
Abstract

Significance Statement
This report demonstrates a chronically infected tongue and hyoid suspension system resulting in facial cellulitis and floor-of-mouth swelling which concerned the referring provider for malignancy. Excision of the hardware resolved the infection, and pathology demonstrated the rare finding of a metaplastic synovial cyst. While more acute infections of tongue and hyoid suspension systems have been reported, this is the first case discussing a long-delayed infection resolving with removal.
Case Report
A 33-year-old male with a history of OSA presented to our otolaryngology clinic after primary care referral for a three-month history of a floor-of-mouth and tongue-base mass with worsening left neck swelling. He was seen previously by dermatology for submental pink papules and pustules (Figure 1) and was treated for suspected folliculitis with topical and oral antibiotics. Despite antibiotic therapy, the floor-of-mouth mass increased in size. Of note, he had also undergone hyoid myotomy with bone-anchored suspension to the mandible (AirLift; Siesta Medical, Inc., Los Gatos, California), and tongue base suspension suture, both performed eight years ago at another facility. The preoperative clinical exam demonstrates findings of chin cellulitis and serous drainage (A) and normal mucosal appearance along left floor of mouth (B). Intraoperatively, an elliptical skin excision (C) and removal of hyoid suspension sutures (D) is performed.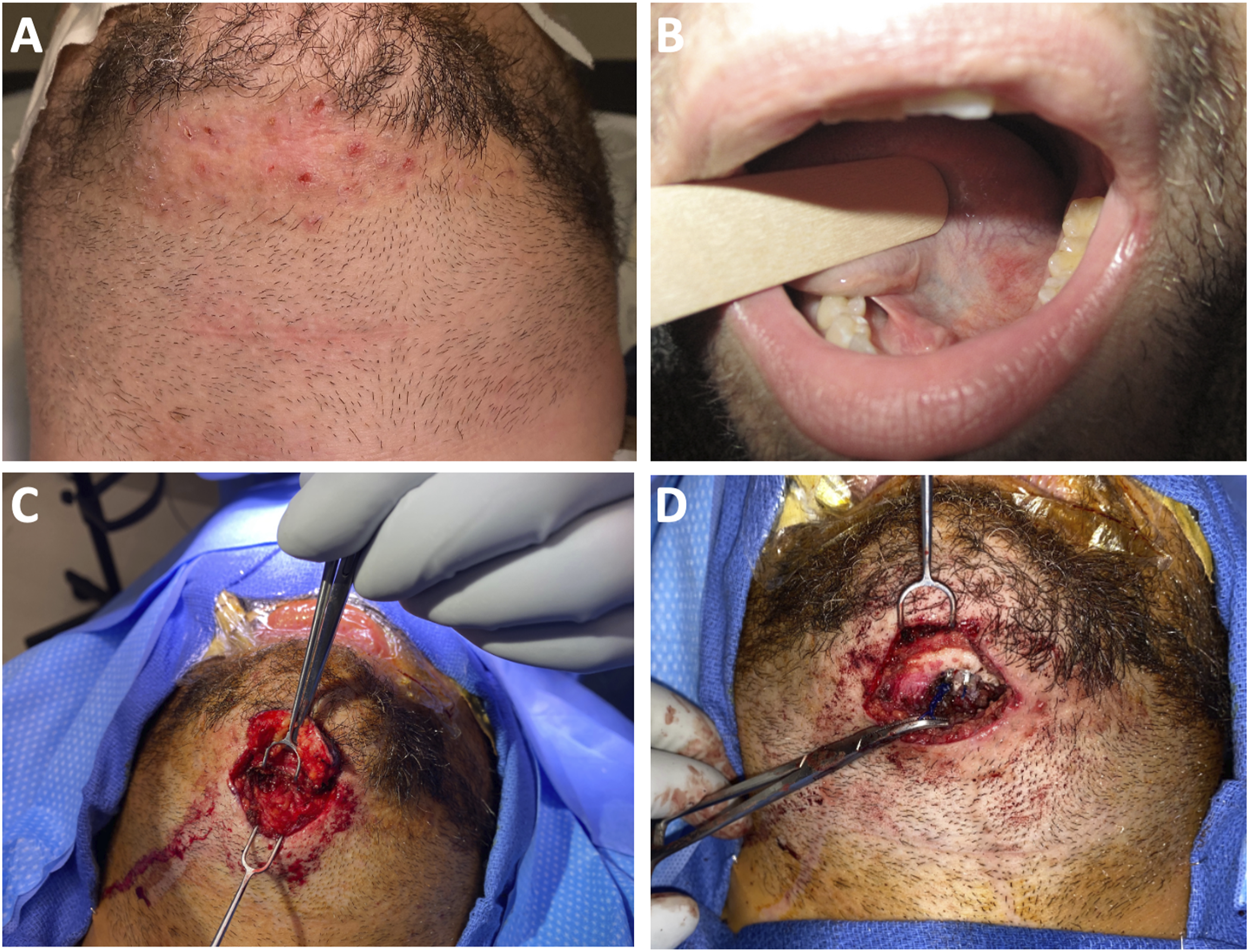
Computed Tomography (CT) scan demonstrated an enhancing submucosal process in the tongue. Physical exam demonstrated a firm, submucosal sublingual mass. Flexible laryngoscopy was normal. Magnetic Resonance Imaging (MRI) (Figure 2) demonstrated a nodular, contrast-enhancing dorsal tongue base mass measuring 2.5 × 1.2 × 1.9 centimeters (cm) with enhancement along the left anterior aspect of the base of the tongue measuring 1.9 × 1.4 × 1.7 cm. Due to concern for infected surgical hardware and inadequate prior antibiotic treatment, he was started on amoxicillin/clavulanate for two weeks with subsequent marked decrease in the size of the mass. Physical exam showed submental cellulitis with a small subcutaneous nodule and a non-tender, mobile submucosal nodularity along the left floor of the mouth, measuring approximately 7–8 millimeters (mm). The preoperative CT and MRI imaging of the tongue base demonstrates inflammation mimicking malignancy. An axial view shows tongue base inflammation with CT (A) and MRI T1 with gadolinium contrast (B). A coronal CT view shows the tract of the tongue base suspension sutures with a surrounding granuloma (C), and a sagittal MRI view shows the complete tract of the tongue base suspension suture (D).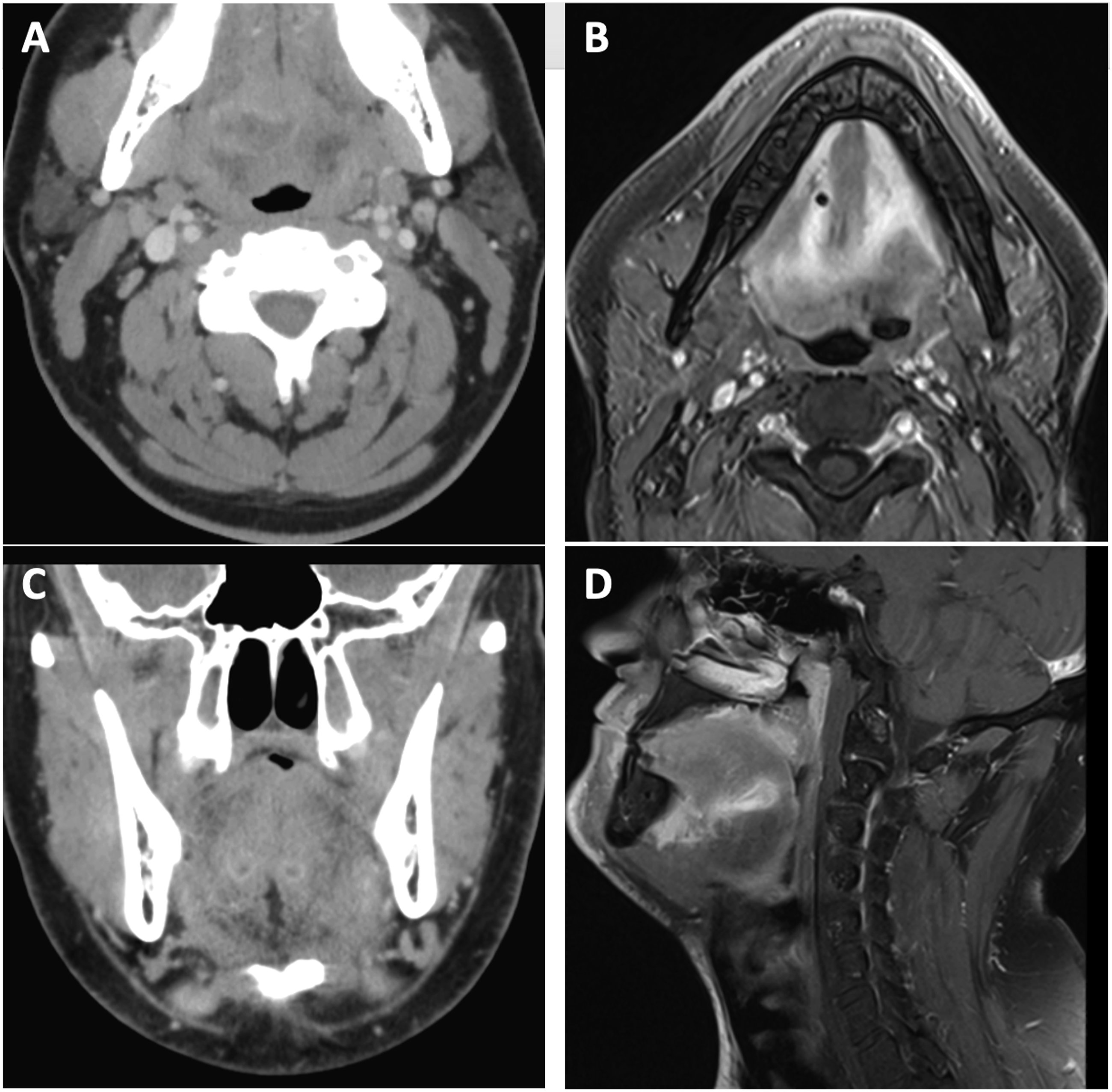
The patient was scheduled for excision of infected hardware two months later. An elliptical incision was created surrounding the suspected infected fistula tract and carried deep to the anterior bellies of the digastric. Polypropylene sutures (Prolene; Ethicon, Inc.), suspected to be a source for the fistula tract, were identified tracking from the hyoid to the inferior border of the mandible. These were removed from around the hyoid and followed to the anchor points in the mandibular periosteum. Two bone-anchored screws were not released to prevent pathologic fractures. Instead, a diamond drill was used to bur these down until the anchored sutures released. The border of the mandible and remnant anchors were smoothed down. The wound was irrigated and debrided then closed in two layers. Biopsy of the anterior neck skin and soft tissue demonstrated chronic inflammation, focal foreign body giant cell reaction, and metaplastic synovial cyst (Figure 3). Pathology slides demonstrate chronic inflammation, focal foreign body giant cell reaction and a metaplastic synovial cyst. A low-power view of skin excision shows a deep dermal cyst with projections into the luminal space (A). A high-power reveals villus-like projection with fibrinous cyst lining (B). Adjacent chronic inflammation and giant cell reaction is noted (C).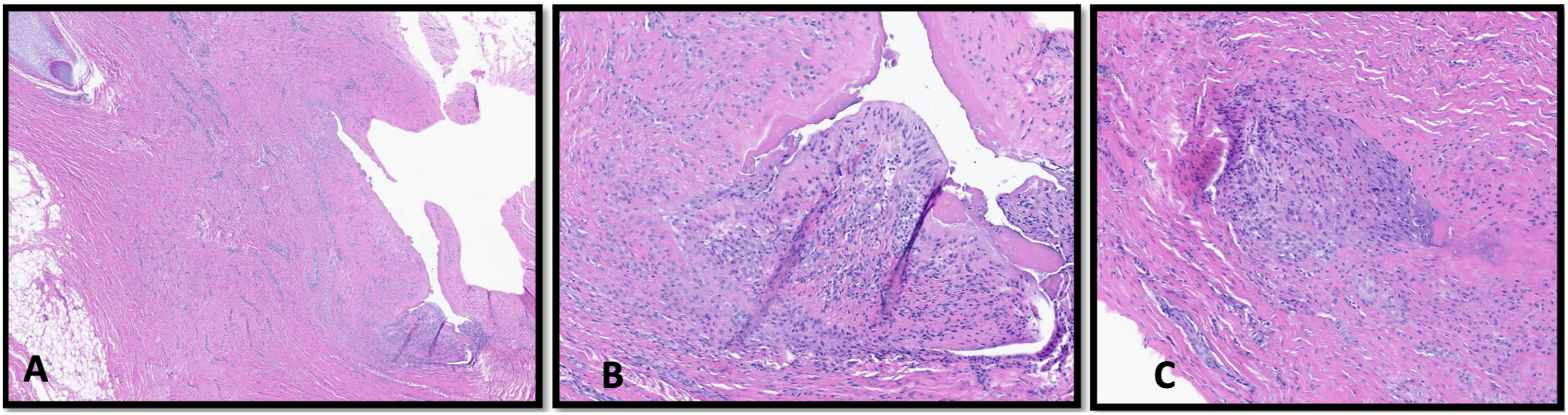
On the clinic visit three weeks after surgery, he reported wound dehiscence of the anterior neck with yellow drainage. Exam disclosed a 3.5 cm anterior neck wound dehiscence, with thin yellow drainage and no evidence of abscess. The wound was debrided and closed, and he was started on a 10-day course of amoxicillin. Two weeks later, the incision was noted to have healed well. He returned closer to home for follow-up.
Discussion
Both hyoid suspension and tongue base suspension procedures are relatively safe and effective treatments of OSA. 1 While isolated tongue suspension may improve AHI by 38%, the rate of complications, including suture infection and extrusion, may range from 12.5–18%.1-3 These risks must be thoroughly considered during surgical decision-making. In this case, the hardware and suture implant developed an infection and granuloma. Foreign body granulomas may appear months to years after surgery and can mimic tumors, abscesses, and other masses. 4 In this case, the patient was referred to the otolaryngology clinic for concern of a large volume tongue malignancy, which was secondary to tongue base and submandibular inflammation.
Interestingly, although hyoid suspension systems have been associated with abscess and fistula formation in the acute setting, 5 significant long-term complications, including infection, floor-of-mouth edema, or foreign body reaction years after tongue base suspension suture placement have not been reported. 6 In this case, after appropriate antibiotic treatment and suture removal, this inflammation resolved.
An additional unique finding of this case was the development of a metaplastic synovial cyst, which can be associated with trauma and tissue fragility. 7 Interestingly, his physical exam was not specific for the presence of a cyst, and a cyst was not visualized intraoperatively. However, an elliptical tract of skin was excised overlying the area of cellulitis tracking to the deeper soft tissue adjacent to the suspension sutures.
Footnotes
Acknowledgments
We would like to acknowledge the West Virginia University Department of Pathology for their contribution and annotation of pathologic images.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
Patient provided informed consent for journal reproduction of clinical information, imaging, and photographs.