
Abstract
Nocardia is regarded as an opportunistic pathogen primarily affecting the respiratory system, whereas Nocardia farcinica is the species of the Nocardia family that is most frequently blamed for central nervous system impairment. The authors present the first case of mastoiditis caused by Nocardia farcinica, accompanied by intracranial complications. An immunocompetent 74-year-old woman who reported a three-week left ear discharge and a two-week facial nerve palsy was referred to our department. MRI revealed mastoiditis and epidural abscess. The bacterial cultures obtained during the surgical management of the patient confirmed the presence of Nocardia farcinica. Targeted antibiotic therapy was subsequently administrated, gradually resulting in favourable outcomes. Nocardia species provoke a disseminated infection that emerges not only among the immunosuppressed individuals but can also affect the healthy population. The nonspecific clinical manifestations in addition to the difficulties identifying the pathogen, remain obstacles to a punctual diagnosis. However, the combination of surgical debridement and antibiotic treatment with trimethoprim and sulfamethoxazole is considered the most appropriate management, leading to propitious results.
Introduction
First described by Edmond Nocard in 1888, Nocardia is a Gram-positive and catalase-positive aerobic bacterium that is considered to be an opportunistic pathogen of the order of Actinomycetes. 1 Since 1888, more than one hundred Nocardia species have been recognised, of which 54 species have been cited as being capable of infecting humans. 2 As Nocardia is widely distributed in nature, most commonly living as a soil saprophyte, its spores can be either inhalated or induced percutaneously through skin breakdown, provoking a wide variety of clinical manifestations, especially in immunosuppressed individuals who are the most prone to contamination. 3 Nocardiosis is usually presented as pulmonary inflammation, caused mostly by Nocardia asteroides, which can be easily spread to multiple sites through the haematogenous route, leading to a so called ‘disseminated’ disease, where two or more separated organs are involved. Specifically, the central nervous system and the skin appear to be the most likely to be affected, following a respiratory tract infection. 4
Even though seldom identified in everyday clinical practice, Nocardia farcinica is the a of the Nocardia family that is most frequently blamed for central nervous system impairment, primarily presenting as brain abscess or meningitis.4,5 It is characterized by high mortality rates, ranging from 20% to 55%, depending on the immunodeficiency status of the patient. In addition to the underlying disease, difficulties in identifying the pathogen along with the inherited resistance of Nocardia farcinica to common antimicrobial agents, result in delays in the initiation of appropriate treatment initiation, reducing the chances of complete recovery.5,6
According to the international literature published in English, very few cases of ear disease caused by Nocardia species have been reported. Furthermore, no cases of mastoiditis due to Nocardia farcinica have been reported.7-9 In the present study we report the case of an immunocompetent woman, who developed Nocardia farcinica mastoiditis accompanied by facial nerve palsy and epidural abscess. The main aim of this study is to emphasize that Nocardia farcinica can affect immunocompetent patients, presenting with quite mild initial symptoms, as well as members of the immunosuppressed population. A secondary aim is to improve ear infection management by providing clinical advice concerning diagnosis and treatment modalities. This report has been approved by the Ethics Committee of the Pirkanmaa Hospital District. The patient has provided written consent for publication of the case details and related images.
Case Report
A 74-year-old woman, with a 11-year history of bilateral glue ear, high blood pressure and hypothyroidism, was referred to the local hospital due to earache in the left ear and a lightly bloody ear discharge, which had started three months earlier. Antibiotic therapy with 160mg of sulfadiazine and 500 mg of trimethoprim twice a day per os was used to treat patient’s ear condition, leading to earache amelioration. A few weeks later, symptoms of left facial nerve palsy arose, mainly encountered in the distribution area of the zygomatic and buccal branches (the forehead was spared). In addition, there was a left side conductive hearing loss of the low and high frequencies (from 60 dB at 250 Hz to 30 dB at 1000 Hz and from 30 dB at 2kHz to 80 dB at 8 kHz) and a sensorineural hearing loss of the high frequencies (from 30 dB at 3 kHz to 50 dB at 8 kHz). Findings lead to a left ear myringotomy and tympanostomy that eventually did not improve the patient’s clinical image. Following the tympanostomy, no drainage from the ear was observed. However, ear discharge was present the following day. High Resolution Computed Tomography (HRCT) of the temporal bone and Magnetic Resonance Imaging (MRI) of the brain and skull base revealed mastoiditis, petrous apicitis and a 6x2 mm epidural abscess, posteriorly from the petrous apex (Figure 1). Gradually, the patient developed a headache, while blood pressure was significantly elevated (RR 218/114 mmHg) and low fever was also reported. Subsequently, the patient was emergently referred to our University Hospital. MRI scan of the admission day in our department: showing the epidural abscess posteriorly to the petrosal apex (indicated by the white arrow).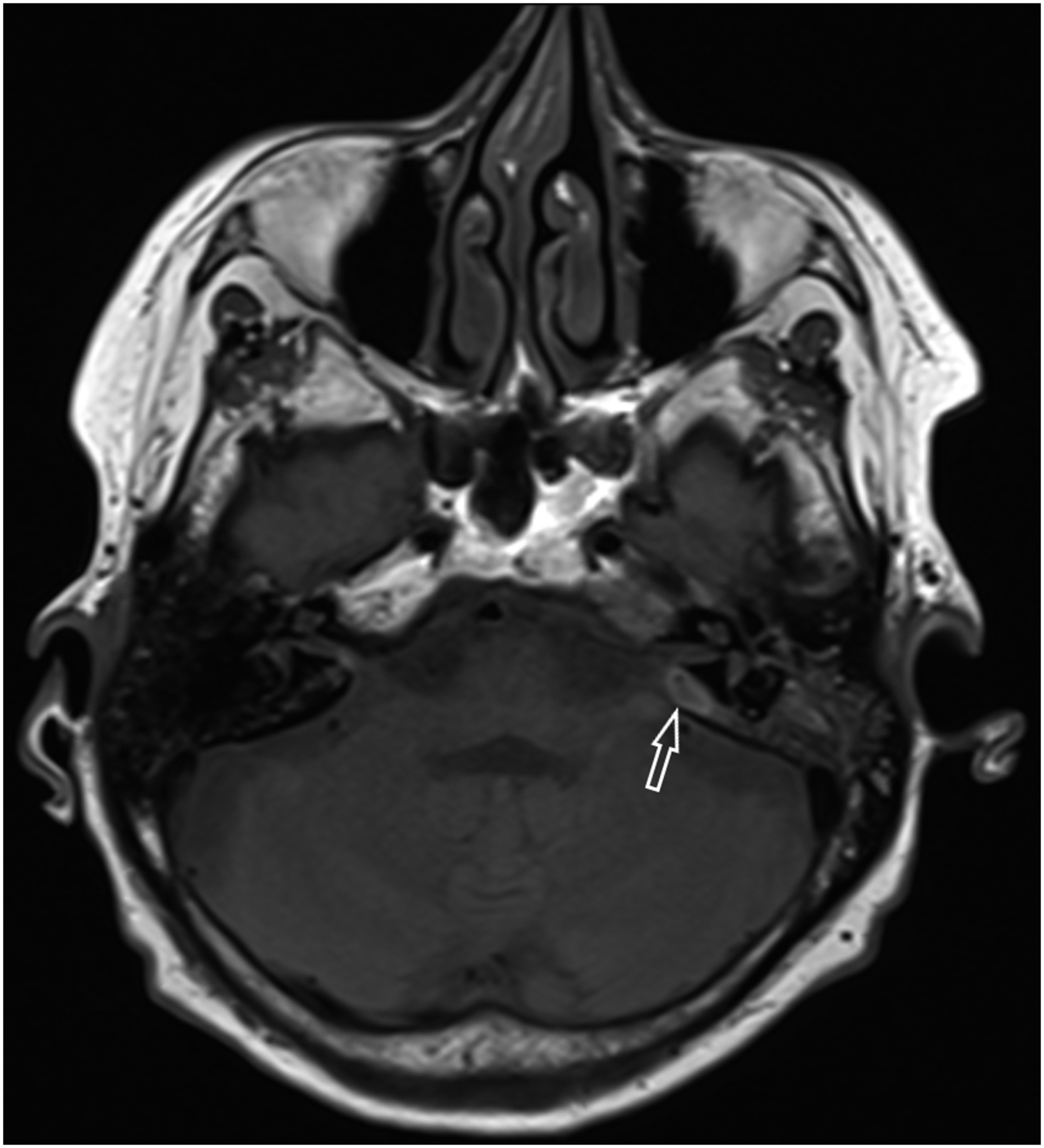
During clinical examination there was purulent secretion of the left external auditory canal, whose bacterial culture showed normal flora development, redness and tenderness of the left postauricular area, as well as conductive hearing loss. No evidence of pulmonary disease was encountered on physical or imaging examination. Neurosurgeon and infectious diseases specialists were also consulted about this patient. Since the patient was alert, afebrile without any neurological impairment and blood tests weren’t alarming (WBC = 4.6 x 109/L, CRP = 2mg/l, normal range: 0–10 mg/l), conservative treatment with intravenous ceftriaxone (2g x 2 iv), ciprofloxacin with fluocinolone acetonide ear drops (3mg/ml +0,25mg/ml, 6 drops twice per day) and a tapering schedule of prednisolone per os (starting from 60mg per day) was suggested. The patient was discharged from ENT ward after 6 days and facial palsy was significantly improved by then. Consequently, she was transferred to regional hospital’s ward for few days, till she was allowed to continue with per os antibiotic treatment at home. A control MRI scan was arranged for the patient 3 weeks later.
Follow-up MRI scan revealed the persistence of epidural abscess. Moreover, the patient’s symptoms worsened, since her headache and hearing deteriorated, dizziness appeared and blood test showed increased inflammatory markers (CRP = 60 mg/l). As a consequence of this clinical status exacerbation, the patient was readmitted in the ENT department. Subsequently, left tympanomastoidectomy was conducted and route to pars petrosal was opened posteriorly to the labyrinth, followed by a two-week treatment with ceftriaxone. A new MRI was performed two weeks later, revealing extensive osteitis of the temporal bone and skull base, whereas no visible epidural abscess was detected. Even though an initial improvement was evident postoperatively, symptoms of headache, ear congestion and drainage reappeared.
Thus, a revision mastoidectomy was performed under sedation and local anaesthesia, due to severe hyponatraemia, and abundant granulation tissue was detected. Tissue samples were taken and sent for histopathology examination. Additionally, extensive testing for immunodeficiency disorders was conducted. For example, the patient was tested negative for IgG-4 related diseases, ANCA antibodies, Tuberculosis, CD138-Immunohistochemistry, IgG and Acid-Fast Bacillus staining. Cultures collected during the revision operation were highly suggestive of Nocardia farcinica development and antibiotic treatment with sulfamethoxazole/trimethoprim and ceftriaxone parenterally (2 gr x2 iv) was administered, followed by sulfamethoxazole/trimethoprim (160/800 mg x3 iv) and amoxicillin/clavulanic acid for a period of 7 months. Thereafter, treatment was stopped due to deteriorating renal function.
Despite the prompt after surgery clinical amelioration, symptoms, such as ear congestion, headache, dizziness and fatigue, reoccurred progressively once antibiotic therapy was discontinued. Thus, nine months postoperatively (16 months after the first admission) a new MRI scan was obtained, where, an oval, well-defined fluid collection of the mastoid area was presented (Figure 2). A mastoid exploration was performed to investigate the new imaging findings. Fortunately, only a seroma accompanied by scar and granulation tissue was found, while the cultures retrieved were negative for bacteria, including Nocardia species. Two weeks later, the patient was examined in the outpatient clinic and her condition had improved. Nevertheless, hearing loss was still present and hearing aid rehabilitation is scheduled. Regretfully, the patient’s chronic headache was not improved completely. Nine month postoperative MRI scan: showing a seroma in the operated mastoid cavity (indicated by the white arrow).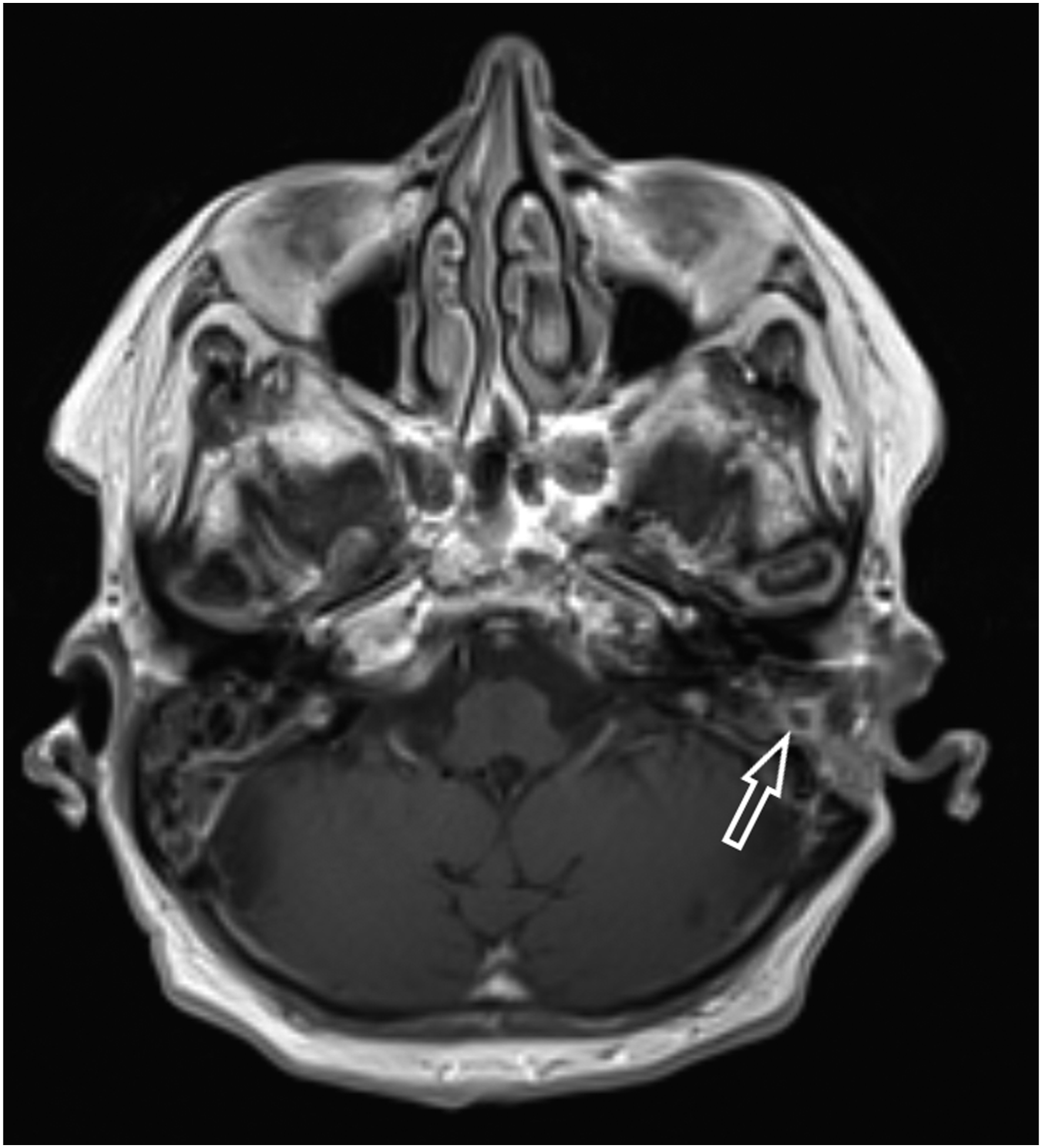
Discussion
Nocardiosis is a granulomatous suppurative infection, of multiple manifestation. 1 Although the host’s immune status probably constitutes the most important predisposing factor for infection, approximately in one-third of the cases nocardiosis occurs in healthy individuals without an acknowledged underlying immunocompromising condition. 10 Indeed, no evidence of immunosuppression was detected in the patient reported in the present study.
As far as its clinical presentation is concerned, nocardiosis usually emerges as pulmonary inflammation, provoked by the inhalation of bacterial spores. Subsequently, foci from the respiratory tract can spread through the human body by haematogenous dispersion. 11 The central nervous system lies among the organs that are primitively impaired, whereas Nocardia farcinica is more prone to affect the brain in comparison to other species. Ear infections caused by Nocardia are rare. To our knowledge, only six cases of acute otitis media and mastoiditis have been described in the literature published in English, and most of them have been associated with intracranial complications, corresponding to the present case report.7-9,12-14 Specifically, the patient presented in the current study is the only known case of an immunocompetent individual developing isolated mastoiditis due to Nocardia farcinica, leading to a brain abscess without any sign of preceding pulmonary contamination.
Ordinarily, upon inoculation, nocardia develops a modest inflammatory response, resulting in mild symptoms that are usually not significant enough; hence, they do not indicate the severity of the latent infectious disease. 15 Indistinct signs of fever, cough, fatigue, chest pain, regarding pulmonary nocardiosis or headache, confusion and ataxia, when the central nervous system is afflicted, in many instances can trick clinicians into taking the wrong diagnostic direction. Thus, imaging testing, which is highly recommended, especially for immunocompromised patients, along with the identification of the pathogen, can provide adequate evidence for the clinicians to suggest nocardiosis.7,16 In particular, Nocardia culture growth, although time consuming (it takes more than two weeks for some species to grow), in combination with histological examination of tissue samples or molecular analysis, is the gold standard technique to confirm the diagnosis and direct therapy.5,17
Clinical experience has proven that antibiotic therapy in conjunction with surgical debridement, when applied in time, is the optimal management of nocardiosis, especially when the brain is involved. 18 Aspiration of abscesses greater than 25mm that are not minimized after four weeks of the aforementioned therapy, is recommended, regardless of the condition of the patient’s immune system.18,19 As far as antimicrobial agents are concerned, sulfonamides appear to be the touchstone of a successful treatment. Because they are able to cross the blood–brain barrier, along with the high antibiotic resistance profile of this pathogen, long term administration of sulfamethoxazole and trimethoprim parenterally is the treatment of choice, even if it is associated with a variety of side effects, such as nausea, hepatotoxicity and renal insufficiency, at times.20,21 In addition, Nocardia farcinica lies among the subspecies with the widest range of antibiotic resistance. Consequently, it can be easily assumed that the bacterium’s diverse resistance to antibiotics, accompanied by the difficulty in its identification, as well as the vague clinical presentation of the patient described here, led to a delay in the commencement of appropriate antibiotic treatment.
In conclusion, Nocardiosis is a rare entity that was thought to be a disseminated infectious disease mostly affecting the immunosuppressed population. Nowadays, it is accepted that the disease can also affect healthy individuals. Nocardia farcinica is reported to be among the subspecies that are most frequently responsible for the isolated pattern of nocardiosis, which mainly impairs the central nervous system. The combination of surgical debridement and long-term antibiotic treatment with trimethoprim and sulfamethoxazole is considered the most appropriate management. However, the nonspecific clinical manifestations, in addition to the difficulties in identifying the pathogen, as in our case, remain an obstacle for the prompt start of appropriate therapy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.