
Abstract
A 53-year-old woman with a recurrent sore throat, xerostomia, nasal obstruction, and nasal discharge came to our hospital. At the first visit, she did not have a fever, but a blood test showed an intense inflammatory response. She had oral mucosal erosion. She developed dyspnea 2 months later. Nasendoscopy, laryngoscopy, and bronchoscopy showed upper and lower respiratory mucosa cobblestone appearance. Microscopy of the nasal and pharyngeal mucosa biopsy found regular mononuclear inflammatory cell dense submucosal infiltrate, mainly plasma cells. A mucous membrane plasmacytosis diagnosis was made. Prednisolone 1 mg/kg/day rapidly improved bronchial symptoms and cobblestone appearance.
Introduction
Mucous membrane plasmacytosis (MMP) is a rare mucositis variant represented by a polyclonal plasma cell infiltration of the tissue. The oral cavity, nasal mucosa, nasopharynx, larynx, oropharynx, hypopharynx, and esophagus of the upper aerodigestive mucosa can be affected by MMP. 1 We report an extremely rare case of MMP in a woman with a cobblestone appearance not only in the upper airway but also lower airway.
Case
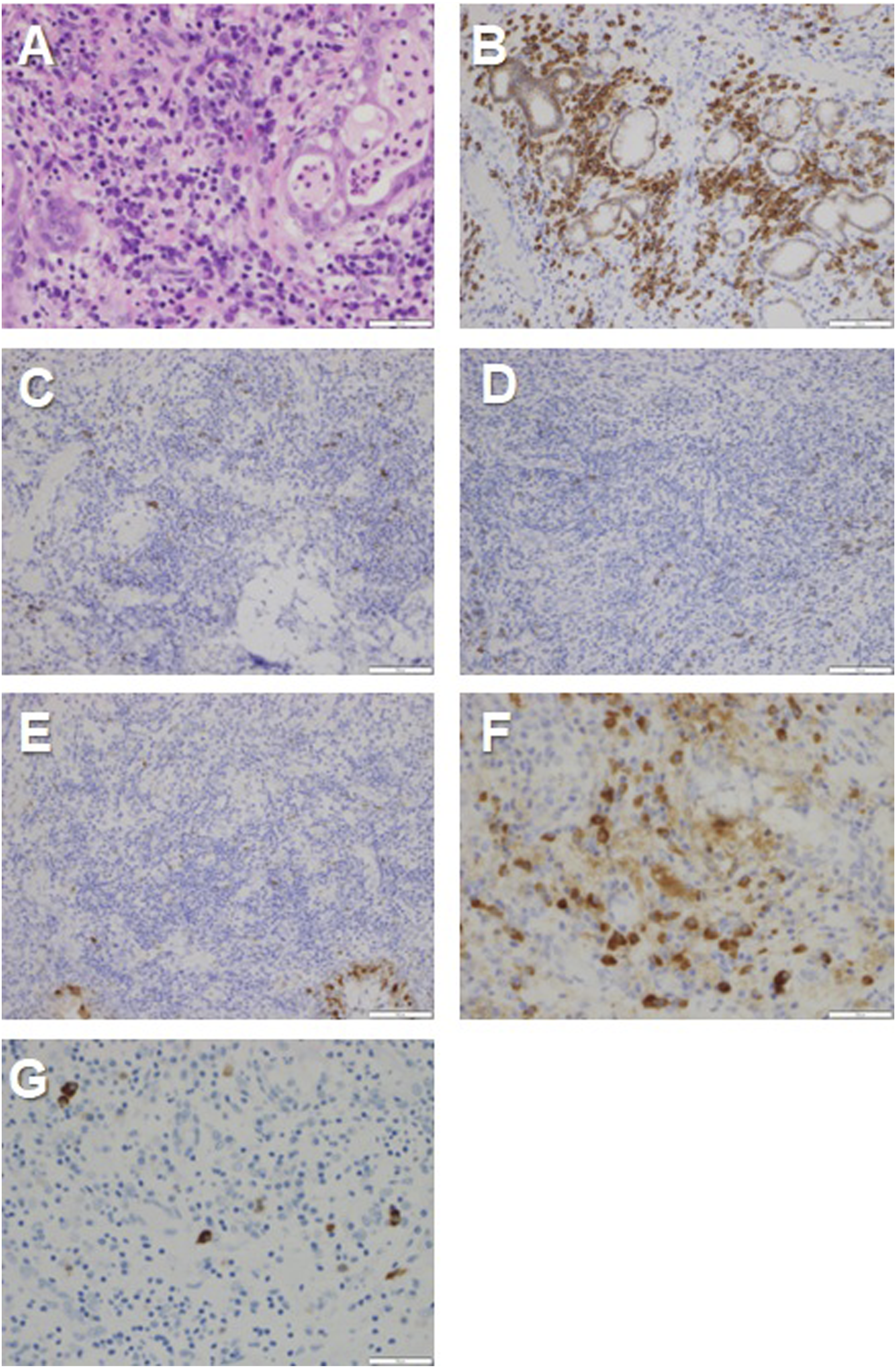
A 53-year-old woman with latent tuberculosis in childhood history came to our hospital with a recurrent sore throat, xerostomia, nasal obstruction, and nasal discharge. The patient was diagnosed with a viral pharyngeal ulcer and hospitalized in another hospital 1 month before her visit. Her symptoms improved after receiving intravenous hydrocortisone succinate sodium and she was discharged from the hospital. Her temperature was 36.4°C, blood pressure was 116/87 mmHg, pulse rate was 96/min, and SpO2:97% (room air) at the initial hospital visit. The oral cavity showed mucosal erythema and shallow soft palate ulceration. Nasendoscopy showed inflammatory nasal mucosa and purulent nasal discharge. Blood and biochemical examination revealed WBC 13,800/μl (87.2% neutrophils, 1.1% eosinophils, .1% basophils, 3.6% monocytes, and 8.0% lymphocytes), Hb 11.8 g/dL, Plt 30.6 × 104/μl, CRP 9.5 mg/dL, Cre .6 mg/dL, AMY 131 U/L PR3-ANCA negative, and MPO-ANCA negative. Levofloxacin 400 mg/day was administered for 1 week for rhinosinusitis. No improvement was observed 7 days later. Treatment was discontinued after ascertaining that infection was not the main pathology. Various autoantibody tests were negative, including Dsg1 and Dsg2. Mucositis symptoms in the oral cavity and nasal mucosa demonstrated a recurrent cycle of getting better and getting worse for 2 months. She then developed dyspnea. Nasendoscopy, laryngoscopy, and bronchoscopy showed an upper and lower respiratory mucosa cobblestone appearance (Figure 1). The auricle or external nose demonstrated no skin rash, vulvar ulceration, ocular symptoms, erythema, or swelling. An urgent bronchoscopic biopsy of the tracheal mucosa and endoscopic biopsies of the nasal mucosa, nasal septal cartilage, and nasopharyngeal mucosa were performed due to the rapid progression of inflammation in the airway. Nasal and tracheal mucosa biopsy specimens showed predominantly dense plasmacyte infiltrate in the subepithelial layer (Figure 2). Immunohistochemical studies showed that there were numerous CD138-positive plasmacytes in the subepithelial layer. These plasmacytes were negative for CD20, CD56, and Cyclin D1. No nuclear atypia or neoplastic change was seen in the plasmacytes. The IgG4-related lesion was also excluded (IgG4 positive cells were 4/HPF. IgG4/IgG = .09). There was a mild degree of neutrophilic infiltrate in the epithelium’s surface lining. There was no inflammatory cell infiltrate in the nasal septal cartilage. MMP was the final pathological diagnosis. Her symptoms and mucosal lesions rapidly progressed. She was treated with oral prednisolone 1 mg/kg/day as soon as possible due to the high risk of a fatal condition. The prominent lesions on the upper and lower airway mucosa improved after 1 week of treatment. Nasendoscopy, laryngoscopy, and bronchoscopy findings. A. Nasal cavity B. Nasopharynx C. Pharynx and larynx D. Trachea. The cobblestone appearance of the upper and lower airway mucosa appeared after 2 months of oral mucositis. Pathological findings. A. HE section (×400). Dense lymphoplasmacytes infiltrate (predominantly plasmacytic) in the subepithelial layer. A mild degree of neutrophilic infiltrate was seen in the epithelium and mucous glands. B. CD138 (×200). Strongly positive for plasmacytes around the mucous glands in the subepithelial layer. C, D, and E. CD56, CD20, and Cyclin D1 (×200) negative. F. IgG stain (×400). 56 positive cells/HPF. G. IgG4 stain (×400). 4 positive cells/HPF, IgG4/IgG: 7%. The bar indicates 200 μm.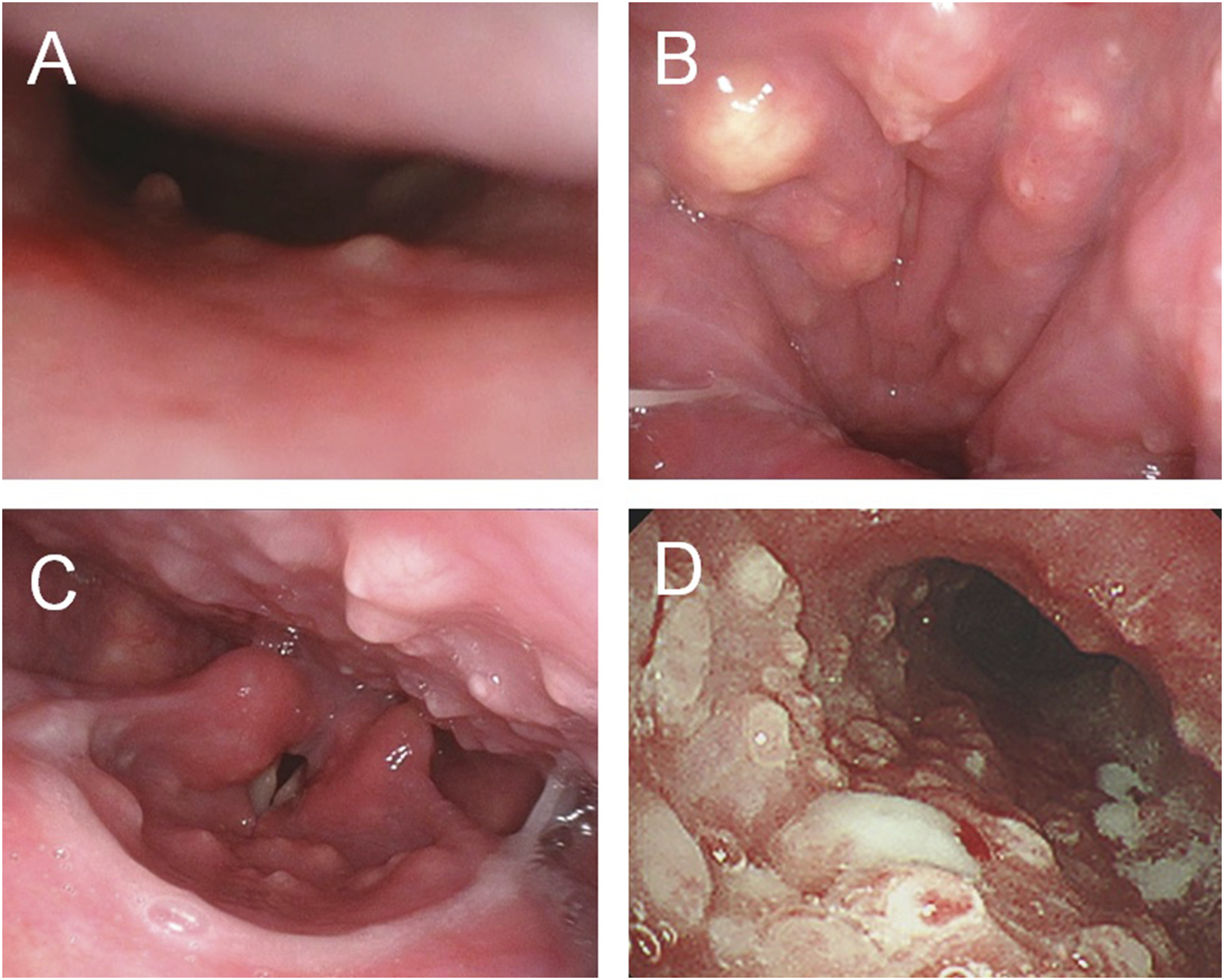
Discussion
Mucous membrane plasmacytosis is a benign polyclonal plasma cell proliferative disorder of the mucous membranes with an unknown etiology first described by Zoon in 1952. This was termed a “chronic benign balanoposthitis with plasmacytes.” 2 Several terminologies were introduced, including plasmacytosis circumficialis, plasmacytosis mucosae, plasma cell orificial and plasma cell mucositis, and MMP with no existing consensus. 3 The oral cavity, nasal mucosa, nasopharynx, larynx, oropharynx, hypopharynx, and esophagus of the upper aerodigestive mucosa can be affected by MMP. 1 Flexible laryngoscopy typically finds cobblestone mucosal appearance.1,4 This case reported a cobblestone appearance in the upper aerodigestive mucosa, as well as the trachea, which is an extremely rare case. Cobblestone appearance indicates severe inflammatory cell accumulation, which was also found in the nasal and trachea mucosa with recurrent cartilitis. 5 There were no inflammatory cells in the nasal cartilage in this case. The main histological MMP features show a dense plasma cell infiltration without cellular atypia in the submucosa. Moreover, one of the most diagnostic MMP points to note is the need to exclude plasma cell neoplasm and lymphomas. 6 In this case, immunohistochemistry studies showed that the plasma cells were CD138 plasma cells, but were negative for CD20, CD56, and Cyclin D1.
Mucous membrane plasmacytosis causes airway obstruction that requires tracheostomy when the disease progresses. 1 If the lesion progresses into the trachea, this will result in airway obstruction, which is a severe condition. Topical and systemic steroids are often used for MMP, although optimal treatment and prognosis remain undetermined for MMP. Immunosuppressive agents have been used with varying success. 7 There have been cases of recurrence after 15 years, so long-term follow-up is necessary even if the disease seems to have gone into remission. 3 Physicians must recognize MMP when a cobblestone appearance in the upper airway is observed. It should be noted that the lower respiratory mucosa may also be compromised.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by the Japan Society for the Promotion of Science KAKENHI (grant no: 20K18323 and 18K16857).
Ethical Approval
Ethical approval to report this case was obtained from Research Ethics Committee Faculty of Medicine, Juntendo University
Human and Animal Rights
All procedures in this study were conducted in accordance with the Research Ethics Committee Faculty of Medicine, Juntendo University.
Informed Consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.