
Abstract
Objective
Dermoid cysts (DCs) are congenital, slowly growing, and may cause nervous system symptoms. Related literature is limited and mainly includes case reports. We report a case series of DCs originating from the middle cranial fossa floor (MCFF) and investigate their demographic information, clinical characteristics, imaging findings, surgical procedures, and prognostic outcomes.
Methods
We reviewed the patients with DCs arising from the MCFF undergoing endoscopic endonasal surgery (EES) in our center between 2012 and 2022.
Results
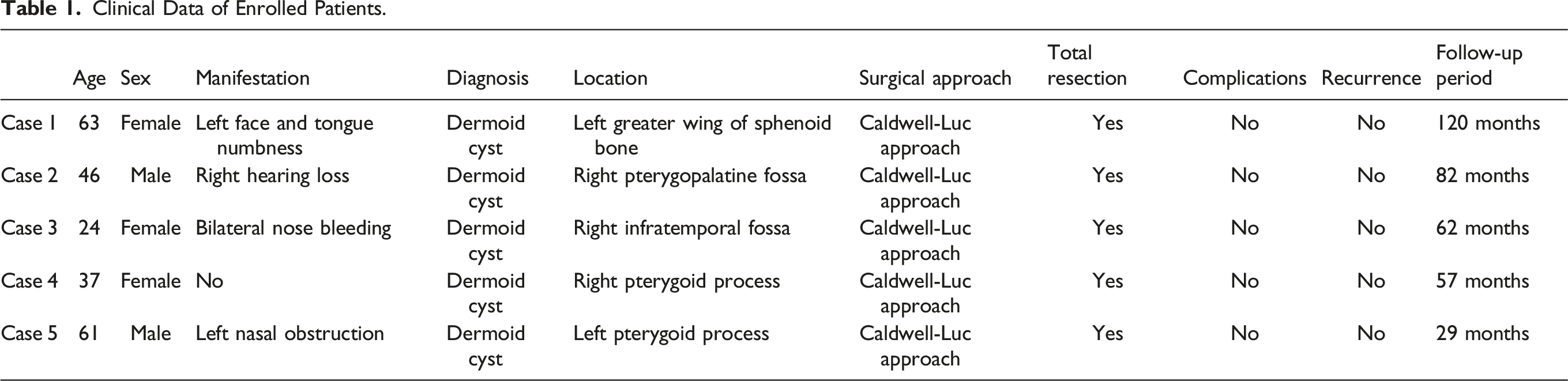
A total of 5 patients with DCs were enrolled (2 males and 3 females), with a mean age of 46.2 years at the onset. All DCs originated from the MCFF with 1 case involving the middle cranial fossa bone and another 1 case affecting the dura mater. One (20.0%) patient had neurological involvement. After admission, all patients received EES with a total resection rate of 100.0% (5 of 5). After a median follow-up of 73.2 months, all patients achieved complete clinical and radiological improvements. No surgical-related complications or relapses were observed during the long-term follow-up.
Conclusion
Endoscopic endonasal surgery is considered a safe and effective approach for the treatment of DCs in the MCFF. A larger sample size and longer follow-up time are needed.
Introduction
Dermoid cysts (DCs) are rare congenital tumors that account for only 0.04–0.7% of all intracranial tumors and are most common in patients aged 20–36 years. 1 -4 They are believed to arise due to ectopic inclusion of epithelial cells in the course of neural tube closure during embryologic development 3 and contain dermal and epidermal elements including sebum, hair, and keratin. 5 These tumors have rarely been reported to arise from the middle cranial fossa (MCF) but usually originate from the petrous apex or cavernous sinus and may involve the MCF. 5,6 Common clinical presentations often depend on the location of the tumor 7 -9 and whether it is ruptured, 10 and can present with headaches, seizures, chemical meningitis, and visual disturbances, and olfactory hallucinations. Computerized tomography (CT) and magnetic resonance imaging (MRI) features are sufficient for accurate diagnosis, 11 yet this confirmation remains dependent on intraoperative histological examination. DCs are basically surgically treated diseases, and traditional approaches for DCs are multiple open approaches. Instead of such invasive techniques, some surgeons convert to resect such lesions via endoscopic endonasal surgery (EES). 12,13 If possible, all lesions should be excised to avoid tumor recurrence. However, subtotal resection is considered acceptable because of the strong adhesion of the capsule to the surrounding nerve and vascular structures. 14 Growing evidence supports the advantage of multiple approaches in treating intracranial DCs, but only case studies have been performed. Thus, more information on clinical characteristics, radiographic findings, surgical procedures, and prognostic outcomes should be identified and summarized. In this study, we collected five case series of DCs arising from the middle cranial fossa floor (MCFF) treated with EES in our institution and shared our preliminary experiences and evaluated the feasibility of endoscopic endonasal surgery treatment.
Patients and methods
Study design
We retrospectively analyzed the clinical data of DCs originating from the middle cranial fossa floor (MCFF) treated with endoscopic endonasal surgery (EES) in our center from 2012 to 2022. The diagnosis of the patient population was made by an otolaryngologist and a pathologist on the basis of neurological symptoms, endoscopic examinations, radiological findings, and pathological outcomes. Clinical data including demographic information, clinical features, imaging and pathological findings, treatment, and prognostic outcomes were retrospectively collected by an independent resident doctor.
The clinical response and safety of EES treatment were evaluated. Complete response (CR) was defined by the complete disappearance of neurological symptoms and other disease-related symptoms, and by the complete improvement of radiological abnormalities related to DCs three months after EES treatment. Partial response (PR) was defined by the partial disappearance of neurological symptoms and other disease-related symptoms and by the partial improvement of radiological abonormalities three months after EES treatment. The main outcome measures were resection degree, postoperative complications, and recurrence rate. This study was approved by the Institutional Review Board of Eye & ENT Hospital of Fudan University. All participants signed informed consent forms.
Case presentations
Case 1
A 63-year-old female presented with numbness in the left face and tongue without an obvious trigger six months ago. After drug treatment in another hospital, there was no improvement. The patient was admitted and underwent CT, which revealed a cartilaginous soft tissue mass on the left MCFF (Figures 1A and 1B). The patient’s MRI demonstrated an intracranial and extracranial neurogenic tumor with cystic degeneration in the large wing of the left sphenoid bone (Figures 1C and 1D). Thus, the patient subsequently underwent endoscopic resection of the mass in the left MCF after the completion of preoperative examination and anesthetic evaluation. During the operation, the first step was to remove the left two-thirds of the middle turbinate and ipsilateral uncinate processes. The next step was to successively enlarge the ostium of the left maxillary sinus, ethmoid sinus, and sphenoid sinus. Then, the anterior wall of the sphenoid sinus was resected, and the bone of the bottom wall of the sphenoid sinus and the pterygoid root was removed. Specifically, the bone of the anterior wall of the maxillary sinus was removed via the left labigingival sulcus incision for better exposure. The lesion was located in the left skull base and posterolateral pterygoid process and extended to the MCF. The lumen of the lesion was fully exposed and enlarged, and a substantial amount of caseous outflow was observed. A bone defect in the middle cranial fossa was found, while the dura mater was intact, and the internal carotid artery was well protected. There were no significant surgery-related complications. Intravenous antibiotics were given postoperatively. On the fourth day of admission, the patient was discharged without any discomfort. The patient recovered well and the disease-related symptoms completely disappeared at the 88-month follow-up. Preoperative computed tomography and magnetic resonance imaging. (A and B) Computed tomography scanning revealed a soft tissue mass at the bottom of the left middle cranial fossa with uneven density. The mass was dilated and partially smooth, involving the left cavernous sinus, the bottom of the temporal lobe, the lateral wall of the sphenoid sinus, the parapharyngeal wall, the infraorbital fissure, the pterygopalatine fossa, and the infratemporal fossa. (C and D) Magnetic resonance imaging scanning showed a slightly irregular oval mass in the left pterygopalatine fossa, protruding outward into the infratemporal fossa and inward into the sphenoid sinus. T2WI showed uniform hyperintensity without enhancement.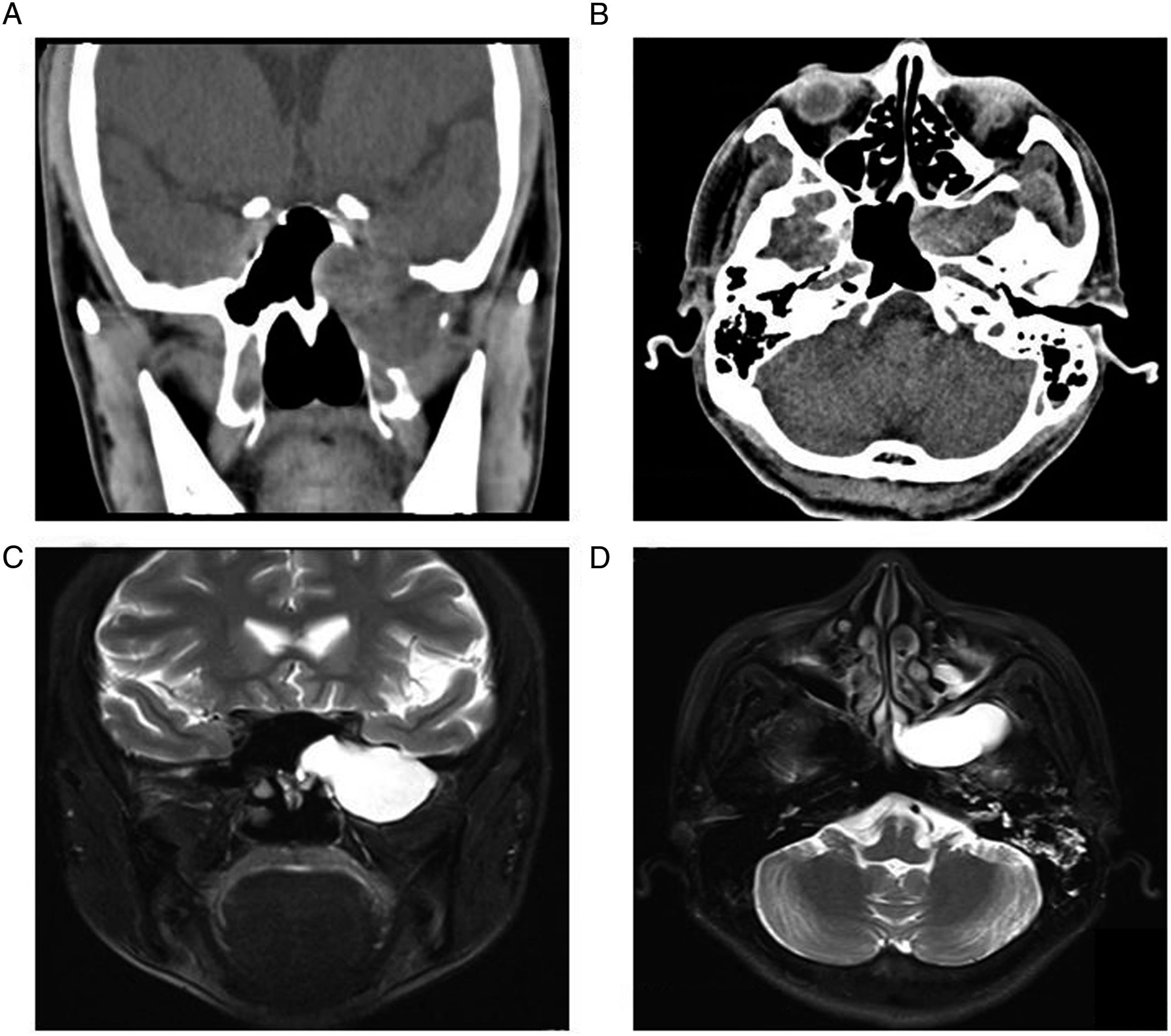
Case 2
A 46-year-old male reported persistent occlusion of the right ear with low frequency hearing loss. He claimed to have received medical treatment (details are unknown) in another hospital and achieved slight improvement. Preoperative CT examination showed an enlarged soft tissue mass in the right pterygopalatine fossa, involving the ipsilateral pterygoid muscle, sphenoid wing, and infraorbital fissure. Neurogenic tumors were considered first (Figure 2A and 2B). Briefly, surgical intervention exposing the posterior wall of the maxillary sinus revealed the lesion in the pterygopalatine fossa and infratemporal fossa. The cyst cavity compressed the eustachian tube, pterygoid nerve, and paraclival internal carotid artery. Eventually, the cyst cavity was enlarged and internal fluid was removed. The patient reported that the sense of ear occlusion disappeared, their hearing was significantly improved after the operation, and there was no recurrence during the 82-month follow-up. Preoperative computed tomography. Computed tomography revealed a round dilated soft tissue mass in the right sphenoid sinus floor and pterygopalatine fossa with clear boundaries, slightly involving the infratemporal fossa, infraorbital fissure, and anterior segment of the eustachopharyngeal tube with low density and no enhancement.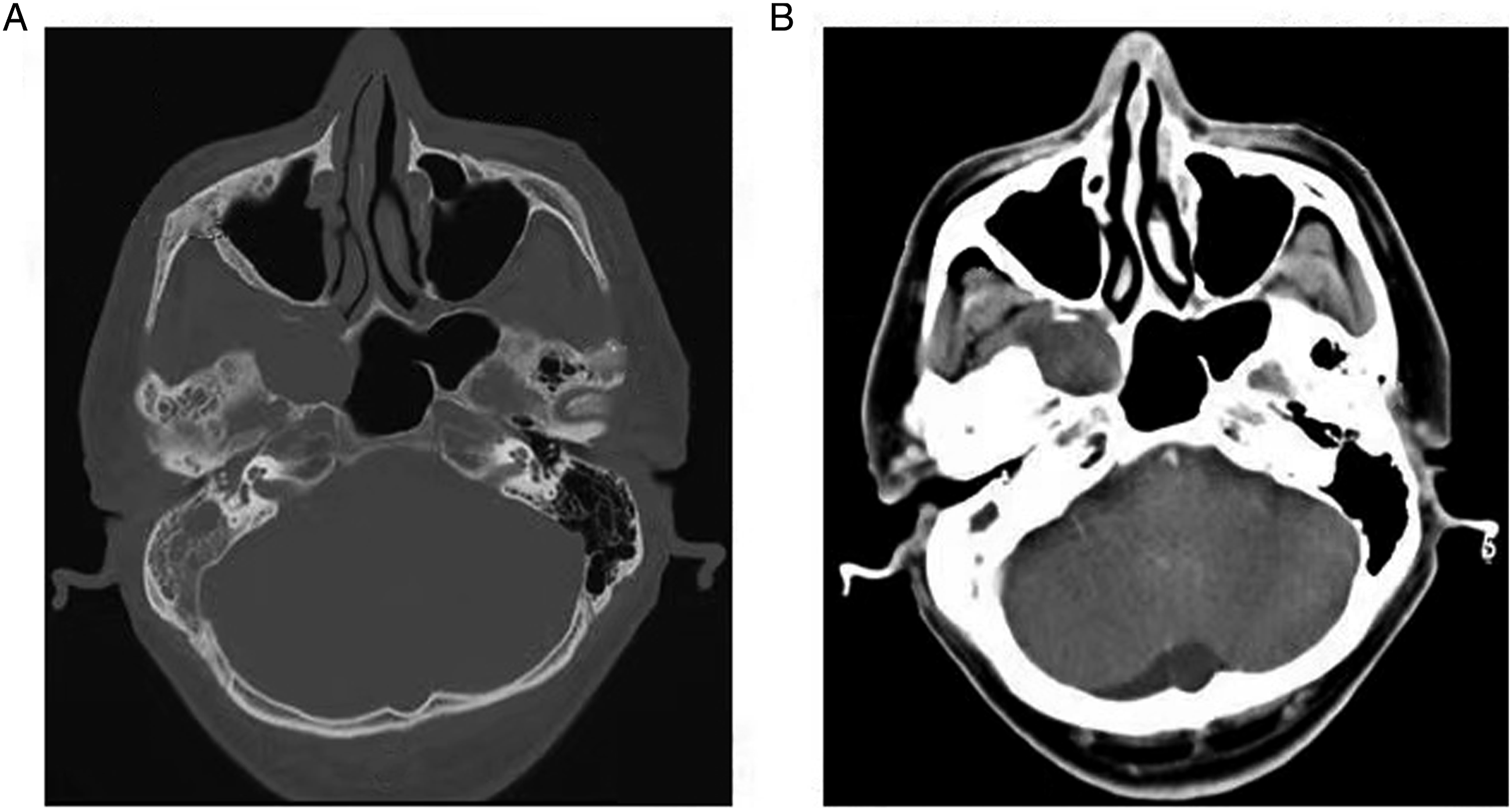
Case 3
A 24-year-old female was taken to the local hospital for CT examination because of unknown nose bleeding. Imaging results revealed an abnormal signal focus adjacent to the right pterygopalatine fossa. Several months ago, the patient had experienced a twitch sensation on the lateral face of the right inferior orbital margin without facial numbness. For further diagnosis and treatment, plain CT and enhanced MRI scanning were performed in our hospital and revealed a large circular mass in the middle of the right skull base (Figures 3A-E). Consequently, infratemporal fossa lesion resection was performed. First, part of the anterior middle turbinate and the uncinate process was removed, and then the ostium of the maxillary sinus, ethmoid sinus, and sphenoid sinus were routinely enlarged. The sphenopalatine foramen was exposed to block the sphenopalatine artery and its branches, and the pterygoid nerve was also removed. Then, the anterior and posterior walls of the maxillary sinus were removed through the labigingival sulcus approach and the maxillary nerve was cut off. The cyst-like lesion was located in the infratemporal fossa, and the bean curd residue secretions were observed to spill out after exposing the pterygopalatine fossa and infratemporal fossa. The anterior skull base was well protected and no leakage of cerebrospinal fluid was observed. The patient continued to do well 62 months after surgery. Preoperative computed tomography and magnetic resonance imaging. (A, B and C) Sagittal, coronal, and horizontal enhanced computed tomography showed an expanded soft tissue mass in the right middle skull base and infratemporal fossa with low density and smooth edges. (D and E) Magnetic resonance imaging showed oval abnormal signal foci in the right middle skull base foramen ovale and infratemporal fossa with obvious hyperintensity on T2 sequences.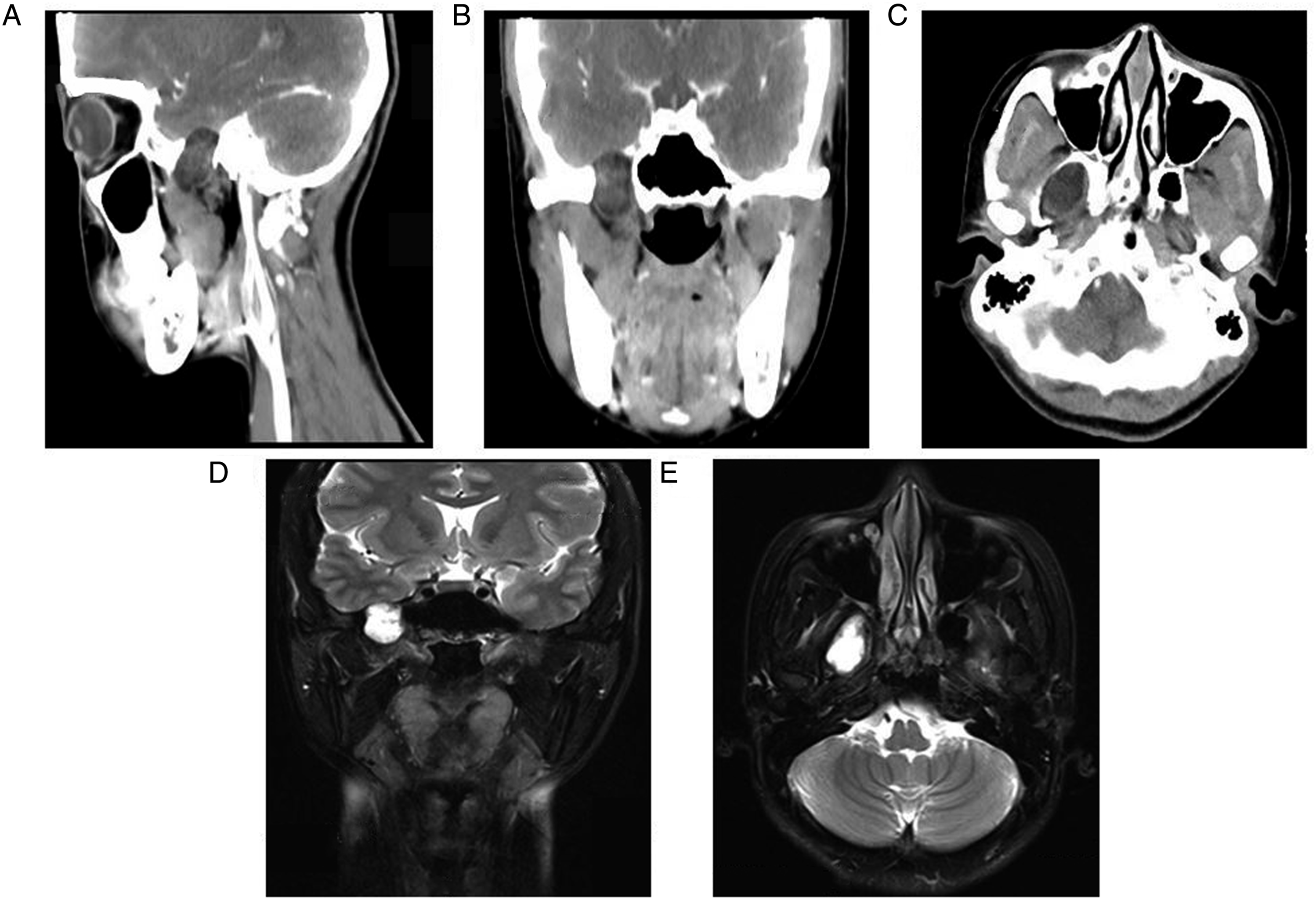
Case 4
A 37-year-old patient developed a right middle skull base mass with pharyngeal discomfort during physical examination three weeks ago. CT examination showed a 2 cm * 3.5 cm oval mass in the right middle skull base (not shown). Intraoperative surgery found that pterygopalatine fossa was exposed after removing the posterior wall of the maxillary sinus and then the mass was seen in the middle skull base after removing the process of the sphenoid bone. The capsule of the mass was dissected and was filled with yellow granules. Multiple imaging examinations after the operation did not find any signs of tumor recurrence (Figure 4A-D). Postoperative magnetic resonance imaging scan. Coronal (A and C) and axial (B and D) magnetic resonance imaging T2 sequences show complete dermoid cyst removal in the right middle skull base without any recurrence at the four-month and two-years follow-ups, respectively.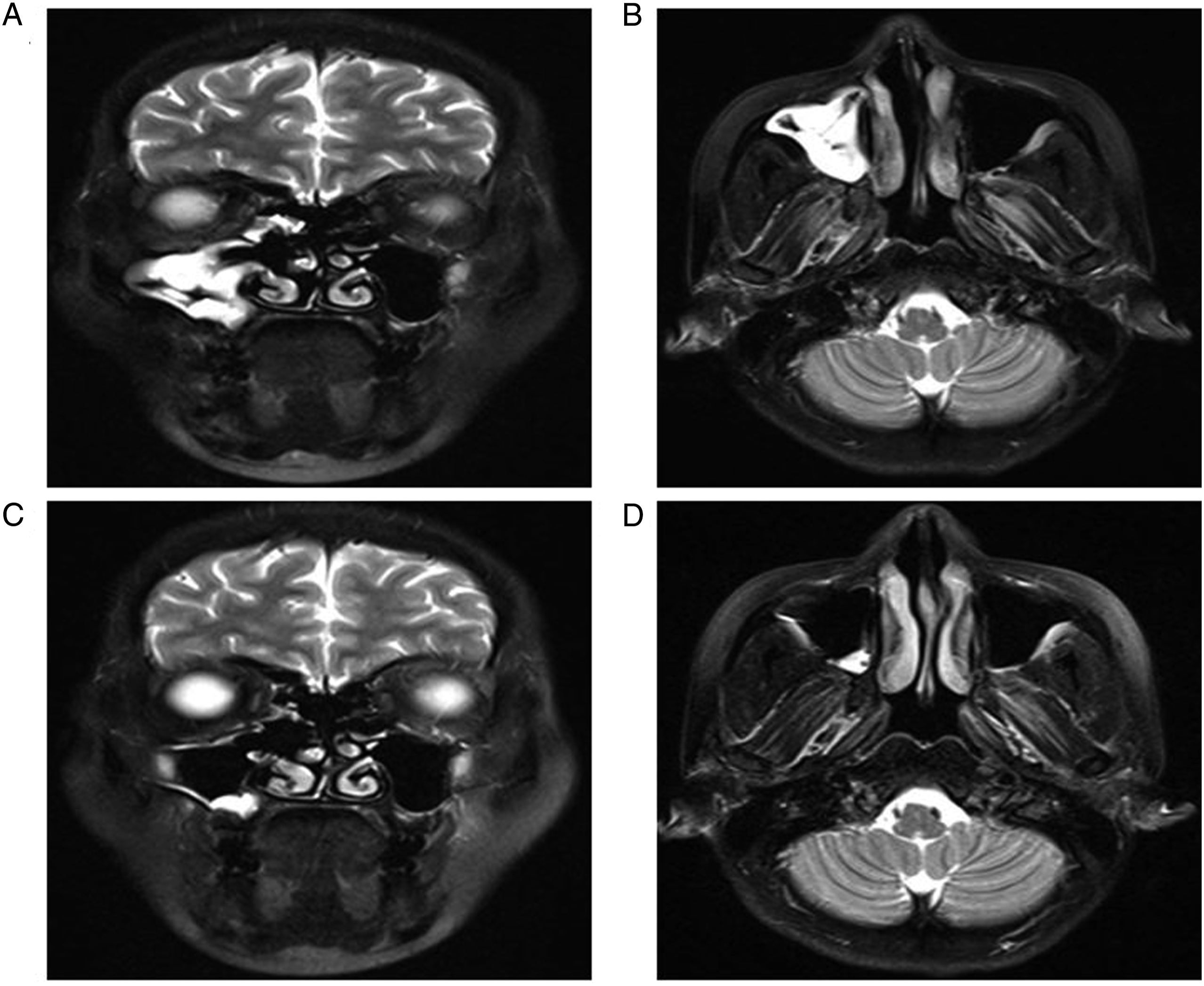
Case 5
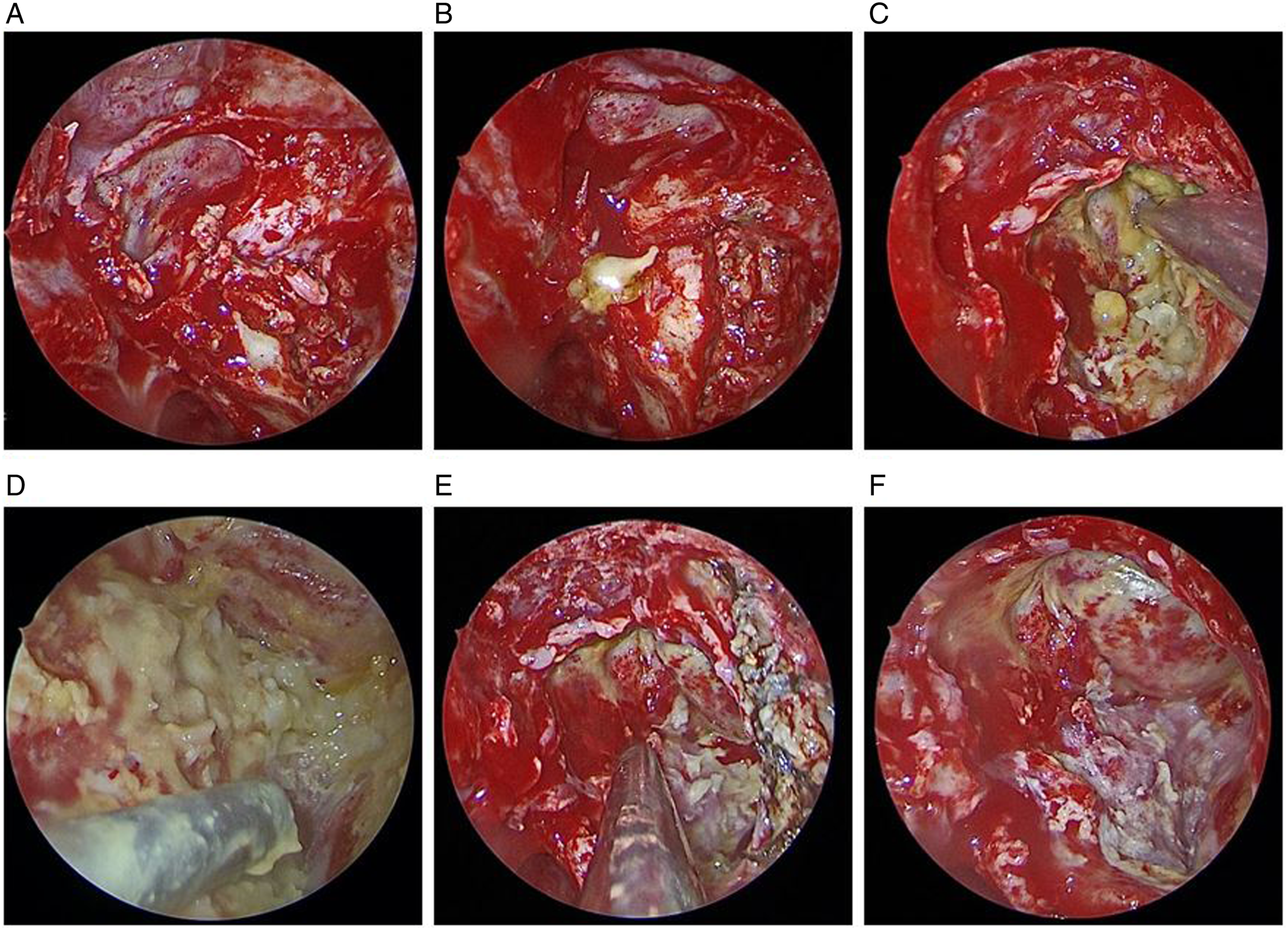
A 61-year-old male developed left nasal congestion and occasional mucopurulent excretion with ear tightness and hearing loss eight years ago. He was treated in another hospital and achieved partial improvement after medical treatment (details unknown). For further diagnosis and treatment, he received horizontal and coronal MRI scanning examinations and imaging results showed an intracranial and extracranial communicating expandable mass occupying the left middle skull base (Figures 5A and 5B). For the main steps of the operations, part of the middle turbinate was routinely excised, and the ostium of the maxillary sinus, ethmoid sinus, and sphenoid sinus were enlarged in preparation for exposure of the lesion. The left anterior wall of the maxillary sinus was exposed through a labial-sulcus incision and enlarged with forceps. A circular incision was made on the posterior wall of the maxillary sinus under endoscopy to expose the pterygopalatine fossa (Figure 6A). Then, the inner and lateral plates of the pterygopalatine process were removed with yellow discharge overflow (Figure 6B). Next, the boundary was further expanded along the edge of the cyst until it was completely exposed and removed (Figure 6C-E). The remaining wound showed the dura of the middle skull base and internal carotid artery (Figure 6F). No obvious cerebrospinal fluid leakage was observed. The middle turbinate mucosa was used to cover the middle skull base and internal carotid artery. Postoperative imaging examination showed the process of lesion regression without recurrence (Figure 5C-F). Preoperative and postoperative magnetic resonance imaging scan. (A and B) T2 sequences demonstrated an intracranial and extracranial communicating mass in the left middle skull base containing fat components and compressing the left temporal lobe and the internal carotid artery. (C and D) On the first postoperative day, T2 sequences showed perioperative hemorrhage and edema around the temporal lobe. (E and F) T2 sequences showed complete dermoid cyst removal without any recurrence at the four-month follow-up. Endoscopic endonasal resection of dermoid cyst in left middle cranial fossa floor. Endoscopic appearance of dermoid cyst (A-D) and gross total resection (E and F).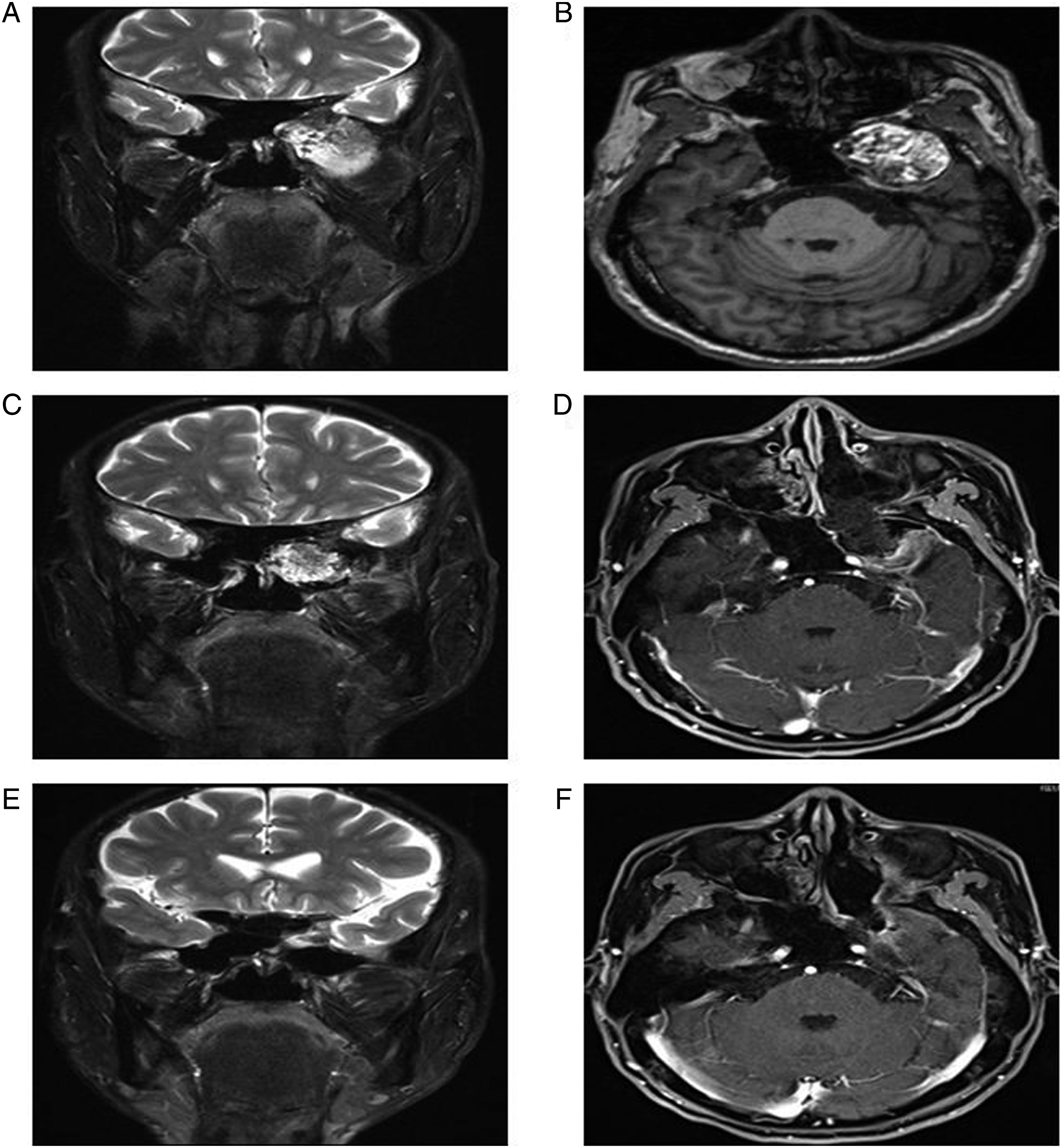
Results
Clinical Data of Enrolled Patients.
Discussion
Skull base DCs as rare congenital diseases mostly occur in the midline region of the brain involving the MCF. The lesions mostly originate from the middle cranial fossa floor, the infratemporal fossa, the cavernous sinus, and the petrous apex. 5,6 To date, there have been no conclusive reports on the clinical features, therapeutic options, and prognostic outcomes of DCs arising from the MCFF. In this article, we summarized 5 patients’ clinical course with DCs originating from the MCFF at our center.
To our knowledge, the clinical manifestations of DCs are varied and lack of specificity, and neurological involvement has certain clinical significance. In our study, only one case was found to have neurological symptoms at onset. These cysts can enlarge before any symptoms or signs appear due to their slow growth, which depends on the location of the lesion and compression of adjacent structures. The common symptoms include focal neurological deficits, headaches, or meningitis, 7,15 and other less common manifestations, including seizures, hydrocephalus, visual field defects, exophthalmos, and oculomotor palsy. These common clinical manifestations are also seen in our data. Asymptomatic intracranial DCs are usually diagnosed by chance, and we also described one case in which the lesion was discovered by physical examination. Cysts can become spontaneous ruptures, traumatic ruptures, or rupture during surgery, 16,17 but these situations were not observed in our cases. Once ruptured, cyst components spread into the subarachnoid space and may present with a variety of symptoms and signs, including headache, nausea, vomiting, visual impairment, dizziness, epilepsy, aseptic chemical meningitis, hemiplegia, and psychiatric changes. 7,15
The use of CT and MRI not only facilitates the diagnosis, but also helps in planning the surgical approach. 3,4 Our imaging findings conform to the general features of DCs being rounded, well-delineated nonenhanced unilocular cystic hypodense masses of variable sizes containing fat and capsular calcium. Notably, in one special case, T1-weighted MRI scans showed hypo- to iso- intense areas in the brain with contrast enhancement, while T2-weighted images showed hyperintense areas. We initially thought it was a schwannoma, but it was eventually confirmed as DCs by postoperative histopathological examination. Lipoma, epidermoid cyst, arachnoid cyst, craniopharyngioma, and teratoma should be considered in the differential diagnosis. Suppression of lipoma in fat-suppressed sequences and uniform visualization are important features for differentiating these lesions from DCs. Thus, histopathological examinations remain the gold standard for diagnosis.
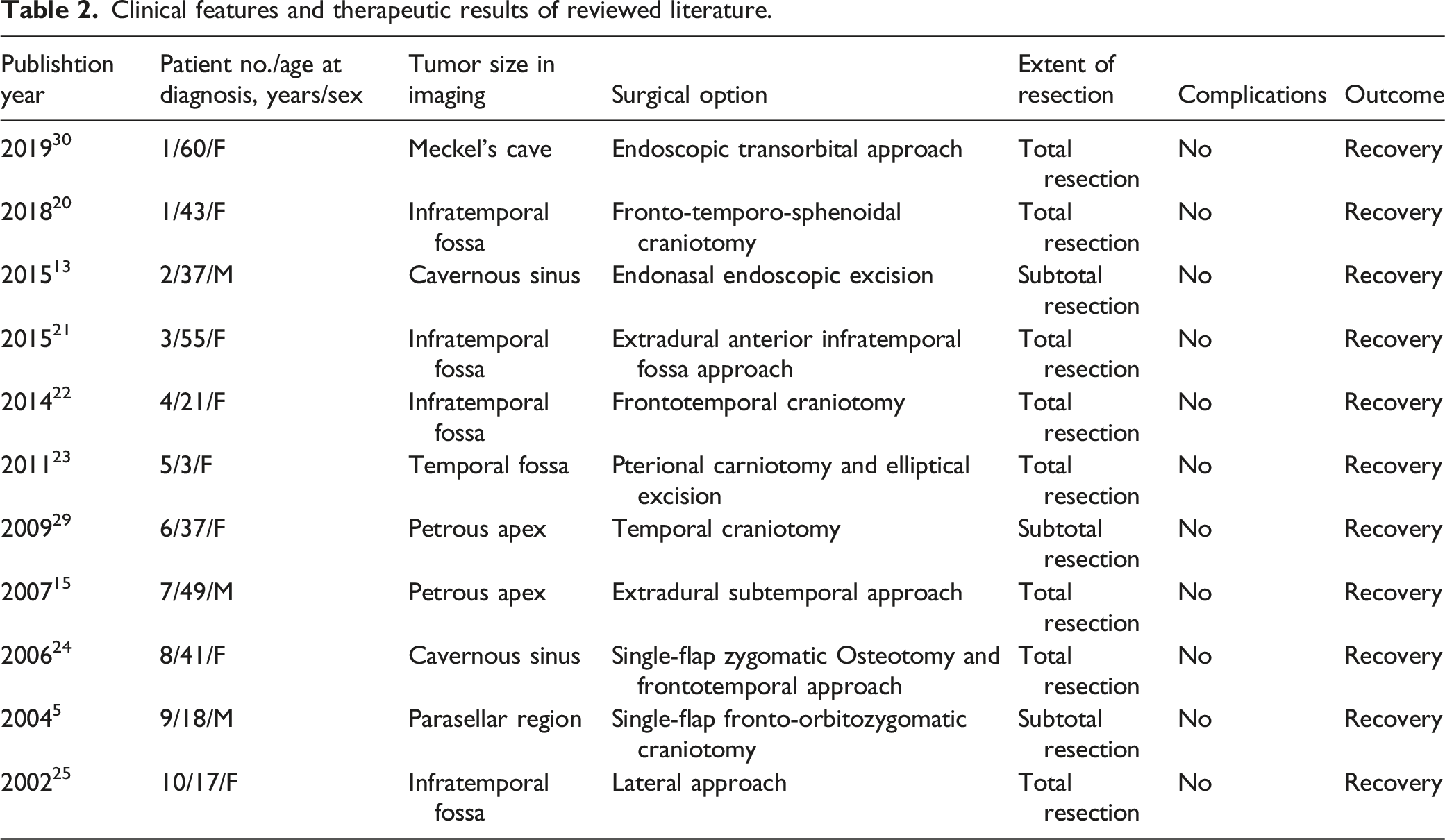
Clinical features and therapeutic results of reviewed literature.
Conclusion
Dermoid cysts are basically benign and generally become symptomatic secondary to their mass effect on neural structures. Radiological imaging is still essential for diagnosis, but ultimately depends on pathological examinations. EES is considered safe and effective in the treatment of DCs in MCFF. A larger sample size and longer follow-up time are needed.
Footnotes
Acknowledgments
The authors thank the researchers of the original studies included in this paper.
Author Contributions
HX drafted the manuscript. WL performed the statistical analysis. DW conceived and designed the study manuscript. HW and HZ acquired the data. LH supervised the study and corrected the manuscript. All authors contributed to the article and approved the submitted version.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was financially supported by the National Natural Science Foundation of China (No. 81870703), Shanghai Shen Kang Hospital Development Center (SHDC12018118), Science and Technology Commission of Shanghai Municipality (20Y11902000, 21ZR1411700), and Shanghai Municipal Health Commission (201940143).