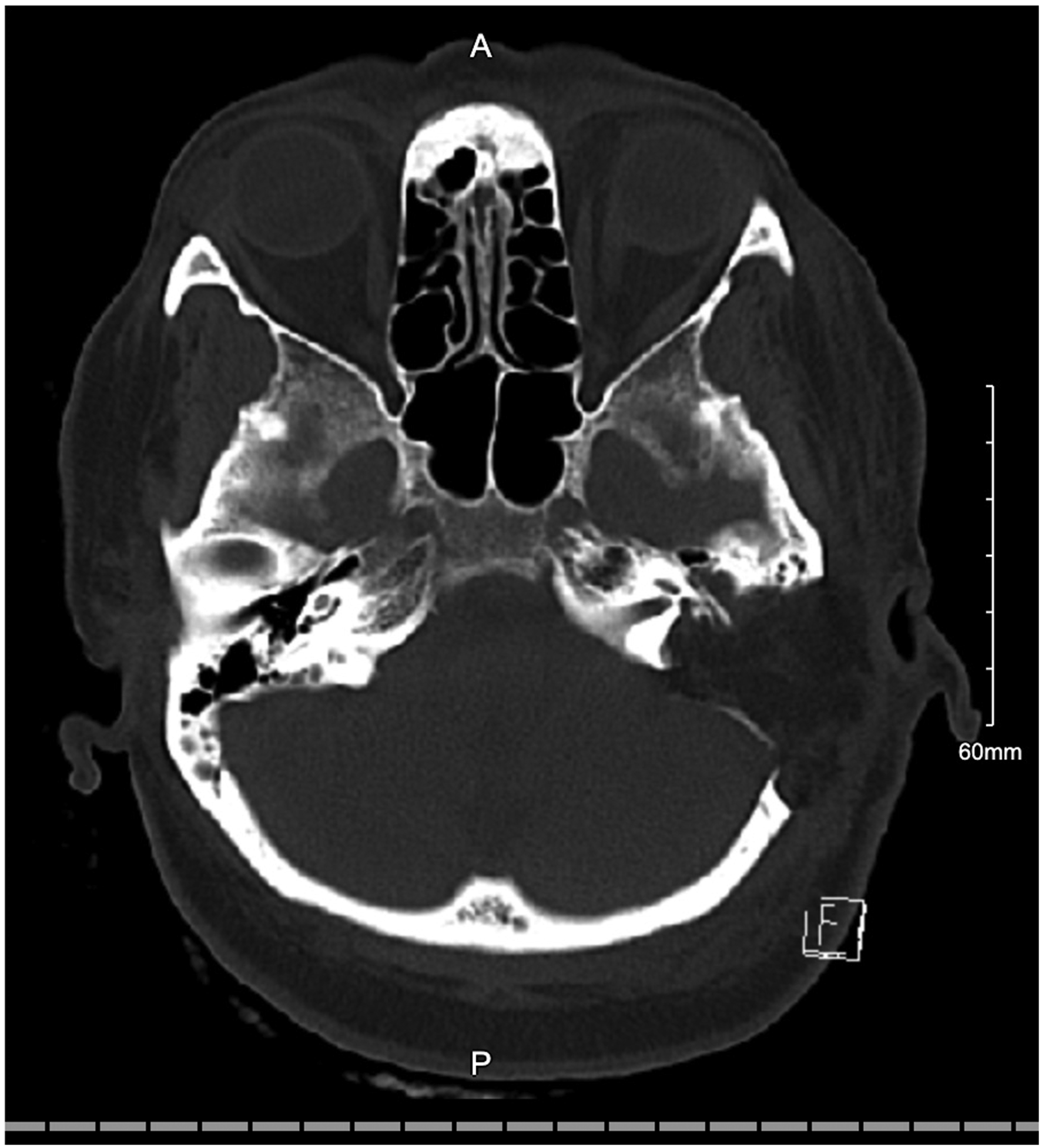
A 65 year-old woman presented with unilateral hearing loss, non-pulsatile tinnitus, intermittent aural fullness and otalgia progressive over a 5-month period. She did not complain of vertigo or other audiovestibular symptoms, nor did she have a history of recurrent ear infections, loud noise exposure or family history of hearing loss. Rinne testing using a 512 Hz tuning fork could not be performed on the affected side as the patient could not hear bone or air conduction. Otherwise, otologic examination was unremarkable. Audiometric testing revealed severe-to-profound sensorineural hearing loss in the affected ear (left) with no discernable speech discrimination. She also had mild high frequency sensorineural hearing loss in the contralateral ear. Serologic testing revealed HLA-Cw7, a marker for increased risk of autoimmune inner ear disease, but was unremarkable otherwise. Temporal bone computed tomography (CT) with contrast revealed a 3.0 × 4.4 × 4.0 mm (AP × TRV × CC) expansile, lytic lesion in the left proximal vestibular aqueduct (Figure 1). Magnetic resonance imaging (MRI) of the internal auditory canals (IACs) with contrast revealed an enhancing mass near the region of the endolymphatic sac with surrounding osseous erosion (Figures 2 and 3). Videonystagmography (VNG) showed reduced responses bilaterally for fast gain on optokinetic testing. Caloric tests revealed clinically insignificant right-sided weakness. The patient was diagnosed with a suspected left-sided endolymphatic sac tumor (ELST). Preoperative axial computed tomography temporal bone with contrast revealing an asymmetric expansile lytic lesion in the proximal left vestibular aqueduct measuring 3.0 × 4.4 × 4.0 mm (AP × TRV × CC). Preoperative axial T2-weighted magnetic resonance imaging of the internal auditory canals reveals an enhancing mass in the region of the left endolymphatic sac. Preoperative coronal T1-weighted magnetic resonance imaging of the internal auditory canals with contrast reveals an enhancing mass in the region of the left endolymphatic sac.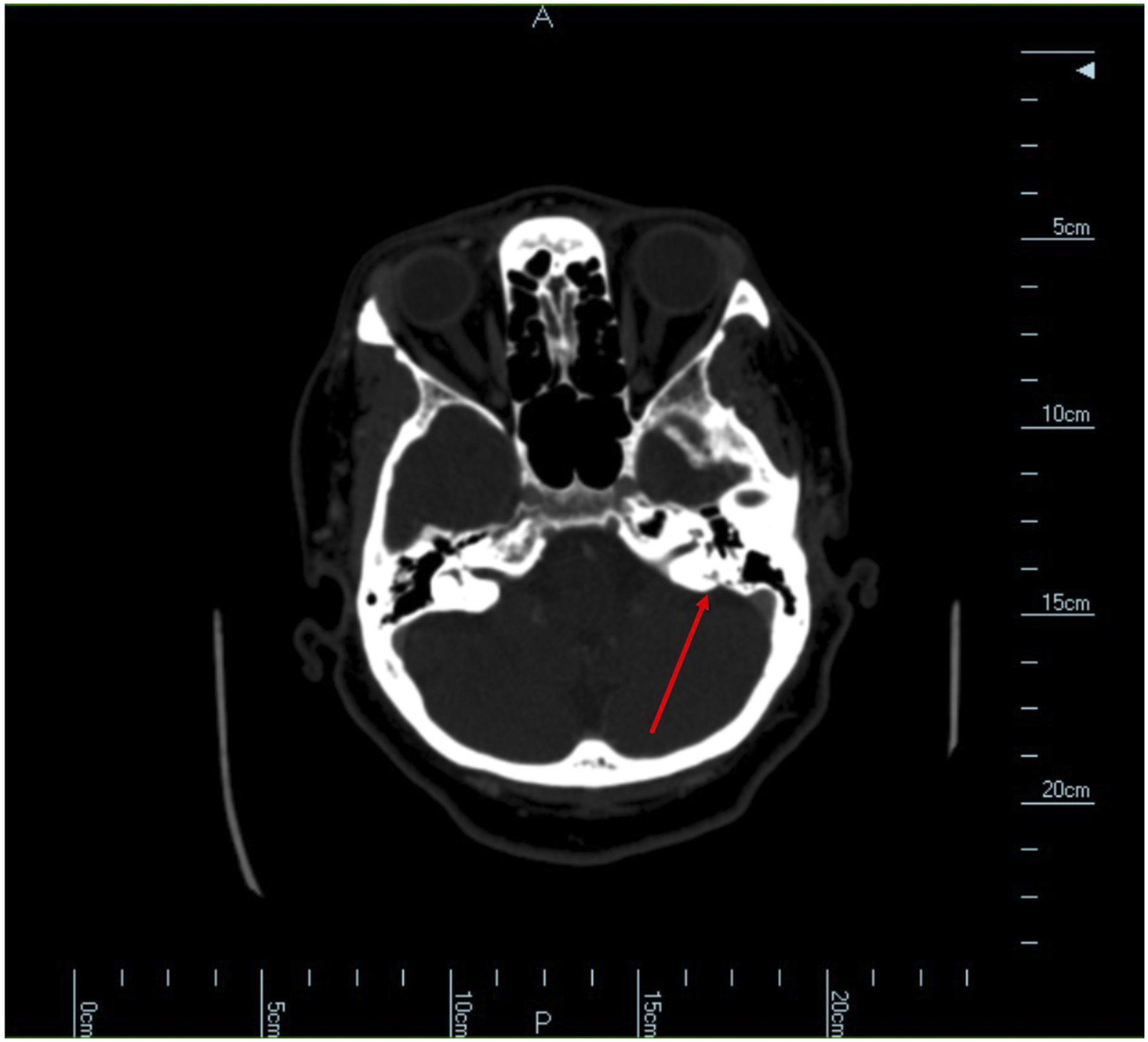
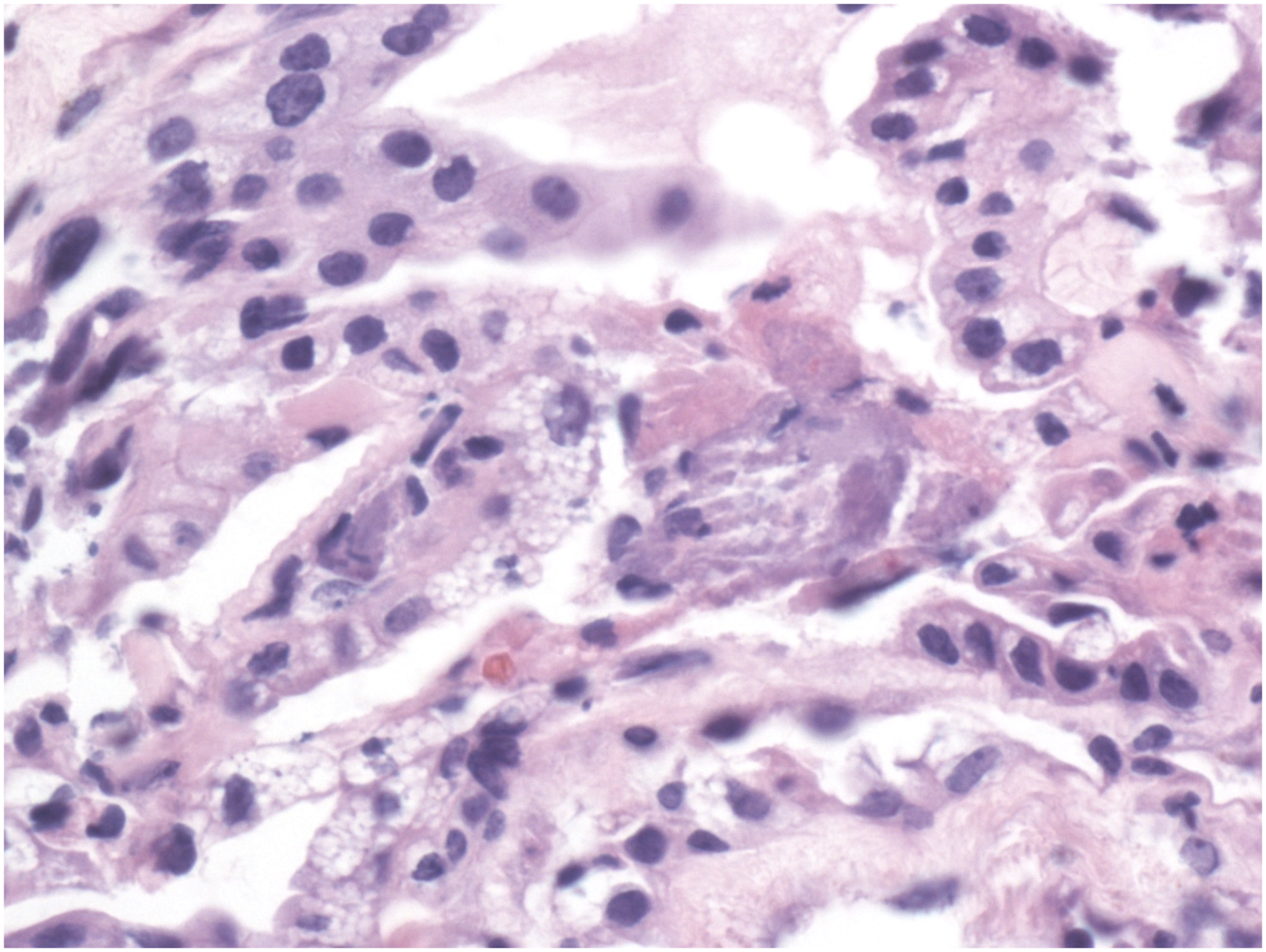
The patient underwent excision of the endolymphatic sac mass using a translabyrinthine approach. Surgery revealed a tan, irregular mass in the region of the endolymphatic sac (Figure 4). A postoperative CT of the head without contrast revealed expected postoperative changes without evidence of residual tumor (Figure 5). Pathology showed papillary epithelium with epithelial cell proliferation composed of cuboidal-appearing cells with uniform, small, round-to-oval hyperchromatic nuclei and eosinophilic-to-clear cytoplasm with indistinct cell membranes. There was no significant nuclear pleomorphism or increased mitotic figures, and there was no tumor necrosis (Figure 6). The neoplastic cells were positive for cytokeratin-7, vimentin, neuron specific enolase, CAIX and PAX8. The findings were consistent with a histologically benign endolymphatic sac tumor. These findings did not reveal malignancy, although ELSTs are commonly low-grade adenocarcinomas.
1,2
Testing for von-Hippel Lindau (VHL) disease did not reveal any genetic abnormalities. Intraoperative picture revealing a tan appearing mass in the retrolabyrinthine space (arrow). Postoperative axial computed tomography head without contrast showing postoperative changes without evidence of residual endolymphatic sac tumor. The prior defect and eustachian tube are occluded with abdominal fat. Histopathologic section revealing neoplastic epithelial proliferation with a cystic and papillary architecture. There is a single layer of cuboidal cells with small, round-to-oval, hyperchromatic nuclei, irregular nuclear contours, occasional indistinct nucleoli and pale eosinophilic-to-clear vacuolated cytoplasm. Cell borders are variably distinct. Nuclear pleomorphism, increased mitotic figures and necrosis are absent (photomicrograph was taken at 40× magnification).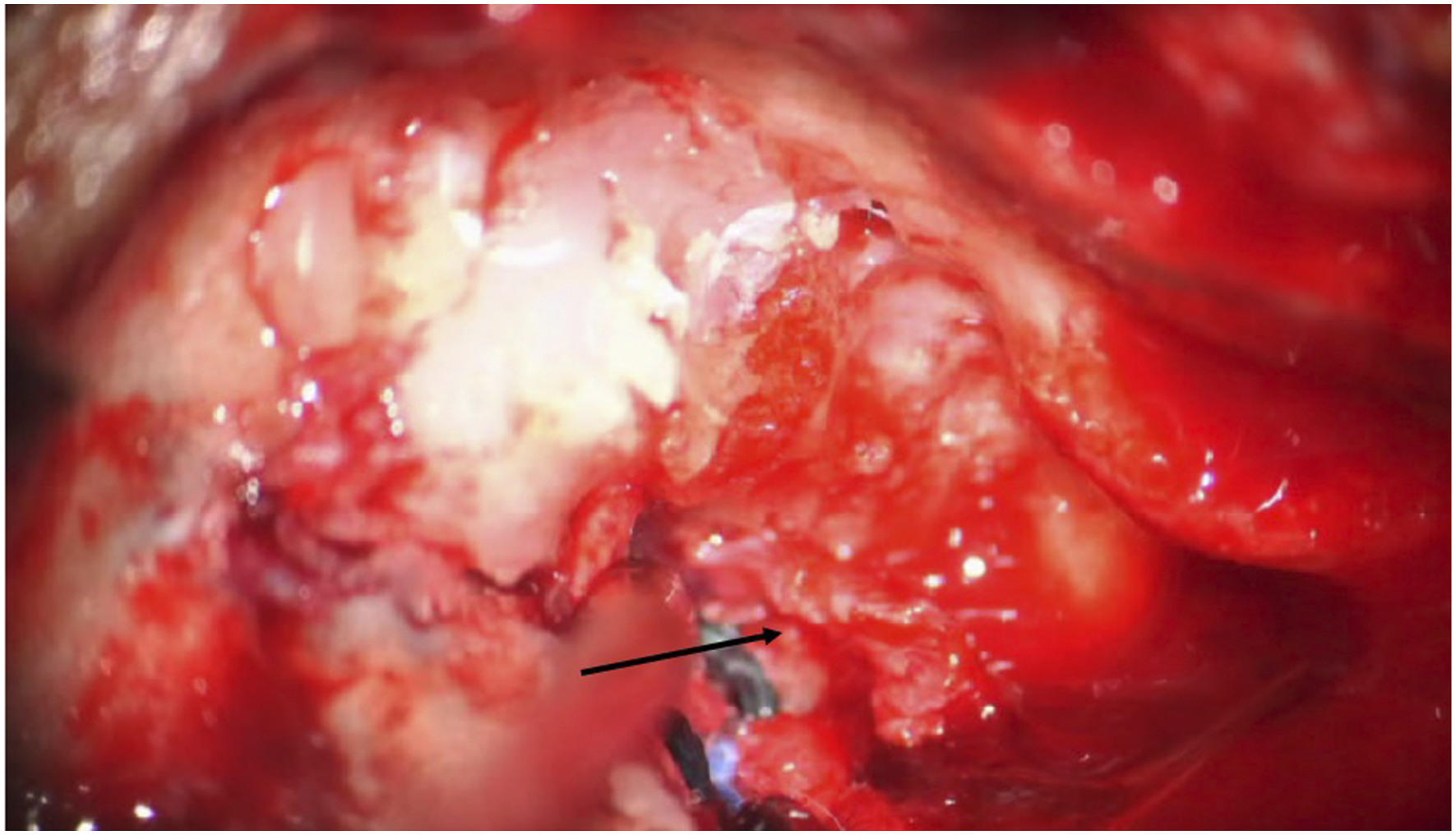
ELSTs are rare, locally invasive, slow-growing and low-grade neuroectoderm tumors of the temporal bone with less than 300 reported cases in the literature. 3 ELSTs occur sporadically or in association with VHL disease. Sporadic cases of ELSTs typically occur during the fifth and sixth decades of life, whereas ELSTs associated with VHL occur earlier in life with a higher incidence in females; and they present bilaterally 30% of the time. 2,4 Individuals with VHL disease have a 5–20% chance of developing an ELST. 4 Patients diagnosed with VHL disease should undergo audiometric testing at the time of diagnosis, and every two years thereafter to screen for the development of an ELST. Patients commonly experience sensorineural hearing loss, aural fullness, tinnitus and vertigo. 5 CT imaging of the temporal bones most commonly reveals an osseous lesion in the retrolabyrinthine space with bony erosion extending into the posterior fossa and/or middle ear. 6 MRI of the IACs typically reveals a slightly hyperintense lesion in the retrolabrythine space on T1-weighted imaging that is isointense on T2-weighted imaging. 6 Paragangliomas, choroid plexus papilloma and metastatic diseases should be included in the differential diagnosis of a retrolabyrinthine lesion. Histologically, ELST commonly is described as cystic and/or papillary with rare mitotic figures or pleomorphism and absence of necrosis. 4,6 ELSTs are positive for cytokeratin, protein S100, and epithelial membrane antigen and negative for chromogranin and synaptophysin. 6 Genetic testing for VHL disease is recommended for all individuals diagnosed with an ESLT. VHL disease is an autosomal dominant disorder caused by a mutation of the VHL tumor suppressor gene located on chromosome 3p25. 5 Patients with VHL disease are at increased risk of benign tumors of the central nervous system, inner ear, retina, adrenal glands and pancreas. ELSTs tend to be locally aggressive with no reported cases of metastasis. Complete surgical excision is the primary treatment with radiation therapy utilized for an incompletely excised tumor or recurrence. The most common cause of recurrence is inadequate resection of involved dura. 2 Although rare, clinicians should be aware of endolymphatic sac tumors and understand their locally destructive properties.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.