
Abstract
Objectives
This study aimed to analyse the correlation between depression, anxiety, and tinnitus handicap in patients with primary tinnitus.
Methods
A total of 102 patients (41 men, 61 women; mean age ± SD: 56.8 ± 11.6 years) were examined. They completed the Tinnitus Handicap Inventory (THI), Beck Depression Inventory (BDI), and Symptom-Checklist-90-Revised (SCL-90-R). Correlations were analysed using Pearson’s and Spearman’s tests. Logistic regression analysis was performed.
Results
The demographic data suggested a slight female predominance. The THI questionnaires indicated a worsening handicap in 73.5% of the patients, of which the ‘mild’ category was the most frequent, followed by severe handicaps. According to BDI, 69.6% of individuals fell in the normal category, with mild cases being the most frequent. Of the two psychiatric symptoms, depression (BDI) and tinnitus were strongly correlated (rho= 0.579, P < .0001*). The correlation was also significant according to the SCL-90-R depression questions (rho= 0.523, P < .0001*). Upon comparing the depressive scores and the THI subscores (i.e., functional, emotional, and catastrophic), each showed a significant correlation, with the strongest correlation with functional and emotional scores. The correlation with anxiety was slightly weaker (rho= 0.480, P < .0001*) but also significant. According to the Kaplan–Meier curves and logistic regression, the appearance of depressive symptoms did not significantly influence the appearance of a worsening handicap [P = .428; OR: 1.124 (95% CI: 0.842–1.501)]. However, a worsening handicap significantly influenced the appearance of depressive symptoms [P < .0001*; OR: 1.35 (95% CI: 1.34–4.86)], indicating that tinnitus has a more expressed effect on the appearance of depressive symptoms than reversed.
Conclusions
The correlation between tinnitus handicap and psychiatric comorbidities indicates the importance of psychological factors in tinnitus management. Tinnitus handicap has a more profound effect on depression scores. To avoid the occurrence of comorbidities, tinnitus handicaps must be reduced.
Introduction
Tinnitus is a sound that can be heard without the presence of an external sound stimulus. 1 Tinnitus is a common symptom, found in approximately 10–15% of the general population. 2 It can be mainly categorised into objective, subjective, primary, and secondary types. Moreover, it can be acute or chronic. In secondary cases, a well-defined otorhinolaryngological reason can be defined based on the background. Examples include external otitis or earwax, middle ear diseases (e.g., myoclonus, tonic tensor tympani syndrome, glomus tumours, or otitis media), inner ear disorders (e.g., Ménière’s disease), and benign tumours of the vestibulocochlear nerve (i.e., vestibular schwannoma). It can also manifest as a symptom of systemic disorders such as diabetes mellitus, dyslipidaemia, hypothyroidism, and vascular aetiology. Primary cases include idiopathic tinnitus, and this group can also be categorised as tinnitus related to sensorineural hearing loss. 3 However, the management of these primary cases remains complicated.
In unattended cases, tinnitus as a primary symptom can result in psychiatric comorbidities such as depression and anxiety. The aforementioned psychiatric comorbidities can be detected in 20% of the population with tinnitus. 4 Furthermore, in previous studies, anxiety and depression have been defined as predictive factors of chronic distressing tinnitus. 5 Depression can be a frequent comorbidity of tinnitus, clinical or subclinical. 6 Previous studies have also analysed the correlation between tinnitus distress and depressive symptoms, indicating a strong correlation. 7 Anxiety and depression are associated with lower quality of life. 8 This study aims to describe and examine the correlation between depression, anxiety, and tinnitus severity based on the Tinnitus Handicap Inventory (THI) questionnaire.
Patients and methods
In this study, we enrolled 102 patients (41 men, 61 women, mean ± SD age: 56.8 ± 11.6 years) with primary tinnitus. All patients underwent a detailed otorhinolaryngological examination to exclude any causes that resulted in secondary tinnitus (e.g., external otitis, earwax, middle ear diseases and Eustachian tube dysfunction). The hearing status of all patients was assessed using pure-tone audiometry, tinnitometry, tympanometry, and brainstem-evoked response audiometry to exclude retrocochlear lesions. Brain MRI was also performed for all subjects. This study was approved by the Semmelweis University Regional and Institutional Committee on Science and Research Ethics (SE RKEB – 203/2021).
Tinnitus handicap inventory questionnaire
THI is a self-administered questionnaire assessing three factors: emotional, functional, and catastrophic. Emotional factors (nine items) analyse the affective consequences of tinnitus, such as depression, anxiety, or frustration. The functional subscale (11 items) includes questions regarding the limitations in everyday life caused by tinnitus, including mental, social, and physical consequences (e.g., sleeping, loss of concentration and interference with a job). The catastrophic subscale (5 items) consists of questions regarding more severe reactions to tinnitus, such as the perception of having a terrible disease, lack of control, and inability to escape. A patient can answer each question with ‘yes’ (4 points), ‘sometimes’ (2 points), or ‘no’ (0 points). The total THI score was calculated by summarising the subscale scores. The interpretation of the total THI score is as follows: no handicap (0–16 points), ‘mild’ (18–36 points), ‘moderate’ (38–56 points), ‘severe’ (58–76 points), or ‘catastrophic’ handicap (78–100 points). 9 The THI questionnaire has previously been validated for the Hungarian population. 10
Beck depression inventory
The Beck Depression Inventory (BDI) is a self-administered questionnaire widely used in everyday clinical practice to detect depressive symptoms. The current study used the 13-item short form of the BDI questionnaire, which is a suitable tool for assessing depressive symptoms. The answer categories ranged from 0 (‘not at all’) to 3 (‘much’). The interpretation of the results is the following: not depressed (0–5 points), ‘mild’ (6–11 points),
Symptom-checklist-90-revised
The Symptom-Checklist-90-Revised (SCL-90-R) is a multidimensional questionnaire assessing psychiatric symptoms and psychopathologies, including 90 items. These questions deal with, for example, depressive symptoms, anxiety, hostility, and somatisation. The answer categories ranged from 0 (‘not at all’) to 4 (‘extremely’). In this study, patients completed all 90 questions in Hungarian. However, the present investigation analysed the results of questions dealing with depression (13 elements) and anxiety (10 elements).12,13
Statistical analysis
Data processing was performed using the IBM SPSS Statistics for Windows, version 24 (IBM Corp., Armonk, N.Y., USA). Spearman’s and Pearson’s correlation tests were used to detect any correlations between the questionnaire scores. A P-value below .01 was considered a statistically significant difference. Furthermore, Kaplan–Meier curves were drawn to analyse the effects of the category measured by the questionnaires on the other, and logistic regression was used to detect a significant difference. The significance level was set as P < .05 in the case of this method.
Results
Patients’ basic demographic data and summarisation of the results of the THI and BDI questionnaires.
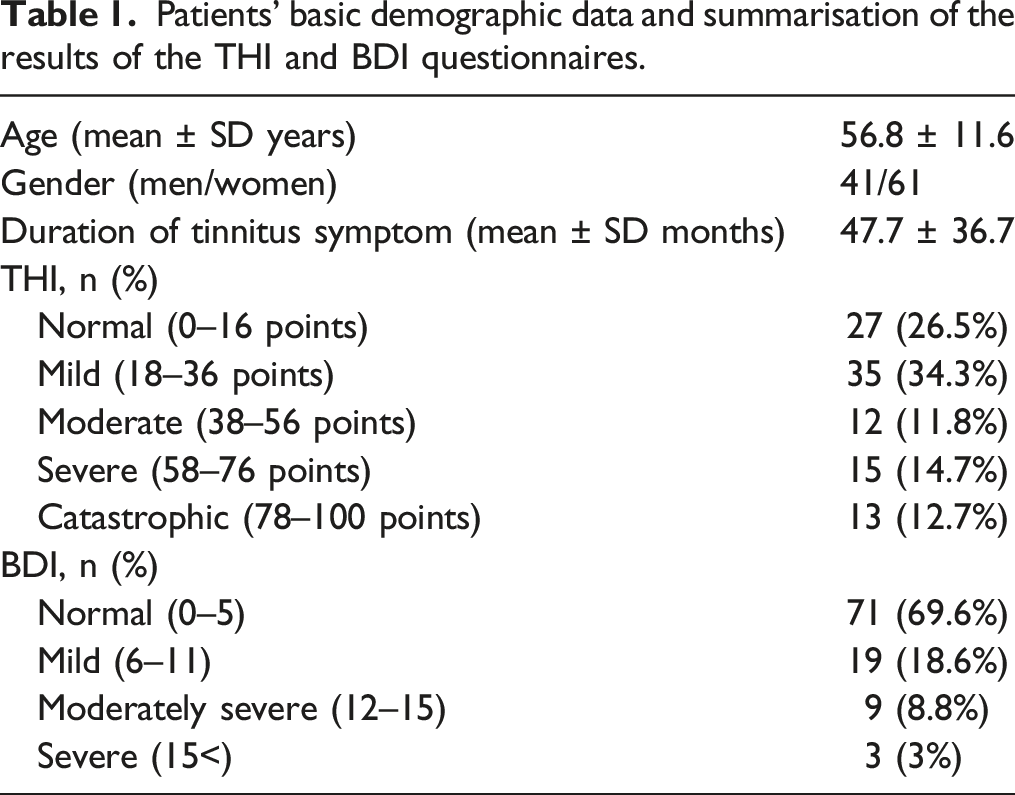
A slight female predominance was observed in the basic demographic data, with a mean age of approximately 55 years. This indicates that a higher proportion of middle-aged women were examined. As Table 1 illustrates, in the case of the THI questionnaires, only approximately 26% of the patients reported a normal tinnitus handicap (i.e., < 18 total points). Consequently, around three-quarters of the participants indicated a worsening handicap, indicating a significant tinnitus ratio affecting their day-to-day functioning. Furthermore, 'mild' handicap was the most common category, followed by 'severe' and 'catastrophic'. Therefore, a mild effect, although significant, is suspected in most cases. In contrast, depressive symptoms were detected in 30% of the patients; therefore, the appearance of depressive symptoms was slightly lower. The most frequent category, in this case, was 'mild', agreeing with the results of the THI questionnaires.
Correlation between total THI and its subscores and the results of BDI and SCL-90-R. Spearman’s and Pearson’s tests were used to detect a possible correlation between the results of the questionnaires. The rho-values show the correlation coefficients, indicating a perfect correlation with a rho-value of 1. A P-value below 0.01 was defined as a significant correlation indicated by the * sign.
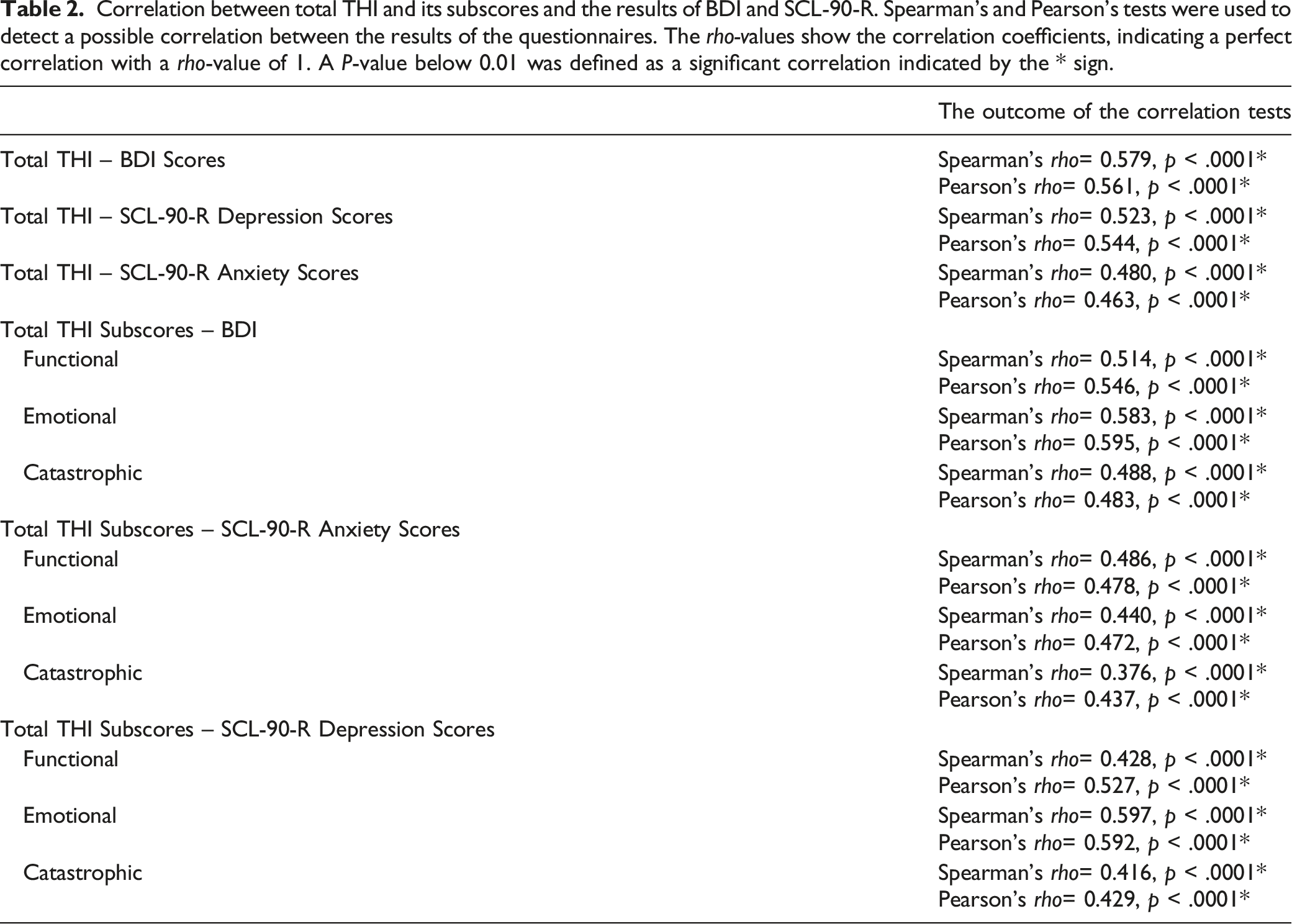
As shown in Table 2, comparing THI and depression scores revealed the strongest statistically significant correlation (rho= 0.579, P < .0001* and rho= 0.561, P < .0001*, respectively). Upon comparing the THI subscores, each item was significantly correlated with the BDI scores, with the strongest correlation in the case of functional and emotional scores. This result was also confirmed by the SCL-90-R depression scores, which indicated a significant correlation with THI (rho= 0.523, P < .0001* and rho= 0.544, P < .0001*, respectively) and its subscores, with a stronger correlation in the case of functional and emotional questions. Based on these findings, it can be stated that depressive symptoms are primarily influenced by functional and emotional aspects of the tinnitus handicap. A slight but significant correlation was observed between anxiety and total THI scores (rho= 0.480, P < .0001* and rho= 0.463, P < .0001*, respectively). These results indicate the most significant correlation between tinnitus handicap and depressive symptoms. Furthermore, the functional and emotional aspects showed the most significant influence on depression and anxiety, respectively.
Another question was whether the correlation between tinnitus handicap and psychiatric symptoms suggests a more significant effect of tinnitus on psychiatric symptoms or the contrary. Kaplan–Meier curves were plotted and analysed to answer these questions.
The data in Figure 1 indicates no apparent difference between the two curves (i.e., probability of a worsened handicap with and without depressive symptoms), indicating no significant differences between the total THI categories with and without depressive symptoms. Statistical analysis also strengthened this result, as logistic regression did not find a significant difference between the two groups [P = .428; OR: 1.124 (95% CI: 0.842–1.501)], i.e., the appearance of a worsening handicap with and without depressive symptoms. Therefore, it can be stated that the results of BDI and the appearance of depressive symptoms did not significantly influence tinnitus handicap. This result can also be interpreted as, according to THI, patients with depressive symptoms do not necessarily report worse tinnitus handicap. Kaplan–Meier curve assessing the results of the BDI and THI questionnaires. Blue curve: no depression based on the categories of the BDI; green curve: the appearance of depressive symptoms (mild, moderately severe, or severe category). The appearance of depressive symptoms was the influential factor in the THI results. In SPSS, the event was defined as the appearance of a worsening tinnitus handicap (including a mild, moderate, severe, or catastrophic handicap). The vertical axis (Y) represents the probability of the defined event (i.e., worsening tinnitus handicap): at 1.0, the probability of a normal handicap is 100%. When the curve drops, a worsened handicap is more frequent.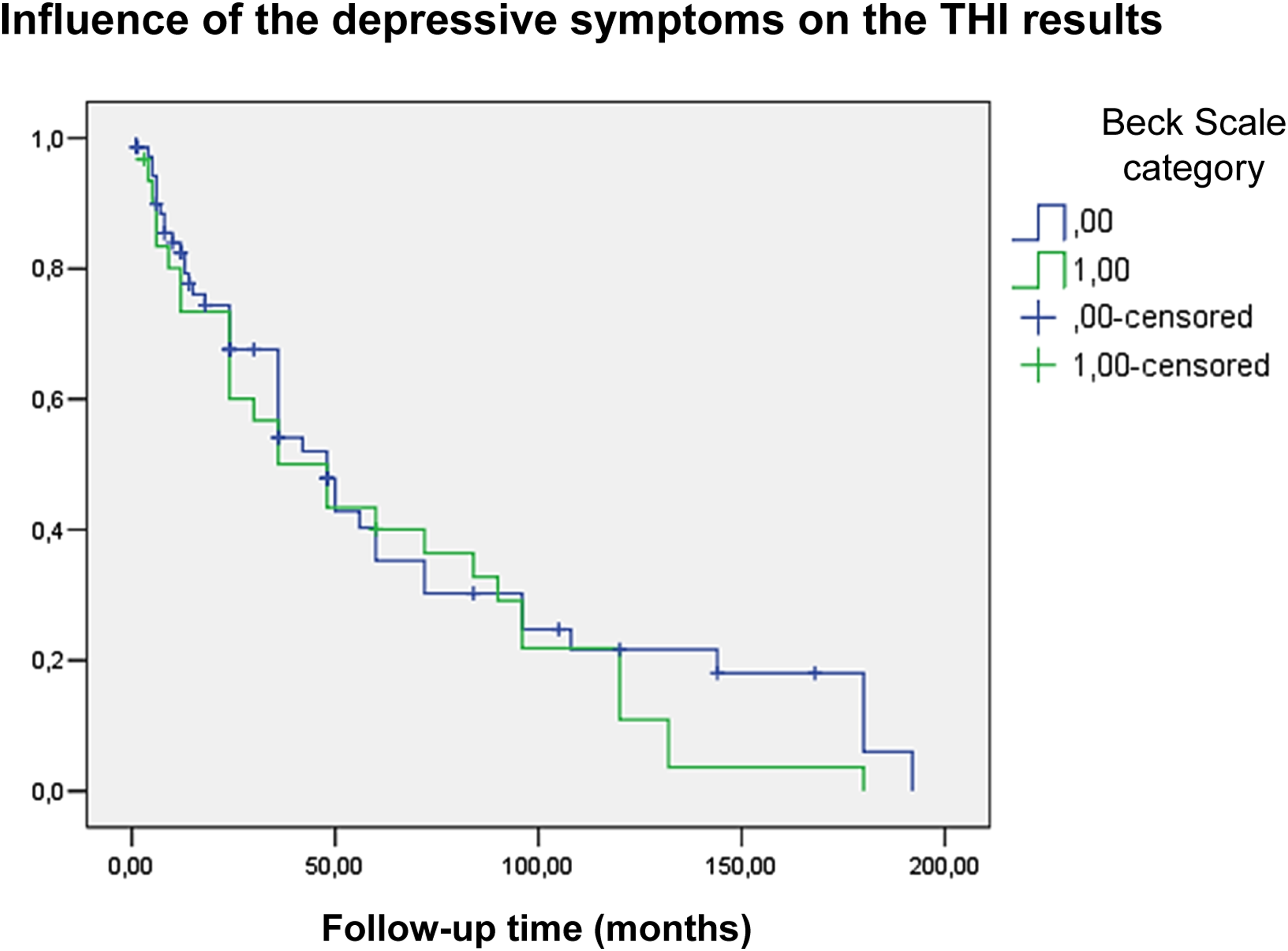
The Kaplan–Meier curve categories were changed, and the THI category was defined as the influential factor for analysing the influence of tinnitus on depressive symptoms. The results are shown in Figure 2. The differences between the appearance of depressive symptoms in participants with a worsened or normal tinnitus handicap could be analysed. Kaplan–Meier curve on the results of the BDI and THI questionnaires. Blue curve: normal tinnitus handicap; green curve: the appearance of a worsening handicap (mild, moderate, severe, or catastrophic handicap). In this case, a worsened tinnitus handicap influenced the BDI results.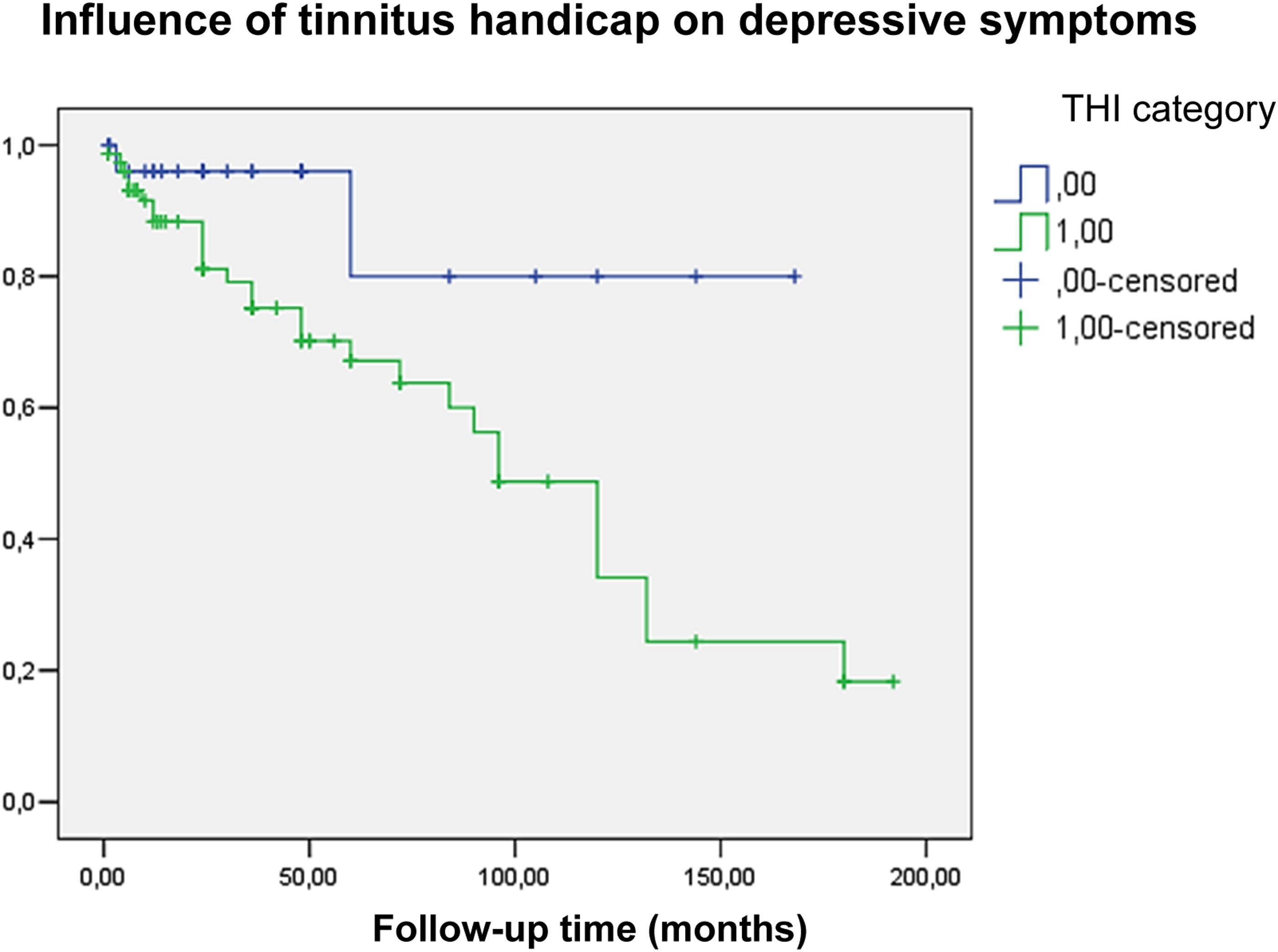
As illustrated in Figure 2, in this case, there was an apparent difference between the two groups (i.e., the probability of the appearance of depressive symptoms with and without worsening of the tinnitus handicap), indicating a more frequent appearance of depressive symptoms in the case of worsening tinnitus handicap than in participants with normal handicaps. Upon performing a statistical analysis using logistic regression, a significant difference was detected [P < .0001*; OR: 1.35 (95% CI: 1.34–4.86)], suggesting a higher probability of depressive symptoms occurring in the case of worsening tinnitus. The results of the two Kaplan–Meier analyses, which show a correlation between depressive symptoms and tinnitus handicap, can be explained by worsening handicap results in the appearance of depressive symptoms.
Discussion
In this study, we investigated many patients with primary tinnitus. According to the demographic data, these patients were predominantly women, with a mean age of approximately 55 years. Our results are in good agreement with previous studies. 14 According to the results of the THI questionnaires, only 26% of our patients reported a normal tinnitus handicap; in most cases, the patients experienced a worsened tinnitus handicap, of which the most frequent category was ‘mild’. Based on the BDI results, only 30% of the participants reported depressive symptoms, although a significant correlation was detected between depressive symptoms and the severity of tinnitus handicaps. This finding is analogous to the results of previous studies. For example, in terms of THI grades, the same distribution was observed in a previous study in men and women. 15
A study in Japan reported that tinnitus severity was mainly affected by depressive symptoms, followed by anxiety disorders, and was much less affected by high-frequency hearing loss. 16 The results of correlation analysis confirmed this finding, where depressive symptoms, based on the BDI and SCL-90-R questionnaires, were strongly correlated with the total THI and its subscores. A study that included veterans reported that most patients with tinnitus also reported anxiety and depression. Furthermore, patients with psychiatric comorbidities have a more severe type of tinnitus. 17 Another study also found a strong relationship between tinnitus, anxiety, and depression, as well as shorter sleep duration and missed extended workdays. In conclusion, these comorbidities have also been considered for treating chronic and bothersome tinnitus. 18 In one study, anxiety was the most important predictive factor for tinnitus, followed by depression, although only neuroticism was correlated with THI scores in personality dimensions. Their conclusions suggest that tinnitus management should also consider psychological factors. 19 An important conclusion of a previous study is that the authors defined the critical role of depressive symptoms in chronic tinnitus, explained by a ‘vicious cycle’. They found that depressive symptoms can facilitate tinnitus as a chronic symptom but can also be defined as a maintenance factor. In their opinion, even though anxiety was a co-mediator of the cycle and therefore correlated with THI, this can be explained by the presence of depressive symptoms in the analysis. 20 This is consistent with the results of the present study, wherein we observed a slight correlation between anxiety and THI and its subscores. The THI categories were similar to those in the current investigation, indicating ‘mild’ as the most frequent category. Therefore, in our opinion, the results of the two investigations are comparable.
One study analysed the effects of tinnitus on brain structures using T1-weighted structural MRI scans. As an essential finding, the reduction in the parahippocampal grey matter was predicted mainly by tinnitus and less by psychometric results. A reduction in the parahippocampal grey matter was also observed on the left hippocampus when the results of patients with low-distress tinnitus were compared with those of control patients. This study is clinically important as it shows that patients with tinnitus can suffer from psychological distress at nearly the same level as psychiatric patients. These results suggest that patients with tinnitus are more distressed than healthy controls, even if they do not meet the clinical diagnostic criteria. 21 These facts highlight the results of the present study. According to the BDI categories, most patients were not clinically diagnosed with depression, although a significant correlation was observed between the depression scores and THI. This result is consistent with the aforementioned results, i.e., even in the case of subclinical depression, the severity of tinnitus can be influenced and should be considered. Regarding the possible neuroanatomical background, another investigation concluded that emotional disorders (e.g., anxiety and depression) could be explained by the correlation between non-auditory structures (e.g., locus coeruleus, raphe nuclei and reticular formation) and the dorsal cochlear nucleus. 22 In the present investigation, upon comparing the correlation of THI with depression and anxiety scores, the strongest correlation was observed in the case of the emotional aspects of THI. This result also highlights the effects of emotional functioning on the appearance of psychiatric symptoms.
The correlation between tinnitus handicap and psychiatric comorbidities indicates the importance of psychological factors in managing tinnitus. According to the statistical analysis, tinnitus handicaps had a more pronounced effect on depression scores. Therefore, to avoid the occurrence of comorbidities, tinnitus handicap must be reduced.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
All procedures performed in the study involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The study was approved by the Semmelweis University Regional and Institutional Committee of Science and Research Ethics: SE RKEB – 203/2021.
Consent to participate
All participants obtained written informed consent. Informed consent was obtained from all individual participants included in the study for publication.
Data availability statement
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.