
Abstract
Background
Based on our cadaveric study findings and the clinical practice, the improved submental island flaps (SIF) used on a case series to reconstruct postoperative defects were reviewed and analyzed, to summarize the technical operation of flap cutting and propose the anterograde anatomical technique of point-line-plane alignment.
Methods
The cadaveric study was carried out first and a case series of about 23 head and neck tumor cases that underwent one-stage SIF repair were reviewed and followed up. The intraoperative anatomy, the technical essentials for vascular pedicle protection and submandibular lymph nodes treatment, and the rational design of flap incisions were analyzed and described.
Results
Most patients (21/23, 91.3%), comprising 19 males and 4 females with a mean age of 59 years, recovered completely from the application of SIFs in the repair and reconstruction of head and neck tumors; Only 2 patients experienced partial flap necrosis, which resolved following a local dressing change. The predominant donor site complication was transitory paralysis of the mandibular marginal branch of the facial nerve (MMBFN) (3/23, 13.0%), and the donor site was closed in one stage without skin grafting. The hair growth on skin flaps was not an issue for male patients requiring postoperative radiotherapy.
Conclusions
SIF is a viable choice for correcting abnormalities of the head and neck tumor with the convenience of flap cutting and the effectiveness of the repair. In addition, it permits simultaneous treatment of the lymph nodes in the region I.
Background
At present, surgery is still the mainstay of treatment for head and neck malignancies, and the thoroughness of surgery determines patient outcomes. However, due to the complexity of head and neck anatomy and the special functions of important structures and organs, the reconstruction of postoperative defects and functions is particularly important. 1 Today, there are many kinds of pedicled tissue flaps and free skin flaps, which make it possible to perform operations that were previously neglected, thus improving the thoroughness of surgeries. Among them, the pedicled submental island flap (SIF) proposed by Professor Martin in 1993 has gradually become one of the most used flaps for head, neck, and face repair. 2 Because of its reliable vascular pedicle, high survival rate, and simple operation, it has increasingly become one of the commonly used means for the reconstruction of head and neck defects. 3 However, it was found in literature and clinical application that the vascular pedicle of the SIF, especially the veins, still had some variation, and there were still reports of necrosis of the flap.4,5 To improve the positioning and protection of vascular pedicle of the flaps and to enhance the survival rate of skin flaps, a case series with head and neck defects repaired by this flap in our department in the past 5 years were reviewed and analyzed, and in combination with the anatomical findings, this paper summarized the technical operation of flap cutting and proposed the anterograde anatomical technique of point-line-plane alignment.
Methods
Ethics Statement
This study was approved by the Institutional Review Board and Ethics Committee of Beijing Tongren Hospital, Capital Medical University, and the written informed consent was approved to waive by the ethics committee, for this is a retrospective case series report. Our research complies with the principles of the Helsinki Declaration and all patient information was kept in strict confidence.
The surgical recommendations from the findings of the cadaveric study
The cadaveric study was carried out first and 3 adult cadavers, including 2 males and one female, were newly perfused by femoral artery and vein. The applied anatomy of SIF in the submental and submandibular regions was performed.
The findings of the cadaveric study were as follows, which were consistent with previous studies:6,7 (1) The submental artery is one of the major branches of the facial artery’s cervical portion, which arises from the facial artery at the inferior border of the mandible (IBM), with a beginning point around 1 centimeter distant from the mandibular margin and a trunk length of approximately 6 centimeters; It passes anteriorly and inwardly through the medial sulcus of the SMG and the surface of the mylohyoid muscle (MhM) before terminating at the anterior belly of the digastric muscle and the mandible. There are tiny branches to the SMG, MhM, digastric muscle, and mandibular periosteum along this path. In addition, there are 1–4 cutaneous perforators that penetrate through the platysma muscle and distribute beneath the dermis. (2) Under the dermis and the deep and shallow surfaces of the digastric muscle, the cutaneous perforator and ramus digastricus of bilateral submental arteries are abundantly anastomosed around the midline, which can give dependable perfusion to the contralateral submental and submandibular skin, which can nourish a flap measuring approximately 18 cm in length and 7 cm in width. (3) The SIF’s venous drainage occurs via the submental vein to the facial vein, with the diameter of the vein ranging from 1.0 to 2.9 mm (average: 2.2 mm), and the submental vein is accompanied by the submental artery at its distal end. most submental veins drain into facial veins and then connect with superior thyroid veins to form internal jugular veins, whereas a few drains into external jugular veins; Variable venous drainage was observed. (Figure 1) The findings of the cadaveric study. A. the submental artery is clearly displayed. After emerging from the facial artery, it runs along the IBM and the deep side of the upper surface of the SMG, and branches to the SMG, MhM, digastric muscle, and mandible. The submental vein runs with the artery at the distal end. B. the submental island flap is pedicled with the submental artery and vein, and the submental artery is 6 cm long. Note: IBM, inferior border of the mandible; SMG, submandibular gland; MhM, mylohyoid muscle.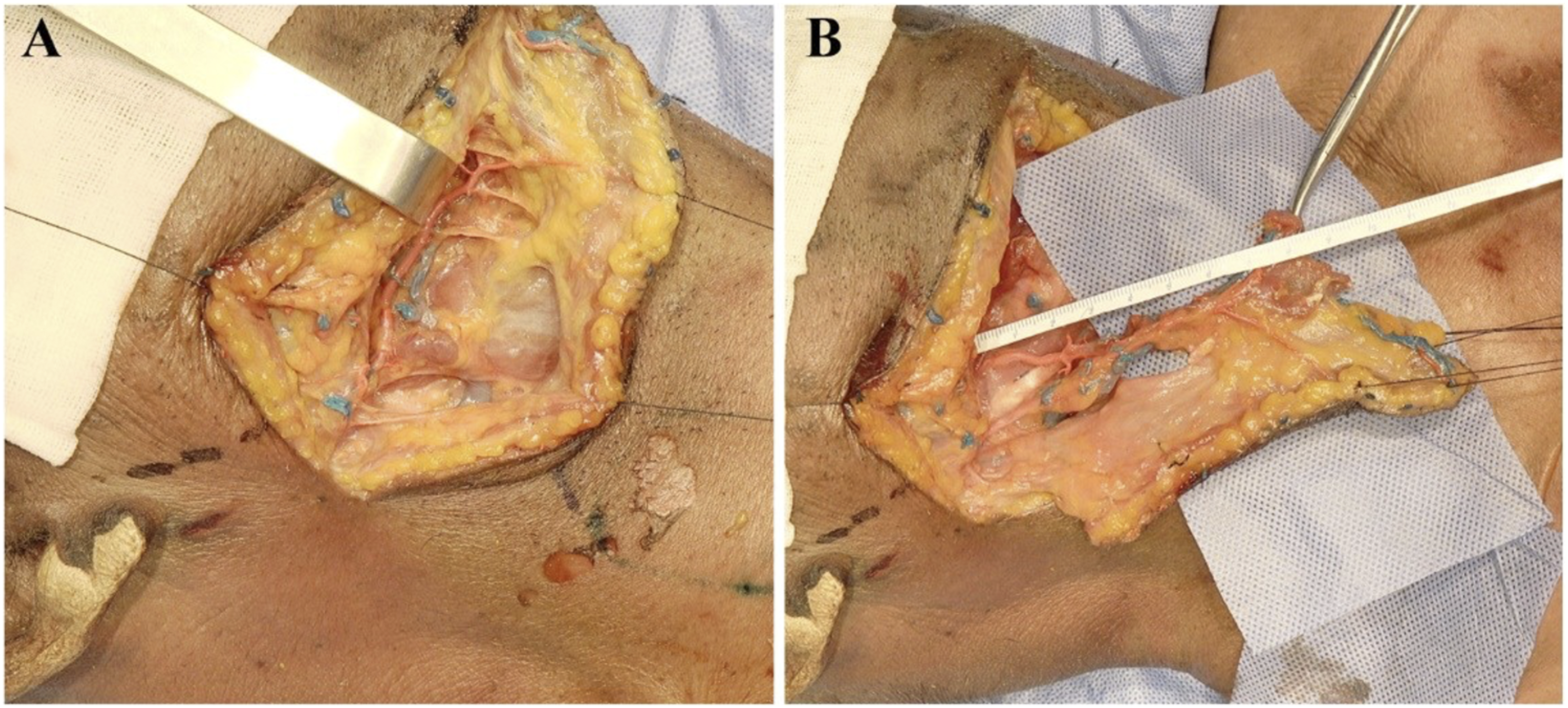
Clinical Application
From May 2017 to December 2021, 23 cases with head and neck tumors undergoing one-stage SIF repair at Beijing Tongren Hospital, Capital Medical University, were included in this case series report.
Inclusion and Exclusion Criteria
The inclusion criteria were diagnosed with head and neck malignancies undergoing reconstruction surgery with SIFs. Exclusion criteria were as follows: 1) the SIF harvest was aborted intraoperatively; 8 2) patients underwent chemotherapy before the surgery; 3) combined with diabetes and other factors that affect wound healing; 4) submandibular or submental lymph node metastases were diagnosed by rapid intraoperative pathology; and 5) the transverse diameter of the defect area was >8 cm.
Observational indexes
Postoperative defects, including hypopharynx, tongue base, oropharynx (tonsil), hard palate, facial skin, auricle, and surrounding skin, were collected. Other information about the neck lymph node dissection, preoperative/postoperative radiotherapy in the neck, and major complications of donor site were reviewed.
Flap Operation
The procedure for finding and protecting the common facial vein that drains the submental vein to the external or internal jugular vein had been documented in detail with precise photos in the surgical note for the retrospective study.
Body surface projection of the vascular pedicle was performed as follows: first, the facial artery was palpated along the IBM within 1–2 cm of the mandibular angle, and point A was indicated. From point A, the IBM’s vertical line was drawn, and point B was defined as 1 cm from the vertical line to the IBM. A perpendicular line was drawn down the middle of the chin, a horizontal line was drawn from point B, and point C was the point of junction with the chin midline. The line from point B to point C was utilized as the body surface projection line of the submental vessels and most of the skin island was designed within the BC line region.
The size of the skin island was designed based on the original site and size of the primary cancer, with the main body of the skin island positioned in the ipsilateral submental and submandibular regions. The flap was adequately stretched to the contralateral submandibular region, generally without beyond the level of the contralateral-mandibular angle, in accordance with the surgical resection range. The donor patch of skin with a width of less than 8 cm in the anterior midline of the neck can be closed with direct sutures, and the flap width can be determined by pinching. To prevent the flap supply area from being unable to be closed and sutured at once, the flap size was customized based on the size of the defect and the condition of the neck.
Utilizing the dissection approach of the point-line-plane anterograde flap, the flap’s long axis was created along the BC line. The superior incision was close to the IBM and might be adjusted down 1–2 cm to eliminate the flap hair problem in male patients with a dense chin beard.
Beginning at point A, the skin and subcutaneous tissue were sequentially removed to reveal the platysma muscle layer. To safeguard the facial arteries and veins and the mandibular marginal branch on the surface, the platysma muscle was carefully separated and dissected, particularly in the ipsilateral mandibular angle region. After the complete explosion of facial arteries and veins and dissection downhill along the facial artery around 1–2 cm below the IBM (point B), the submental artery from the facial artery can be in a relatively stable location, as depicted in Figure 2. The platysma muscle was successively incised along the IBM towards the submental midline, exposing the anterior belly of the digastric muscle in the submental region. Then, the attachment of the anterior belly of the digastric muscle to the submental mandible was severed to safeguard the branch vessels from the submental arteriae to the digastric muscle and skin island region. The platysma myoides was cut anteriorly to the distal contralateral end of the flap. The subcutaneous and platysma layers of the flap were then gradually sliced and separated along the deep surface of the platysma muscle, and the flap was elevated to the midline of the submental region. To protect the submental vascular branches, the anterior belly of the digastric muscle was kept on the flap following the direction of the flap’s superior incision. Then, dissection was done along the surface of MhM, and the distal branches of ipsilateral submental vessels towards the mandibular hyoid muscle and the oral floor were observed and ligated/severed. Along the submandibular region, anatomical dissociation was continued, leaving the submental vessels beneath the flap to the facial artery. The facial artery branch close to the surface of SMG was detached and ligated with extreme care. In addition, the portion of facial vein that extended from the submental vein was dissected and dissociated along the facial vein, and in most patients, veins led to the internal jugular vein. Surface projection of the submental artery. Point A is the body surface point of the ipsilateral artery at the IBM, and point B is the perpendicular point from point A to 1 cm below the IBM. Point C is the intersection of the vertical line under the chin and the horizontal line from point B. The line of BC is the projection line of the submandibular area of the submental arteries and veins. Note: IBM, inferior border of the mandible.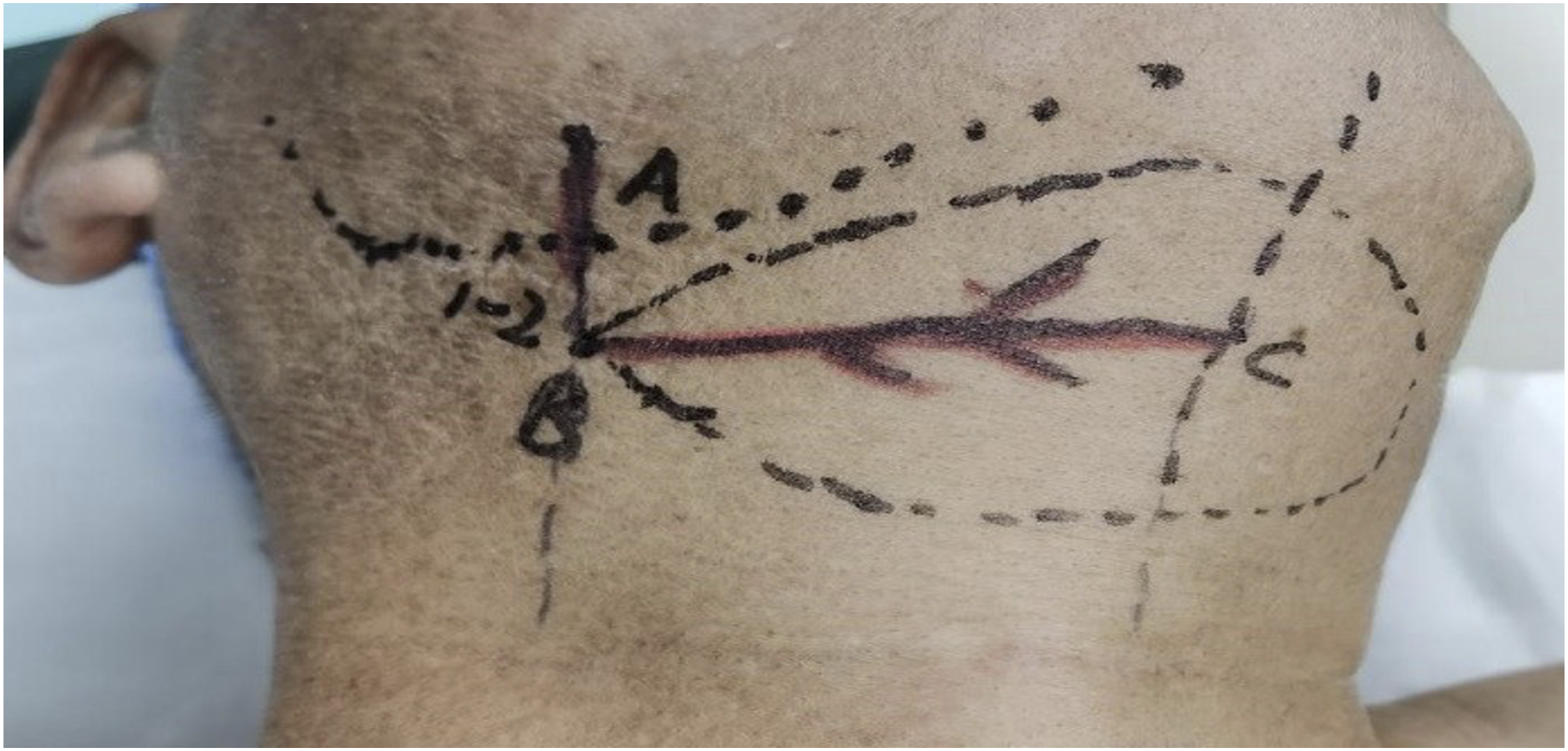
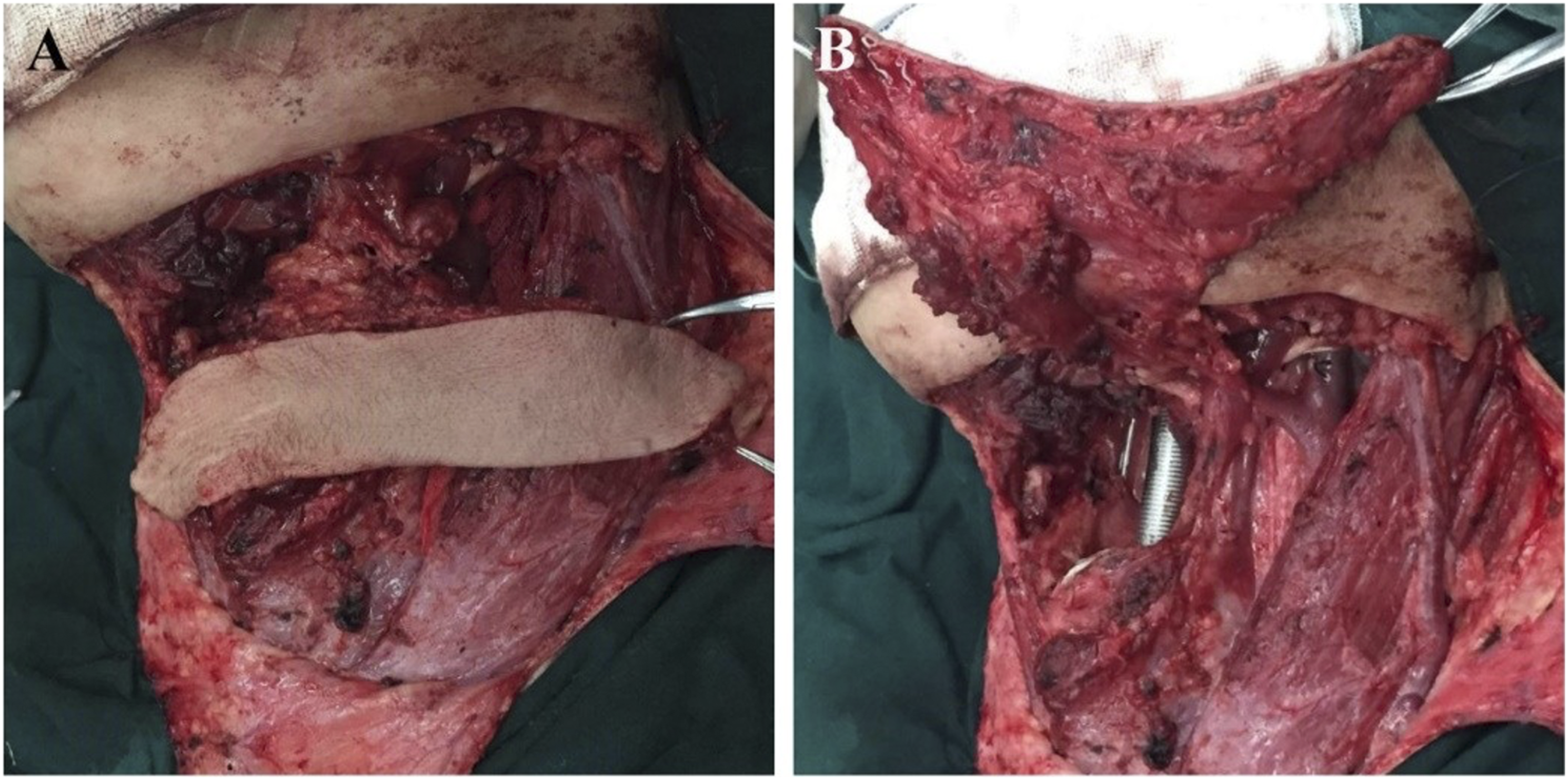
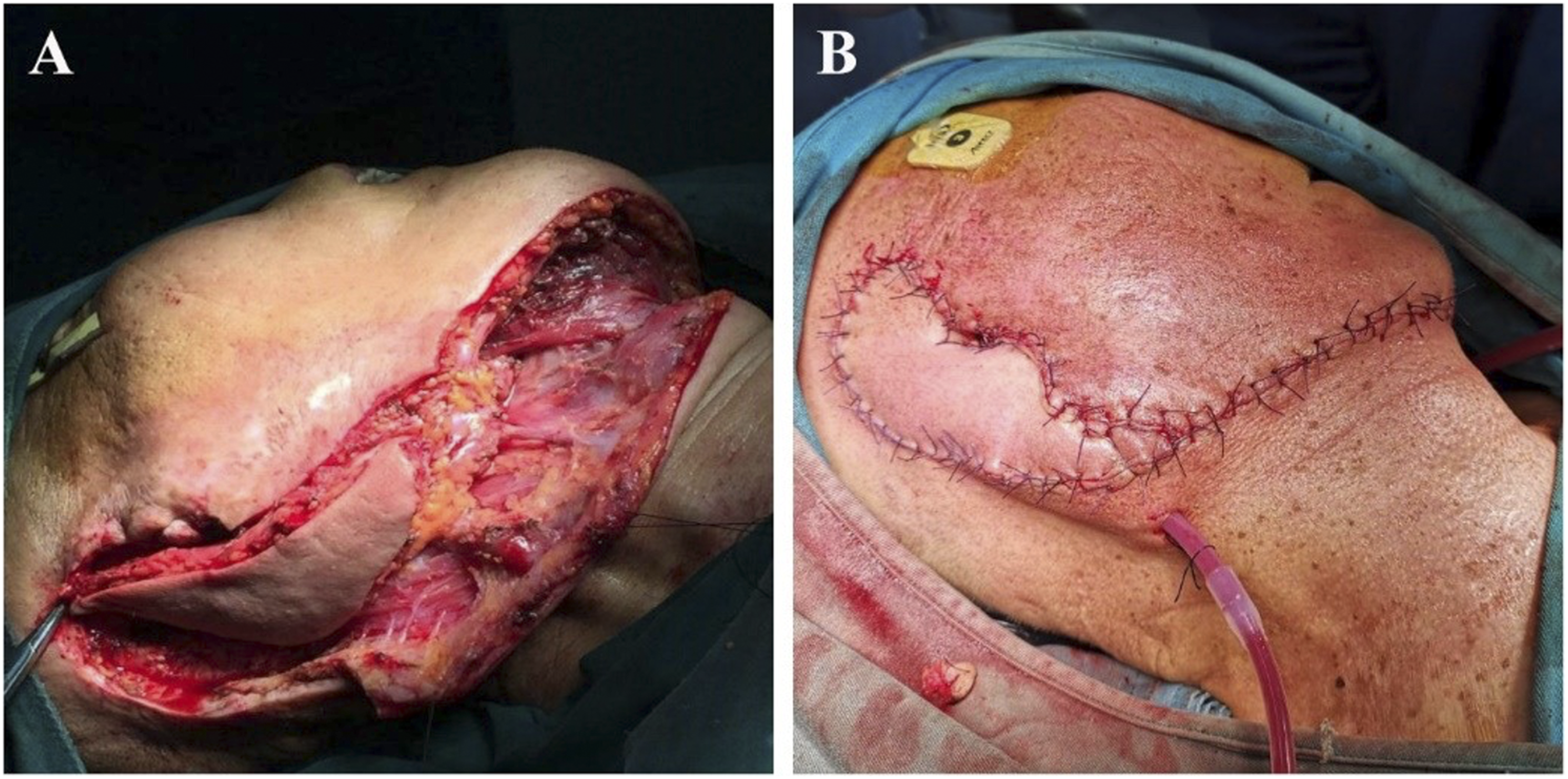
Flap transposition: after vascular pedicle dissociation, flap transposition was performed according to the surgical defect area. The flap was transposed to the defect area of the inferior pharynx. Due to the proximity of the anatomical position of the flap and the inferior pharynx, the flap transposition range was small, the length of the required flap vascular pedicle was not long, and the rotation angle of the flap vascular pedicle was not large. When the flap is transposed to the defect area of the palate, base of the tongue, and the tonsil, the distal end of the undisconnected facial artery and vein will hinder the upward and inward pulling of the flap to a certain extent; therefore, when the flap is transposed to the defect area of the palate, base of the tongue, and the tonsil, the distal end after the submental artery was generally cut off and ligated, and the distal end after the submental vein joins into the facial vein was cut off at the same time. The repair of the submental island flap for auricle and parotid gland defects was relatively simple; after the distal end of the facial artery and vein was cut off and ligated, the flap would be rotated and transposed to the operation area. Figures 3–5. Hypopharyngeal carcinoma (pyriform fossa carcinoma, T2N1M0). Selective dissection of lymph nodes in Level II-IV region of the ipsilateral neck was performed to preserve the external carotid artery and internal jugular vein. The ipsilateral SIF was performed, and the veins flowed into the internal jugular vein system. Flap transposition was performed to repair the ipsilateral hypopharyngeal wall and piriform fossa defects. A. Ipsilateral SIF prepared intraoperatively. B. Pharyngeal defect after ipsilateral hypopharyngectomy. C. Repairing pharyngeal cavity defect with medial inversion of submental island flap. D. Reconstruction of hypopharyngeal lateral wall with partially aligned suture showing the flap and pharyngeal cavity defect on the opposite side. Note: SIF, submental island flap. Patients with base tongue carcinoma (well-differentiated squamous cell carcinoma, T2N0M0). Bilateral submandibular and submental lymph nodes were dissected during the operation, and no lymph node metastasis was found by intraoperative pathology. Then, a SIF pedicled with the ipsilateral submental arteries and veins was taken, and the vein merged into the internal jugular vein system. Flap transposition was performed to repair the tongue base and supraglottis defects. A. Prepared SIF. B. The tongue base and supraglottis defects. Note: SIF, submental island flap. The squamous cell carcinoma of the auricle. The auricle and surrounding skin were excised, and the incisal margin was negative during the operation. In addition, lymph node dissection in parotid and ipsilateral submandibular regions was performed, and no lymph node metastasis was found during the operation. The skin defect of the auricle and parotid gland was repaired by transposition of ipsilateral SIF. A. Defect after auricle excision, the submental island flap is rotated to the defect area. B. The image after suture of SIF for the auricle defect repair. Note: SIF, submental island flap.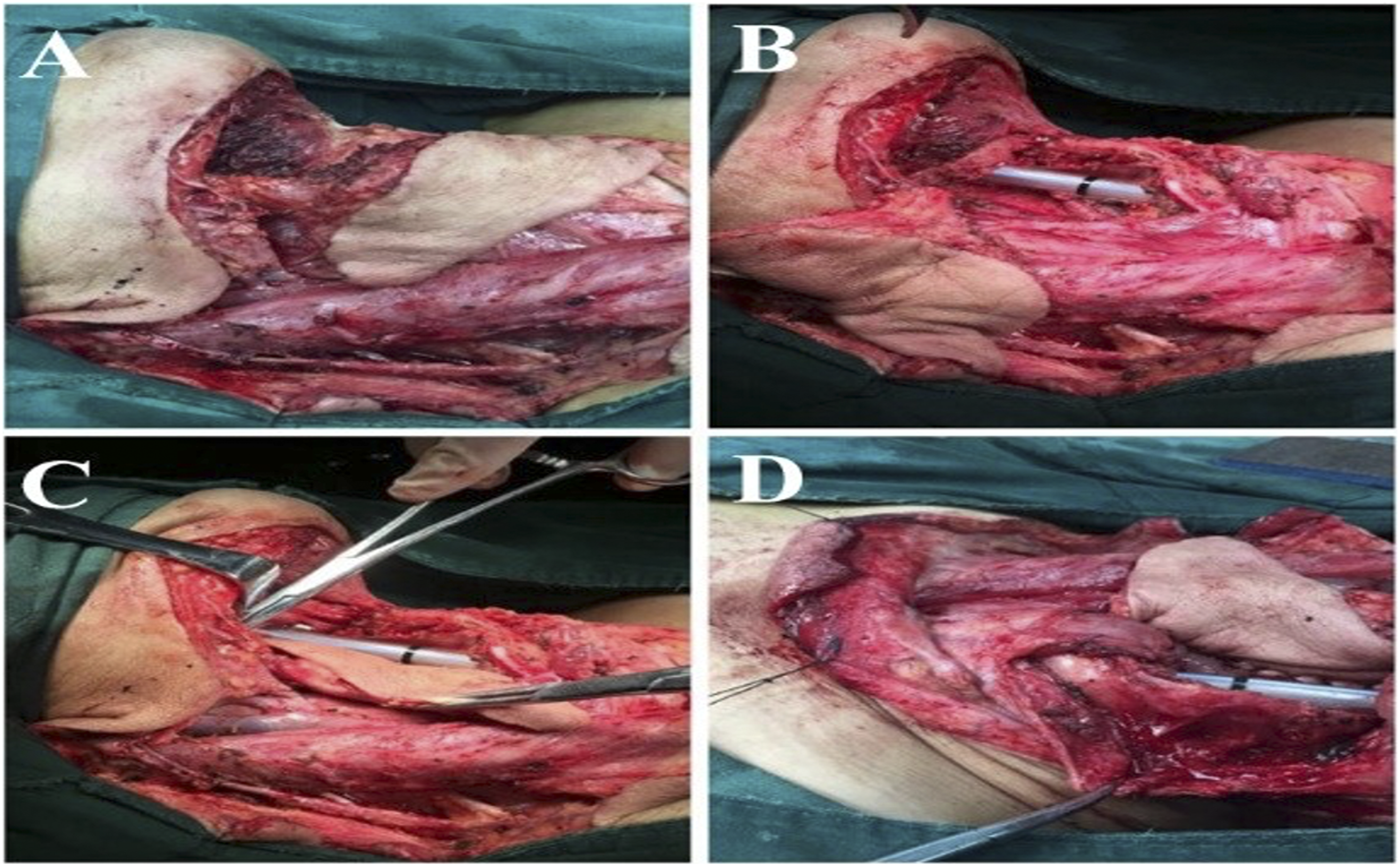
Results
A total of 23 head and neck malignant cases reconstructed with SIFs were reviewed and evaluated, including 19 male and 4 female patients with a mean age of 59.
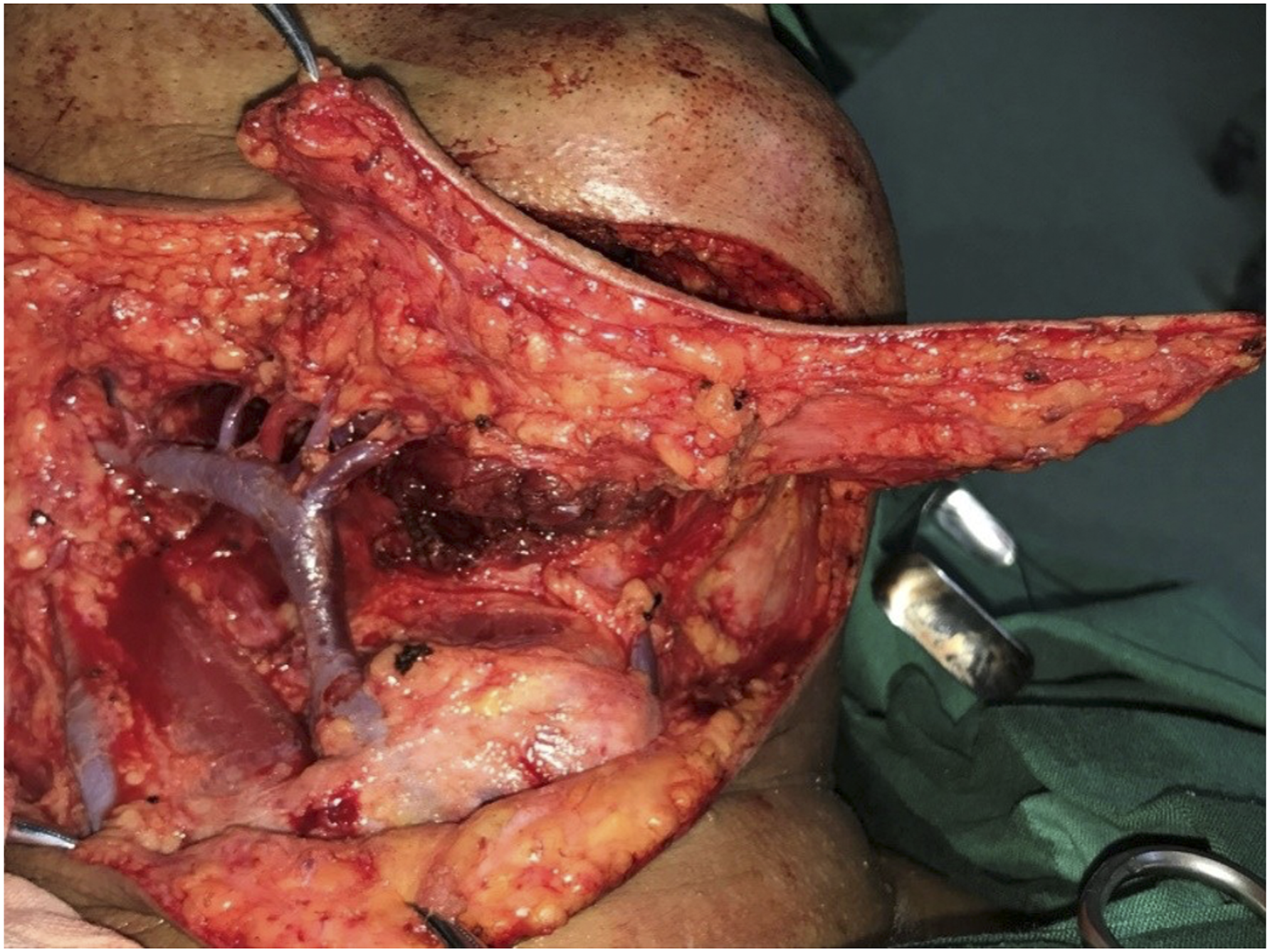
According to the architecture of the flap’s vascular pedicle, anterograde flap anatomy was performed on all 23 patients. Figure 2 depicts the body surface projection of the vascular pedicle that was performed first. In eleven cases, the submental vein emptied into the facial vein before joining the superior thyroid vein and the internal jugular vein; correspondingly, in 7 cases, after flowing into the facial vein, the submental vein drained into the external jugular vein. As depicted in Figures 6 and 7, the submental vein was intricate in 5 instances which had many confluence branches with the facial vein, external jugular vein, and anterior jugular vein. Anatomy of the facial arteries and veins in the mandibular angle area and the marginal mandibular branches. Variations in the venous confluence of submental island flaps. The patient had 3 cutaneous confluence veins which flowed into the facial vein and then joined with the common trunk of the superior thyroid vein and flowed into the internal jugular vein. The middle one of 3 veins was the submental vein.
Patients with head and neck malignancies undergoing reconstruction surgery with SIFs.
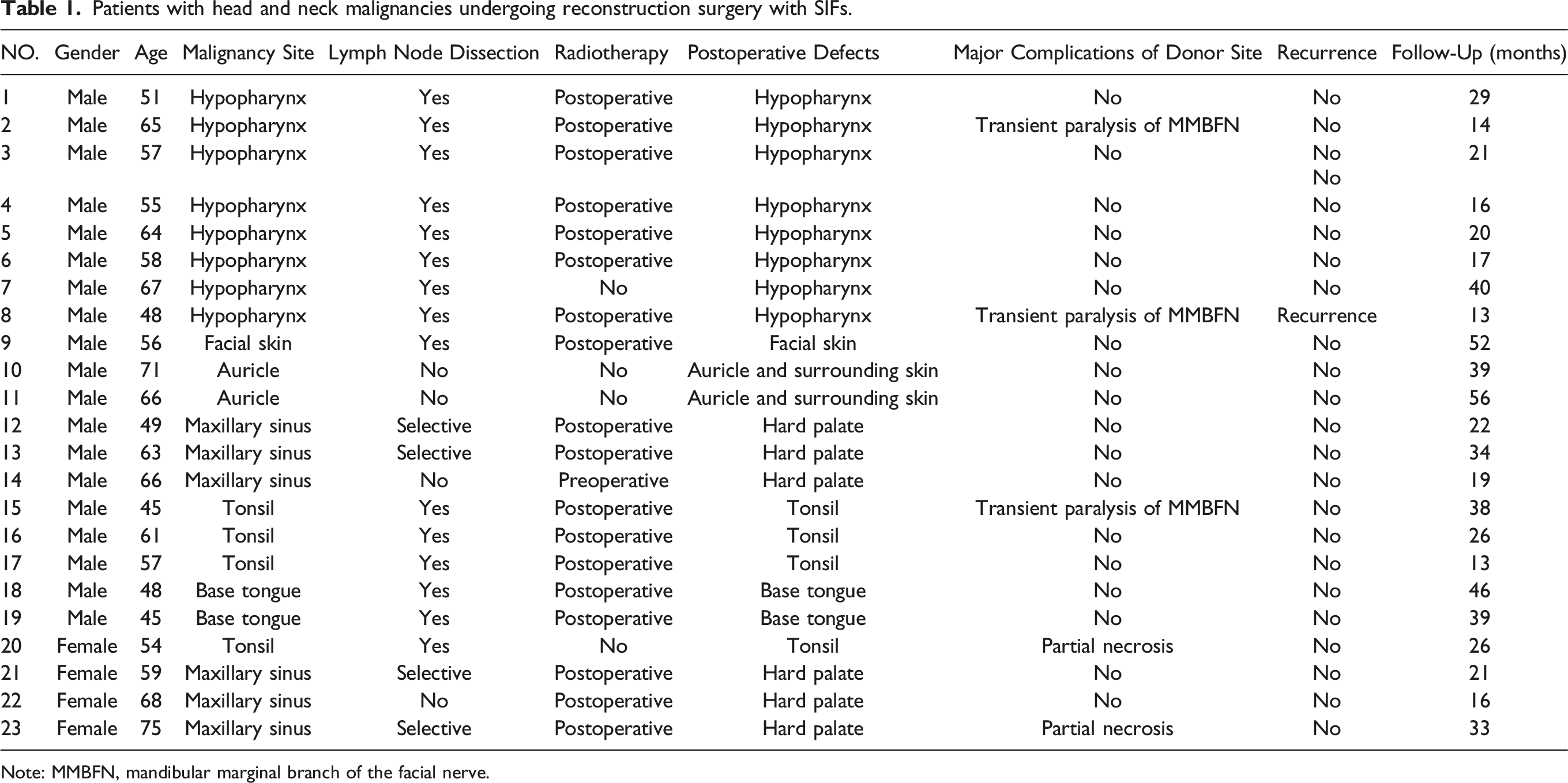
Note: MMBFN, mandibular marginal branch of the facial nerve.
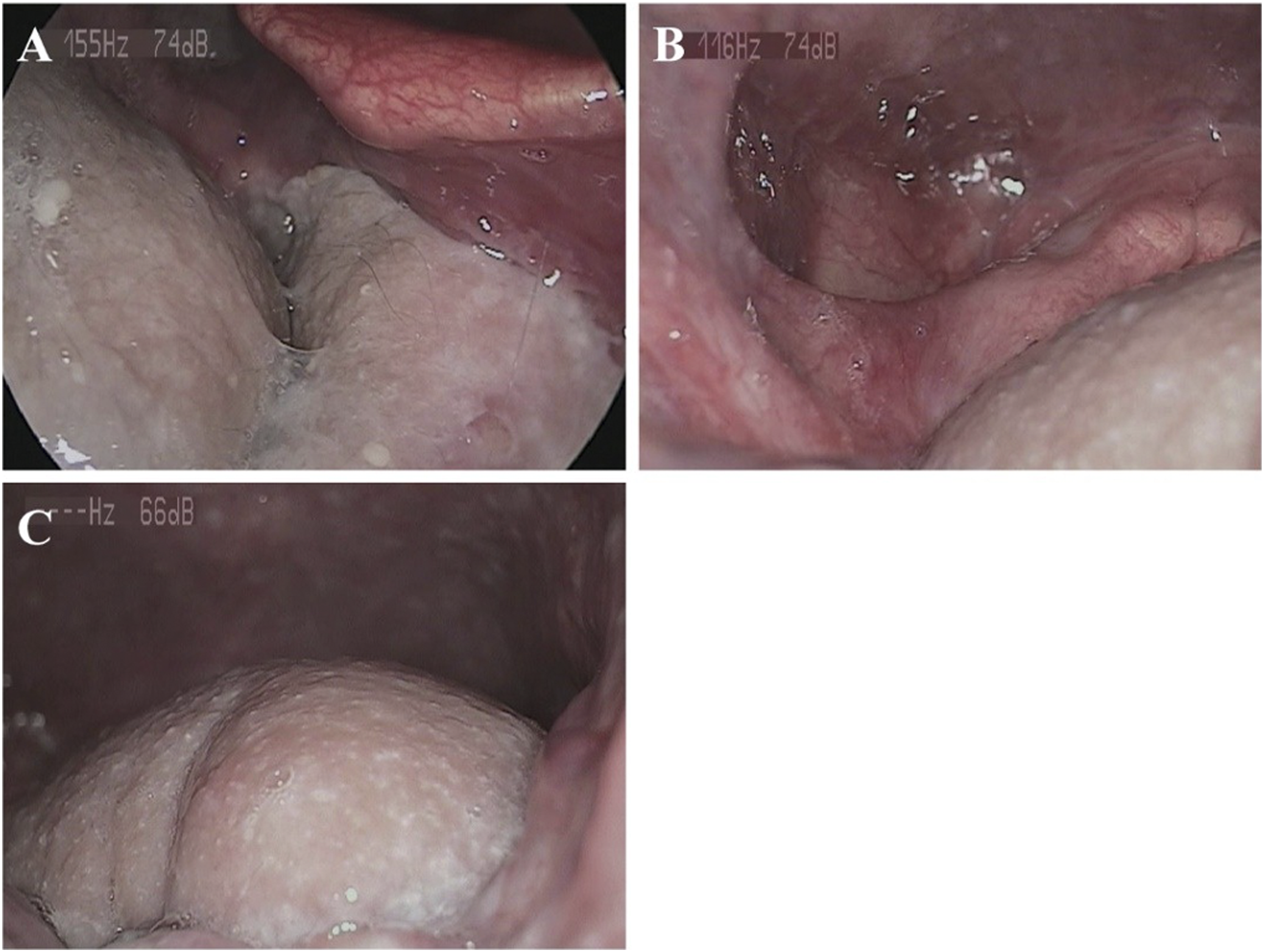
One month after the operation of mucoepidermoid carcinoma of the tongue base. The skin flap survived well and the hair grew. Base tongue carcinoma was repaired with the SIF. One month after radiotherapy, the flap was smooth and complete, and the glottis occlusion was effective in preventing accidental swallowing and choking, with no hair found. A. Laryngoscopy image of one month after of tongue base defect repair with SIF. B. Postoperative laryngoscopy image of tongue base SIF after radiotherapy. C. The SIF was used to reconstruct the tongue base defect, and the glottis was well covered under the laryngoscope. Note: SIF, submental island flap.

The squamous cell carcinoma of the auricle. Half a year after the operation, the skin flap survived well, the color was consistent with the face, and the facial hair did not affect the appearance.
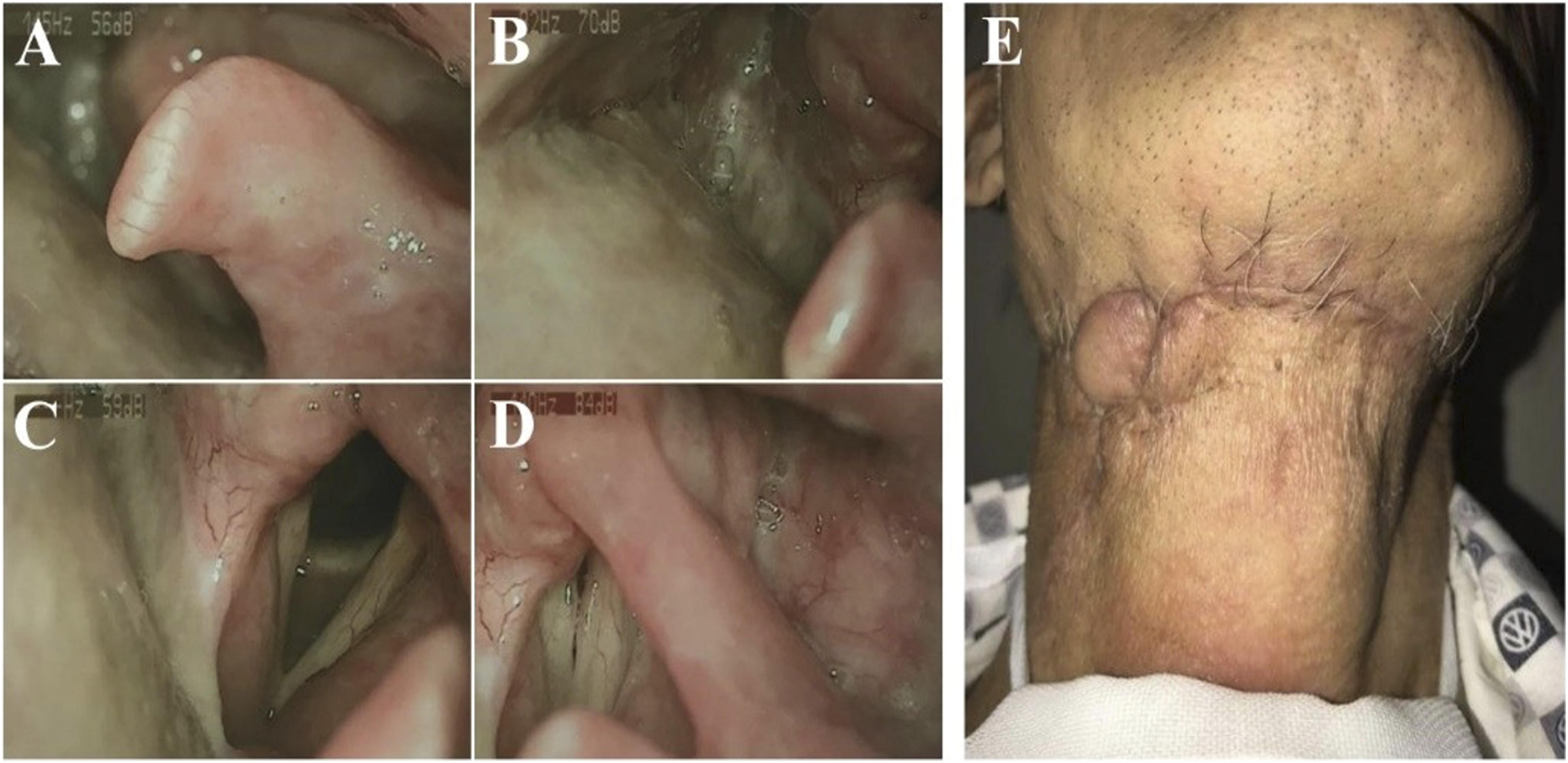
Four years after SIF repair of hypopharyngeal carcinoma. A-D. Postoperative laryngoscopy images of hypopharyngeal carcinoma with SIF repair, showing the reconstructed piriform fossa. E. Postoperative view of the donor site of the SIF, with the small right skin island as the observation window of the SIF in the pharyngeal cavity. Note: SIF, submental island flap.
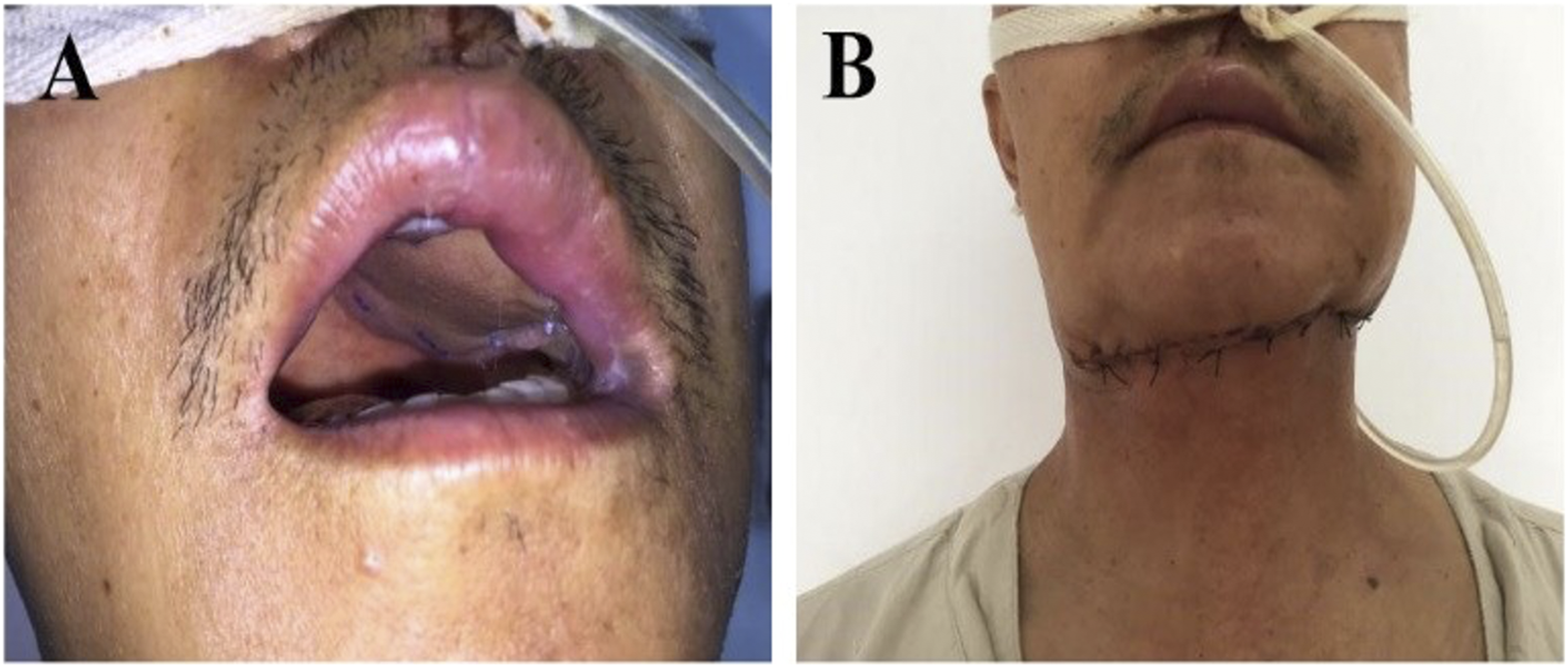
The maxillary sinus carcinoma. Maxillectomy and SIF reconstruction for palatal defect were used. 2 weeks after the operation, the intraoral reconstruction using the submental island flap survived well, and the incision in the submental donor area was concealed and not apparent in the non-head-up position. A. Intraoral view 2 weeks after surgery for SIF repair of the hard palate defect after maxillectomy. B. SIF donor site appearance 2 weeks after surgery. Note: SIF, submental island flap.
Discussion
The SIF, first proposed by Martin, et al. in 1993, is a relatively novel approach for the reconstruction of head and neck deformities. 2 The color and texture of the SIF match the skin of the face and neck, and the appearance is natural; the vascular pedicle of the flap is long, and the rotation range is large, which can provide a large amount of flap tissue; the vascular anatomy of the flap is constant, the blood supply is abundant, and the survival rate is high; the donor site has no hair issues, the incision is relatively hidden, and the cosmetic effect is good; 9 in addition, the flap operation is generally straightforward, with a shorter time and fewer hospitalizations, which is preferred for by doctors. 10 With the advancement of anatomical study and broad clinical use of SIF, it has steadily become one of the key flaps for correcting head and neck abnormalities. However, it was found in literature and clinical application that the vascular pedicle of the SIF, especially the veins, still had some variation, and there were still reports of necrosis of the flap.4,5 In this study, combined with anatomical findings, the technical operation of flap cutting was summarized, and by reviewing the repair results of 23 patients who underwent SIF reconstruction for head and neck defects, the anterograde anatomical technique of point-line-plane alignment was proposed, which can further improve the positioning of the vascular pedicle of the flap and increase the flap survival rate.
Reconstructing oral cavity and facial soft tissue abnormalities is a challenging endeavor. There are numerous flap options, each with their own pros and disadvantages. Local and regional axial pattern flaps, random pattern flaps, and free flaps include these flaps. Particularly useful for facial soft tissue abnormalities are local flaps produced from cervical skin. These flaps fit the skin’s color and thickness well. Nonetheless, they have limitations, including variable viability and restricted mobility. 11 With little donor site morbidity, no need for microvascular skill, and a large arc of rotation, the submental island flap has been used to treat abnormalities in the lateral skull base, face skin, maxilla, and oral cavity. 12 A study found that submental island flap repair of the oral tongue has comparable functional outcomes to radial forearm free flap reconstruction, with less donor site morbidity, faster surgical time, and shorter hospitalization length. 13 In this study, based on the anatomy of 6 submental blood vessels of 3 freshly perfused cadavers (Figure 1), the projection line of submental blood vessels was determined, and the long axis of the flap was designed along the projection line so as to prevent dissociation from the blood vessels, reduce the damage to submental artery branches, and prevent the flap from detaching from perforators. In addition, the anterograde point-line-plane anatomy was used. First, the location of the submental artery of the facial artery was identified, and the vascular pedicle was dissected retrograde around the facial artery trunk to safeguard the vascular pedicle and the MMBFN. Moreover, while ensuring that the trunk of the vascular pedicle was adequately protected, the flap was cut along the submental blood vessel anterograde to prevent the submental blood vessel and flap from becoming separated, thereby preserving the flap perforating branch of the submental blood vessel and the flap’s blood supply. In addition, the anterior belly of the digastric muscle was severed along with the flap, which significantly increased the flap’s blood supply. The SMG branch of the facial artery was carefully dissected, the SMG was excised as necessary, and the degree of rotation of the vascular pedicle of the flap was increased or decreased as needed to relieve compression of the vascular pedicle going through the tunnel. Thus, the vascular pedicle naked dissociation was achieved, which not only facilitated lymph node dissection in the ipsilateral submandibular region but also accounted for the efficacy of tumor therapy.14-16 Only one of the 23 patients enrolled retained the SMG in the tongue base. The remainder required delicate dissection of the vascular pedicle and the removal of the ipsilateral SMG, particularly for treating abnormalities of the palate and oropharynx, as the flap needed to enter the pharynx or palate through the deep surface of the jaw. The ablation of the SMG facilitates the passage of the vascular pedicle through a relatively narrow tunnel and decreases its entrapment. 17 In this study, most patients underwent ipsilateral lymph node dissection first, and SIF repair was used after submandibular lymph nodes were quickly confirmed without metastasis during the surgery by pathological examination; if submandibular lymph node metastasis was found during surgery, SIF repair was not used; patients with hypopharyngeal carcinoma combined ipsilateral and patients with cervical lymph node metastases would be treated with postoperative radiotherapy according to treatment guidelines.
There were some limitations in this study. First, the sample size from a single center was small, and this was a retrospective review, which only reflected the single-center experience. In addition, there were no other pedicled tissue flaps included in this study to analyze the comparative benefit of SIF and no data about the specific size of SIF to analyze the design strategy of SIF. Furthermore, it did not consider which head and neck malignancy benefited from SIF and the SIF was not raised before the neck dissection. More patients and various treatment methods from multi-center will be included in the future. Moreover, the relationship between size and viability of SIF, the kind of head and neck malignancies, and the surgical benefits of SIF will be examined.
Conclusion
SIF is a reliable multi-purpose flap for repairing head and neck defects due to the convenience of flap cutting, the constant vascular pedicle of the flap, completion in the same surgical site, high matching degree of elasticity and skin color, and high survival rate. Moreover, it allows for simultaneous treatment of lymph nodes in the region I. Therefore, SIF may be a good choice for head and neck defect repair after surgery.
Footnotes
Author Contributions
PL and HL conceived and designed the research. PL, HL, SD, JZ, XC, JF, and ZH collected the data. PL, HL, and SD analyzed and interpreted the data. PL prepared and wrote the manuscript. HL, SD, JZ, XC, JF, and ZH collaborated in the discussion and reviewed and revised the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Beijing Natural Science Foundation (No. 7122039).
Ethical approval
The study was approved by the Institutional Review Board and Ethics Committee of Beijing Tongren Hospital, Capital Medical University. Our study was a retrospective study, and thus the ethics committee exempted the informed consent requirement for patients. Our study adheres to the principles of the Declaration of Helsinki. All included patient data were confidential.
Data Availability
The datasets generated and analyzed during the current study are not publicly available due to (ownership of data) but are available from the corresponding author on reasonable request.