
Abstract
Introduction
The natural progression of common pediatric otolaryngologic diseases can be difficult to assess. Children present and progress through the disease process as they grow—making it difficult to ascertain when to intervene. Additionally, the presence of communicable diseases can exacerbate or mask underlying illnesses. 1 The decision to intervene precludes an understanding of disease progression. Finally, the unethical nature of withholding pediatric treatment prevents a thorough understanding of the natural progress of childhood diseases.
The mandated COVID-19 shutdown created an opportunity to study the natural progression of several pediatric otolaryngologic diseases. 2 The prohibition of elective surgeries forced caregivers and healthcare providers to engage in watchful waiting and reassess the need for intervention. Further, mandated public health behaviors such as wearing masks and remote learning reduced the incidence of communicable diseases among children.3-5
Our study aims to determine if postponement of elective pediatric otorhinolaryngology surgeries results in a change in overall healthcare utilization and if there is any commensurate impact on disease progression. Through a prospective analysis of disease succession during the pandemic, we can highlight opportunities to revisit common treatment algorithms.
Patients & Methods
The study was approved by the Institutional Review Board of all three involved medical systems. Medical records were reviewed to identify patients whose previously scheduled pediatric otolaryngology surgeries between March 17, 2020 and April 14, 2020 were postponed or canceled due to the COVID-19 crisis at Children’s Healthcare of Atlanta (CHOA), Ann and Robert H. Lurie Children’s Hospital of Chicago (Lurie), and Texas Children’s Hospital (TCH). Demographic data collected includes age at COVID-19 shutdown (March 17, 2020), sex, ethnicity, race, preferred language, insurance, comorbidities, indication for elective surgery, number of ED visits, and any medication changes. Data at all three institutions was collected by August 2020. Of note, only medication changes for CHOA and Lurie were collected. Preferred language was categorized as English, Spanish, and other or unknown. Insurance was categorized as public, private, Tricare, unknown, and self-pay. Indications for surgery were grouped into ten categories: minor ear, major ear, airway, tonsil and/or adenoid (T&A), nasal cases, benign head and neck, cancer, urgent (lacerations and foreign body removal), and other.
Among CHOA and TCH’s patient cohort, caregivers were asked to complete a survey to assess decision-making on surgery rescheduling and additional services sought during the delay period. Parents who did not have adequate resources to complete the survey, had no email address on file, were unable to read and understand English and those who did not provide e-consent were excluded. Surveys reported information regarding caregiver decision-making, their child’s disease status, COVID-19 exposure, number of emergency room visits and if their child had any medication changes during the delay period.
Patients were grouped into those who rescheduled surgery (RS) and those who did not reschedule (NR). Any procedure not rescheduled by August 2020 after reopening was considered NR. Statistical analysis was completed using SPSS (Version 27.0, © IBM Corporation, Armonk, NY). Two sample t-tests were used to compare continuous data, such as age at COVID-shut down. Chi-squared analysis was performed to compare demographic and clinical characteristics between RS and NR patients. Fisher’s Exact Test was performed when more than 20% of expected cells had values <5. Multivariable logistic regression was performed to determine the effects of patient demographics on scheduling outcomes. Variables were considered for the regression models if they were associated with the outcome in the unadjusted univariable analysis with P-value of ≤.15. The conservative P-value allowed for reporting of possible trends and potential confounders that were marginally significant. All variables with P-value < .05 were considered statistically significant. Confidence Intervals (CI) were reported at 95% level.
Results
Demographic Data
Patient Demographics.
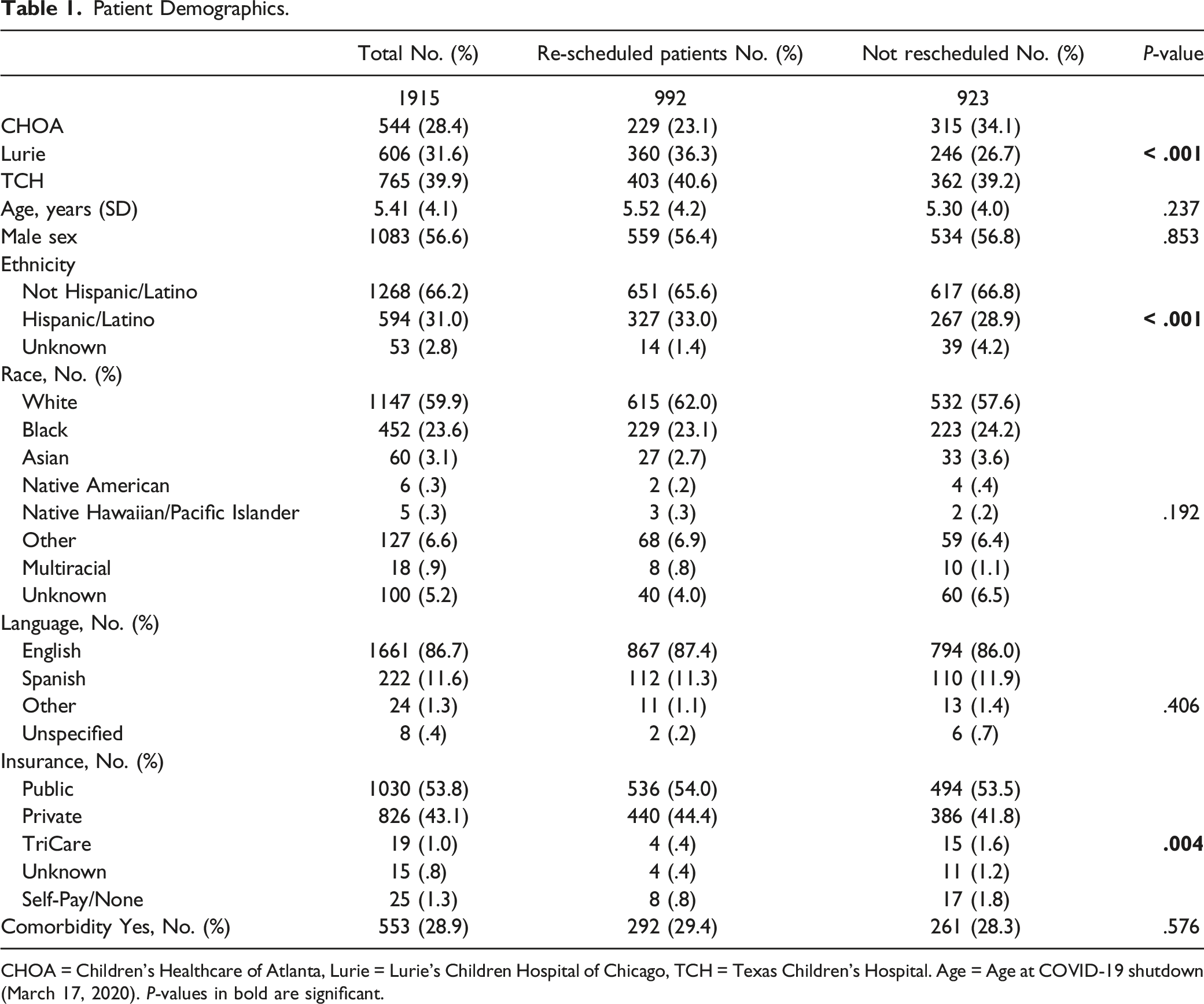
CHOA = Children’s Healthcare of Atlanta, Lurie = Lurie’s Children Hospital of Chicago, TCH = Texas Children’s Hospital. Age = Age at COVID-19 shutdown (March 17, 2020). P-values in bold are significant.
Surgery Indication
Surgery Indication by Institution.
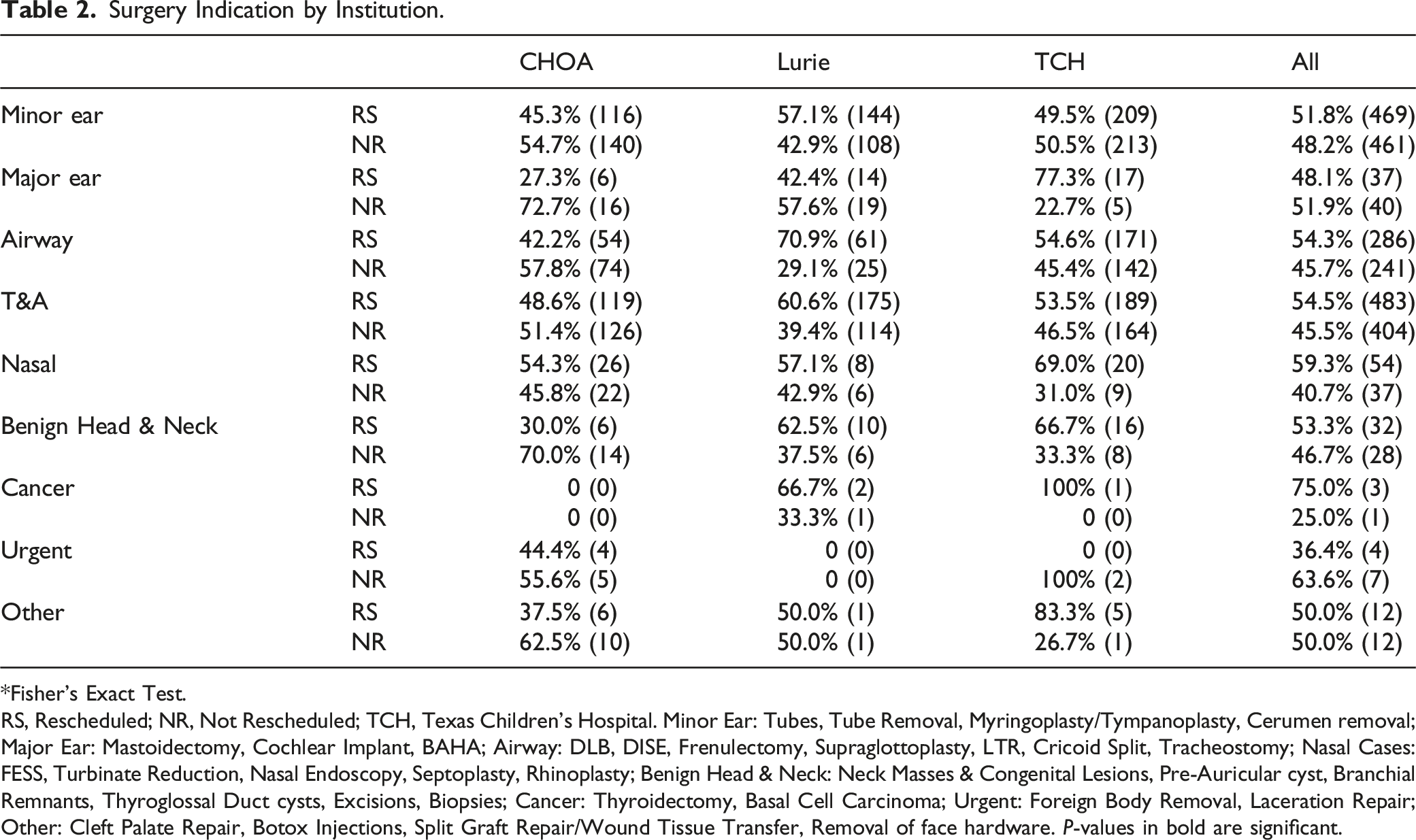
*Fisher’s Exact Test.
RS, Rescheduled; NR, Not Rescheduled; TCH, Texas Children’s Hospital. Minor Ear: Tubes, Tube Removal, Myringoplasty/Tympanoplasty, Cerumen removal; Major Ear: Mastoidectomy, Cochlear Implant, BAHA; Airway: DLB, DISE, Frenulectomy, Supraglottoplasty, LTR, Cricoid Split, Tracheostomy; Nasal Cases: FESS, Turbinate Reduction, Nasal Endoscopy, Septoplasty, Rhinoplasty; Benign Head & Neck: Neck Masses & Congenital Lesions, Pre-Auricular cyst, Branchial Remnants, Thyroglossal Duct cysts, Excisions, Biopsies; Cancer: Thyroidectomy, Basal Cell Carcinoma; Urgent: Foreign Body Removal, Laceration Repair; Other: Cleft Palate Repair, Botox Injections, Split Graft Repair/Wound Tissue Transfer, Removal of face hardware. P-values in bold are significant.
Comorbidities
Comorbidities.
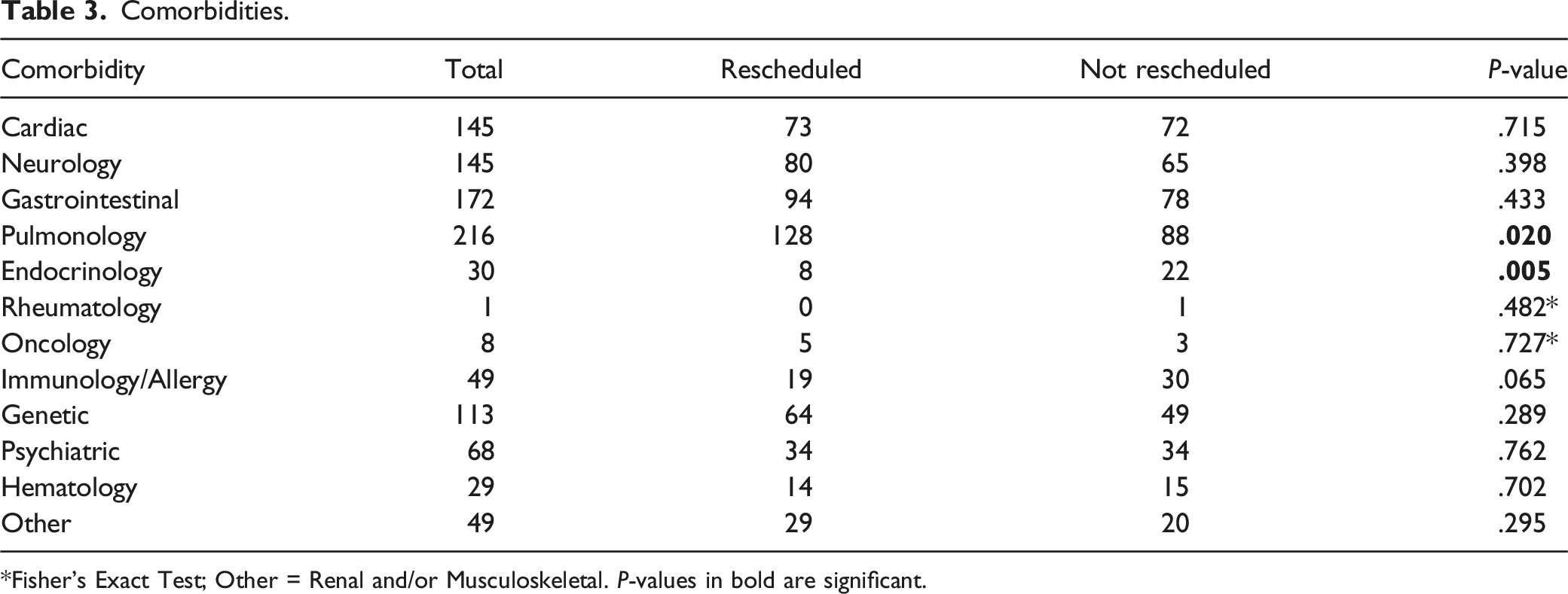
*Fisher’s Exact Test; Other = Renal and/or Musculoskeletal. P-values in bold are significant.
Survey Data
Reasons for Not Rescheduling Surgery vs Rescheduling Surgery*.
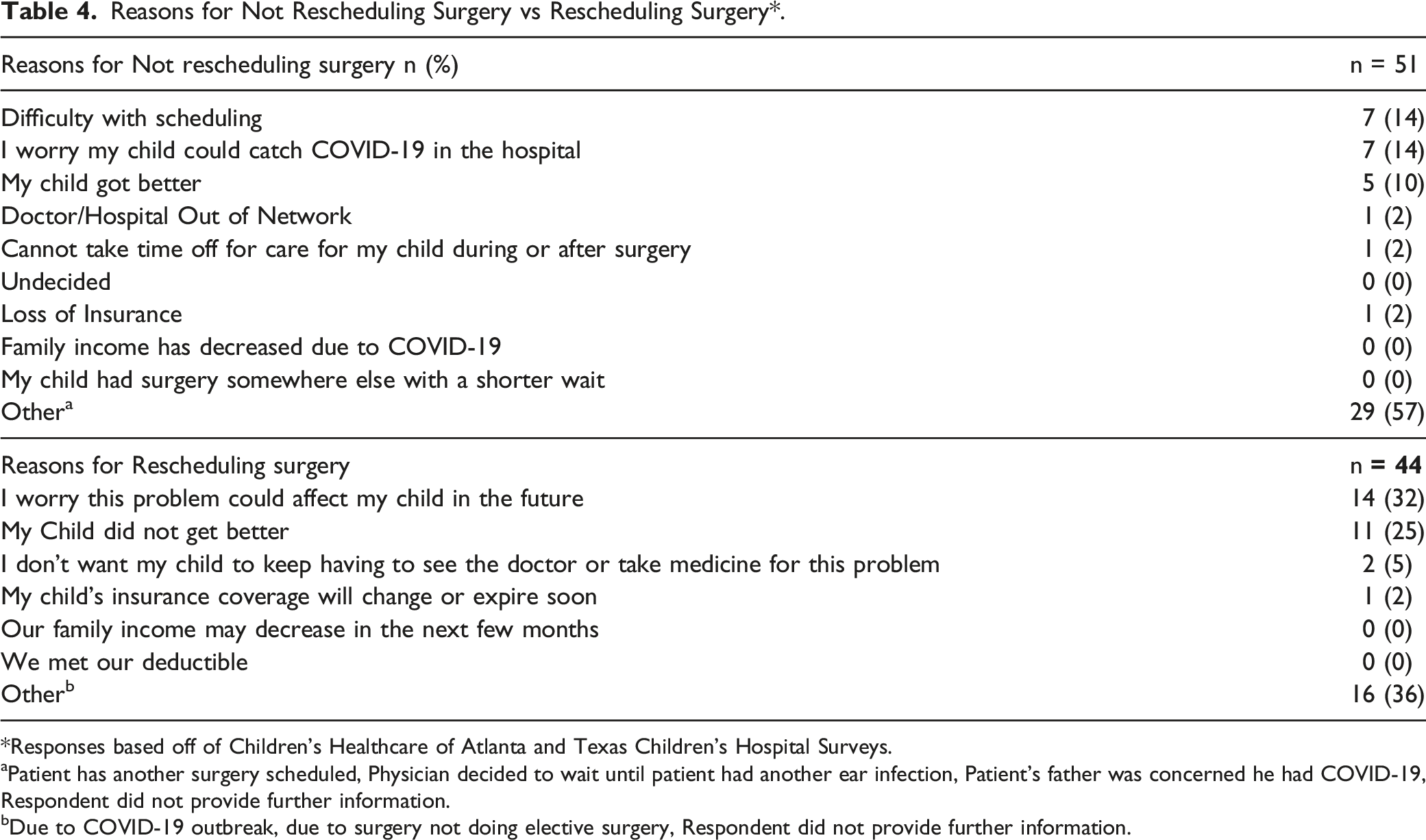
*Responses based off of Children’s Healthcare of Atlanta and Texas Children’s Hospital Surveys.
aPatient has another surgery scheduled, Physician decided to wait until patient had another ear infection, Patient’s father was concerned he had COVID-19, Respondent did not provide further information.
bDue to COVID-19 outbreak, due to surgery not doing elective surgery, Respondent did not provide further information.
Among the patients who rescheduled (n = 44), 32% (14) patients indicated that they worried their child’s condition could after their child’s future, 25% (11) indicated their child did not get better, and 36% (16) indicated “other.” Among those who chose, other, only 3 respondents provided additional details which included “due to the COVID-19 outbreak,” “due to surgery center not doing elective surgery,” and “protections are now very high for protection from Covid-19. I felt it was better to complete the surgery now than to wait when vigilance might become relaxed.”
ED Visits and Medication Alterations
Medication Changes and ED Visits*.

*Medication Change only reported for CHOA and Lurie.
Medication Change = Patient had at least one medication change, Emergency Room Visit = Patient had at least one Emergency Room Visit.
Discussion
The COVID-19 shutdown created a rare opportunity to study the natural progression of common pediatric otolaryngologic diseases without surgical intervention. Among our patient population, 48.2% (923) of caregivers did NR their child’s surgery (Table 1). Neither patient demographics nor surgical indication, excluding T&A, predicted scheduling outcomes (Tables 1 and 2). Further, the rate of emergency room visits and medication changes did not vary based on scheduling outcomes (Table 5). This suggests that conservative management for common pediatric otolaryngologic diseases may be effective for many conditions.
The reduction in human and environmental exposures during the shutdown may have played a significant role in the natural progression of common otolaryngologic diseases. In response to the pandemic, school attendance significantly decreased, with approximately 86% of pre-school aged children staying out of daycare.6,7 Upon reopening of childcare centers, COVID-19 safety precautions were implemented including child wellness checks, mask wearing, and an emphasis on hand hygiene.8,9 Consequently, there was a decrease in the spread of common communicable diseases, a trend that was even observed globally.10,11 Concurrently, there was a significant decrease in air pollution, a known trigger for pediatric asthma. 12 Given that nearly half of our patient cohort did NR, it is likely that the reduction in these exposures played a role. Thus, the development of treatment arms focused on mitigating pediatric triggers could be beneficial for the pediatric otolaryngologic patient population.
Our study also provides insight into how watchful waiting impacts pediatric otolaryngologic care. Tonsil and/or adenoid was associated with a higher likelihood of rescheduling (Table 2). This may be due to clinical research trials that have shown the benefit of early T&A compared to watchful waiting. 13 Minor ear surgeries were not associated with scheduling outcomes—a likely product of the heterogeneity in management of acute otitis media compared to chronic otitis media with effusion and recurrent acute otitis media14,15 as well as decreased exposure to viral causes of AOM during the pandemic. 16 Therefore, watchful waiting in conjunction with reducing viral exposure can be a management opportunity for AOM. Overall, the trends in surgery rescheduling serve as a powerful reminder that watchful waiting can be a safe alternative for our pediatric population and should not be overlooked.
In response to the pandemic, several surgical specialties revisited their treatment algorithms. 17 While the response was mixed, surgical subspecialties made substantial changes to their workflow to mitigate the growing backlog of cases. Some providers emphasized watchful waiting, 18 while others developed new surgical techniques. 19 Overall, the focus turned to reallocating resources and creating a safe environment for patients during the COVID-19 pandemic. Less attention has been given to revisiting management, including emphasis on preventive care. Our data suggest addressing external factors may help avoid the need for surgical intervention in many cases.
Limitations
Though our study included multiple institutions and has a large sample size, it is not without its limitations. Race and Ethnicity were self-reported and limited the analysis of these demographic variables. 50 (2.7%) and 92 (4.9%) caregivers did not identify their child’s race and ethnicity, respectively, among the total cohort. This study did not look at the completion rate of surgeries, which may be different than the number of cases rescheduled. The survey was not conducted at Lurie which study precludes further insight into caregiver decision making. Finally, we did not collect data on COVID-19 behaviors among the participants. Thus, it precludes us from directly measuring the impact of environmental triggers on disease progression.
Future Directions
As we continue to improve management of pediatric diseases it is to revisit current management algorithms. Further studies that elucidate preventable triggers and treatment modifications may help caregivers and practitioners to better manage common diseases. This simulated watch-and-wait situation for many pediatric otolaryngologic disease processes has also shed light on the multifactorial nature of surgical shared decision-making, which should be further explored in future studies.
Conclusions
The COVID-19 pandemic has resulted in cancellation of nearly 50% of pediatric otolaryngologic surgical cases. This study highlights the potential to revisit treatment algorithms for common pediatric otolaryngologic disease processes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.