
Abstract
Cervical necrotizing fasciitis (CNF) is a rare infection that can quickly lead to devastating patient outcomes. Considering the vital importance of surrounding neck structures, rapid control of the infection is essential. Infection is most frequently polymicrobial and occurs in the adult patient in the context of certain medical comorbidities. Complications are typically limited to tissue destruction in the form of necrosis. There are no current reports describing CNF complicated by acute shock in the post-operative pediatric patient. Here, we present a pediatric case of CNF complicated by acute shock following Sistrunk procedure for removal of a supposed thyroglossal duct cyst. This case illustrates a potential post-operative complication that can be seen within the pediatric patient. Although most reported examples of CNF are polymicrobial and result from odontogenic infection, providers should be aware of other potential sources of disease. It is important for the pediatric surgeon to rapidly identify CNF and consequent shock, as prompt medical and surgical interventions are critical to offering the best chance of patient survival.
Introduction
Necrotizing fasciitis is a severe infection of the subcutaneous soft tissue and fascia. Involvement of the head and neck region is particularly uncommon but associated with a mortality rate approaching upwards of 50%.1-3 Head and neck necrotizing fasciitis can be classified as either cervical or craniofacial. In cervical necrotizing fasciitis (CNF), the infection is most often odontogenic in origin, such as following tooth extraction.1,4,5 As such, these infections are frequently polymicrobial and involve both aerobic and anaerobic organisms. 6
Control of the infection is crucial to patient management and usually involves rapid surgical intervention with debridement of necrotic tissue. Because of the vital importance of many surrounding neck structures, patients with CNF must be closely monitored for complications including airway obstruction and vessel thrombosis. In only a few reported instances, complications in the form of septic or toxic shock have been described. 7
Most examples of CNF within the literature are limited to adult populations.3-5,7-9 Examples of CNF within the pediatric population are uncommon. In this report, we describe a case of CNF with resultant acute shock occurring as a post-operative complication within a pediatric patient.
Case Report
Written consent was provided from the child’s parental guardian (legally authorized representative) for publication of patient information and images.
A 3-year-10-month old male was seen in the pediatric otolaryngology clinic with a chief complaint of an anterior neck mass. He had no significant past medical history. An ultrasound of the neck was obtained and showed a 1.1 × 1.5 × 0.6 cm lesion in the subcutaneous soft tissue of the neck, superior to the thyroid gland. This was consistent with a thyroglossal duct cyst. The patient was then scheduled for a Sistrunk procedure, which was performed uneventfully. A Penrose drain was placed at the conclusion of the case.
On post-operative day (POD) 1, the patient was in good spirits with adequate oral intake, stable vital signs, and an appropriate-appearing wound. There was still a fair amount of serous fluid emanating from the Penrose drain so the decision was made to leave it in place for another evening. Early on POD 2, the patient developed nausea, vomiting, and diarrhea which rapidly progressed to tachypnea, tachycardia, and hypotension. Multiple intravenous fluid boluses of 0.9% sodium chloride were unable to maintain his blood pressure. Consultations were placed to pediatrics, infectious disease, and intensive care. The patient was transferred to the pediatric intensive care unit (PICU), initially placed on bilevel positive airway pressure (BiPAP) but was then subsequently intubation. Inotropic agents were administered to maintain his blood pressure.
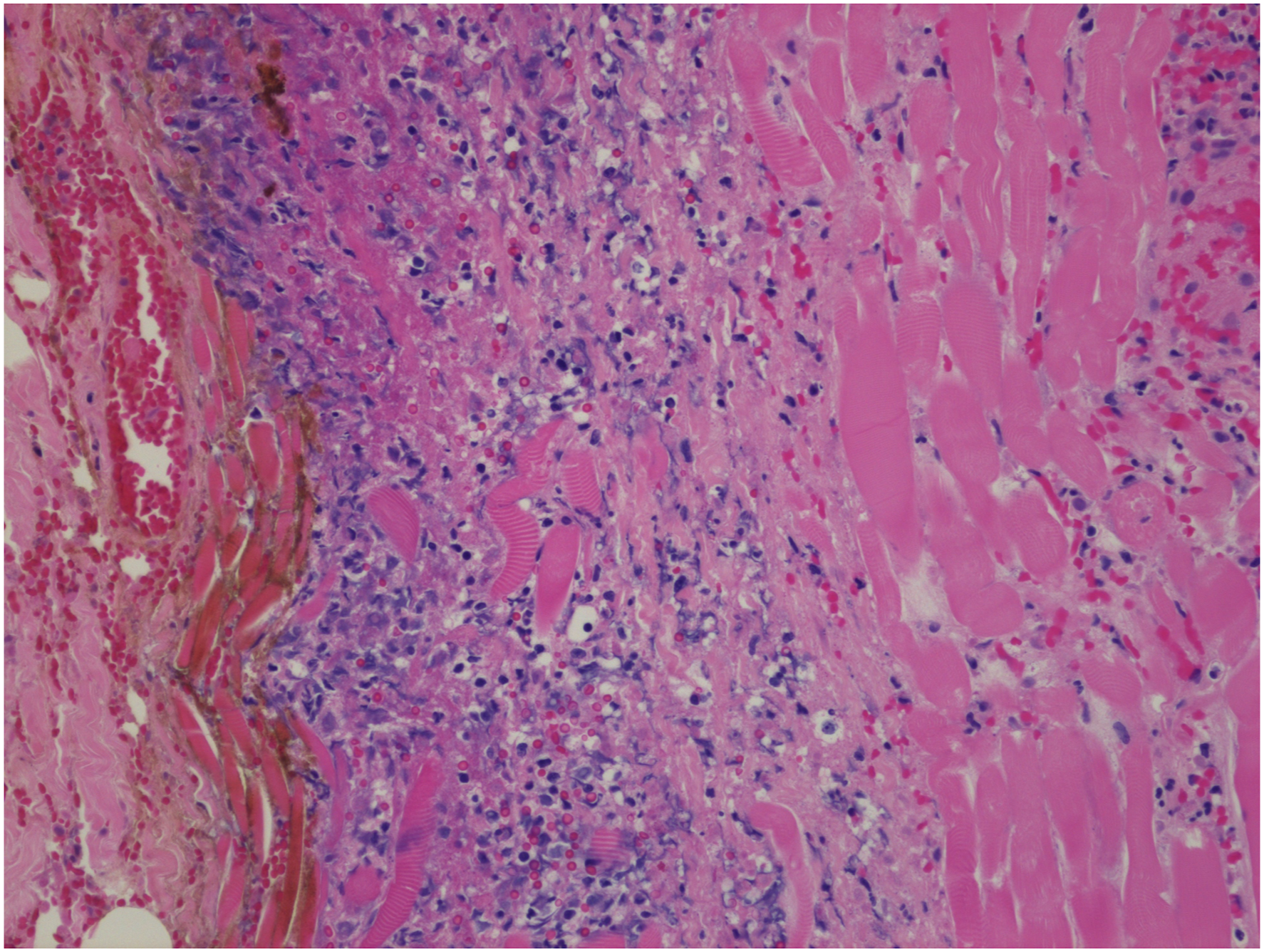
The wound was inspected (Figure 1A) and was then opened at the bedside within the PICU, as the patient was too hemodynamically unstable to be transferred to the operating room. The Penrose drain was removed. Empiric antibiotic coverage with cefepime, vancomycin, and clindamycin was initiated. The patient was found to have devitalized tissue with necrotic skin edges consistent with necrotizing fasciitis. Limited debridement was performed secondary to his hemodynamic instability. Tissue samples were sent to pathology and microbiology (Figure 2). The histologic specimen showed extensive necrosis and acute inflammation. Cultures obtained showed gram-positive cocci in clusters. Post-operative cervical necrotizing fasciitis. (A) Initial surgical wound with necrotic skin edges after Penrose removal. (B) Wound with ongoing fibrinous and necrotic debris preceding second wound debridement. (C) Wound before closure following wound VAC removal and final tissue debridement. Fibroadipose tissue and muscle with extensive necrosis, exudate and acute and chronic inflammation consisting of lymphocytes, plasma cells, and neutrophils. Focal vessels show congestion, thrombosis, and inflammatory cells within the vascular media.
The patient was then taken to the operating room again on POD 3 to undergo a second stage of wound debridement (Figure 1B). Necrotic skin edges and strap muscles were excised, and the wound was copiously irrigated. Wet-to-dry packing was employed for ongoing wound care. Final wound cultures grew methicillin-sensitive Staphylococcus aureus (Staph. aureus), explaining the patient’s acute hemodynamic instability as likely the result of Staphylococcal Toxic Shock Syndrome (TSS). Antibiotics were de-escalated to cefazolin and clindamycin.
By POD 7, the patient had improved hemodynamically and was weaned from pressors. On POD 9, the patient returned to the operating room for a third debridement. Minimal further fibrinous tissue was excised. No new necrotic tissue was present. The wound was copiously irrigated with normal saline using a PulsaVac® (Zimmer BioMet). Instrumentation for wound vacuum-assisted closure (VAC) was then placed. The patient was successfully extubated on POD 9, and antibiotics were de-escalated further to cefepime alone. Enteric feeds were advanced. On POD 15, the patient was taken for wound irrigation, wound VAC removal (Figure 1C), and wound closure. The patient was discharged home on POD 24 after completing intravenous antibiotics. The final pathologic diagnosis of the neck mass was a dermoid cyst.
Discussion
Since its initial description in 1871 by Jones et al., 10 necrotizing fasciitis remains an illness that is associated with significant morbidity and mortality. Areas that are more frequently traumatized or those with reduced vascular perfusion are at particular risk. These regions include the extremities, abdominal wall, or perineum. Certain chronic diseases are also implicated as risk factors for the development of infection, including diabetes mellitus, chronic obstructive pulmonary disease (COPD), or certain autoimmune conditions.3,7 As a result, most cases of necrotizing fasciitis are seen in adults, and examples within pediatric patients are scarce.
Cervical necrotizing fasciitis occurs infrequently. The vast majority of cases arise from odontogenic infections.1,4 As a result, CNF is most typically polymicrobial and consists of both aerobic and anaerobic species from normal mucosal flora. 9 Other reported sources include cervical adenitis, tonsillar infections, or salivary gland infections.11,12 There are no studies to date suggesting that patient outcomes correlate with certain bacterial strains. However, upon literature review, it appears that there are very limited examples of CNF where Staph. aureus was isolated as the only causative organism. Since this bacterial strain is a common constituent of the normal skin flora, it is likely the patient we describe acquired his infection through auto-inoculation from surrounding skin.
Examples of CNF occurring post-operatively are also limited. Hadzibegovic et al. 8 described 2 adult patients who acquired polymicrobial CNF following total laryngectomy and selective neck dissection for squamous cell carcinoma. Chung et al. 11 described a child who acquired CNF following expansion laryngotracheoplasty for the treatment of subglottic stenosis.
Once infection reaches the subcutaneous soft tissue, it can spread rapidly, dissecting along or even deep to fascial planes. Rarely, advanced infection may lead to bony involvement. 3 When CNF occurs deep to the investing fascia enveloping the strap muscles, the pretracheal fascia may become involved. The pretracheal fascia extends inferiorly from the hyoid bone to just above the pericardium. Therefore, CNF occurring within this region can rarely be complicated by thoracic extension and concurrent necrotizing mediastinitis.1,13 In these instances, imaging with computed tomography may be useful for determining the extent of the infection.
Without rapid control of the infection, CNF can also involve other vital surrounding structures. Edema as a result of tissue necrosis or post-operatively from debridement can lead to airway obstruction and may require intervention in the form of tracheostomy. 3 Infection may also spread to surrounding vasculature, resulting in vessel rupture or thrombosis.9,14 Aside from supportive measures and early broad-spectrum antibiotic therapy, proper wound care is essential to promote healing. In many instances, multiple rounds of wound debridement are necessary.3,4 Wound debridement initiated within the first 24 hours has been associated with improved morbidity and mortality.5,15 Additional treatment options that may improve patient outcomes include the use of hyperbaric oxygen therapy.4,15
Aside from tissue necrosis, the infection seen in our case example was further complicated by the development of acute shock. Toxins produced by certain bacterial strains can lead to a cascade of immunologic events culminating in features characteristic of toxic or septic shock. The most frequently cited organisms responsible for TSS include Staph. aureus and Group A Streptococcus pyogenes. It is critical to recognize the features of TSS early in disease development. Mortality rates in the context of necrotizing fasciitis approach upwards of 60%. 16 Similar to the patient we describe, early multisystem complaints can include nausea, diarrhea, tachycardia, and fever. 17 Rapid progression to acute hypotension is characteristic and can often lead to multisystem organ failure. Intubation is often necessary to maintain respiratory function, as was in our case example. Supportive measures including IV fluids and pressors are also frequently required to maintain arterial pressure.
Conclusion
The infection seen in CNF can result in rapid tissue destruction and is associated with high morbidity and mortality. Although most examples of CNF are polymicrobial and occur as a result of odontogenic infection, providers should be aware of other potential sources of infection. Within the post-operative period, normal skin flora including Staph. aureus may infect the wound and be implicated as a potential cause of CNF. Unlike other bacterial strains, toxins produced by Staph. aureus can result in acute hemodynamic compromise and multisystem organ failure in the form of TSS. It is important for the pediatric surgeon to be informed of this potential complication, as prompt medical and surgical interventions are critical to offering the best chance of patient survival.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author’s Note
This manuscript has been previously presented as a poster at the American Society of Pediatric Otolaryngologists 2022 and Research Month 2022 at Children’s Mercy Hospital.