
Abstract
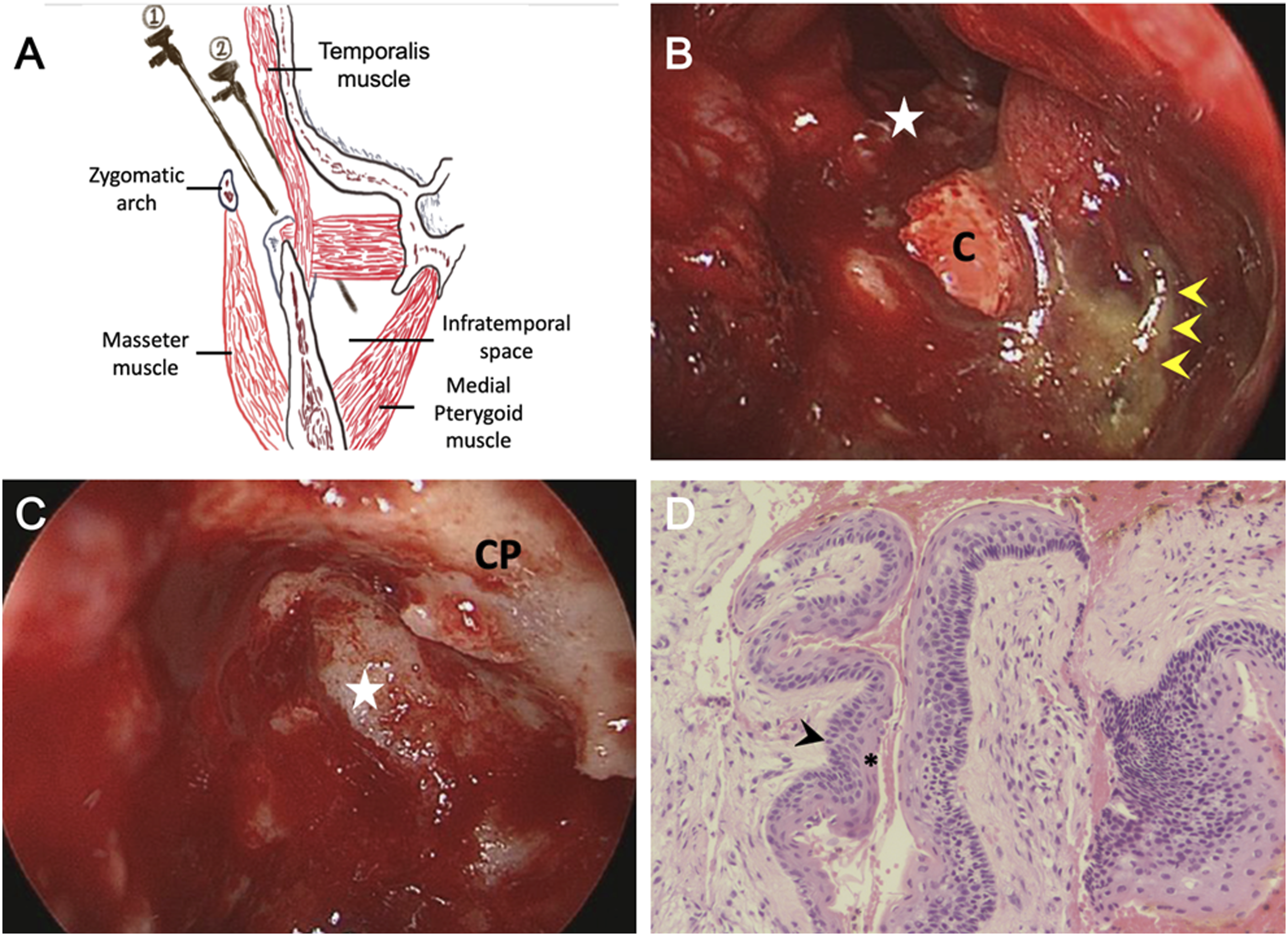
A 67-year-old otherwise healthy man visited our clinic with a 3-day history of a persistent, painful swelling in the right temporal region. He stated that the swelling had occurred regularly approximately once every 6 months over the past decade; however, it had regressed in a few days each time. However, in the last year, the temporal swelling had become aggravated and occurred more frequently. He had no febrile episodes, facial sensory loss, or orbital disorders. Physical examination revealed asymmetric face and trismus associated with a firm induration over the temporal and cheek regions. Laboratory tests revealed an elevated white blood cell count >14300 mm3 and elevated C-reactive protein levels of 11.69 mg/dL. Computed tomography (CT) (Figure 1A) with three-dimensional reconstruction (Figure 1B) of the head was performed, which demonstrated osteolytic lesions within the right mandible. The patient’s clinical condition improved after 7 days of empirical treatment with intravenous amoxicillin/sulbactam. However, subsequent magnetic resonance imaging (MRI) (Figures 1C and 1D) revealed persistent lesions. We subsequently scheduled an endoscopy-assisted surgery via a pre-auricular incision to approach the lesion. After reflecting the deep temporal fascia to protect the identified facial nerve branches following partial parotidectomy, we created surgical corridors through the planes of the zygoma and pterygoid muscles to access the mandible and infratemporal fossa by blunt dissection (Figure 2A). The endoscopic approach facilitated enucleation and curettage of the bony lesions (Figures 2B and 2C). Histopathological analysis of the specimens (Figure 2D) confirmed the diagnosis of a keratocystic odontogenic tumor. The patient had an uneventful postoperative course without evidence of recurrence in the 2-year follow-up. Computed tomography (CT) and magnetic resonance imaging (MRI) of the head and neck region. Axial image (A) and three-dimensional reconstruction (B) of the head and neck CT showing separate lesions (arrowhead) located within the right mandibular coronoid process and condyle. MRI (C and D) revealing additional soft tissue lesions adjacent to the condyle (arrow). The intra-osseous lesions (arrowhead) in the post-contrast T1-weighted sequence (C) demonstrate heterogeneous enhancement with a signal slightly higher than that of the medial pterygoid muscle on the contralateral side. The coronal T2-weighted sequence (D) shows distinct signal intensities of intra-osseous (arrowhead) and extraosseous (arrow) lesions. The surgery scheme, intraoperative view, and pathologic findings. (A) Schematic drawing of our surgical approach. The deep temporal fascia was released from its attachment to protect the upper branches of the facial nerve following partial parotidectomy. A 4-mm endoscope was docked between the zygoma and medial pterygoid muscle to approach the mandible (route 1) and infratemporal fossa (ITF) (route 2). (B) The endoscopic findings demonstrate the coronoid process lesion containing yellowish materials (arrowheads) that had perforated into the ITF (star). (C) Findings of the condylar KCOT after endoscopic enucleation and bony curettage (star). (D) The pathologic analysis of retrieved specimens (hematoxylin-eosin, original magnification ×200) revealing corrugated parakeratin layers (asterisk) and palisading basal cells with hyperchromatic nuclei (arrowhead). (C, coronoid process; CP, condyloid process; KCOT, keratocystic odontogenic tumor).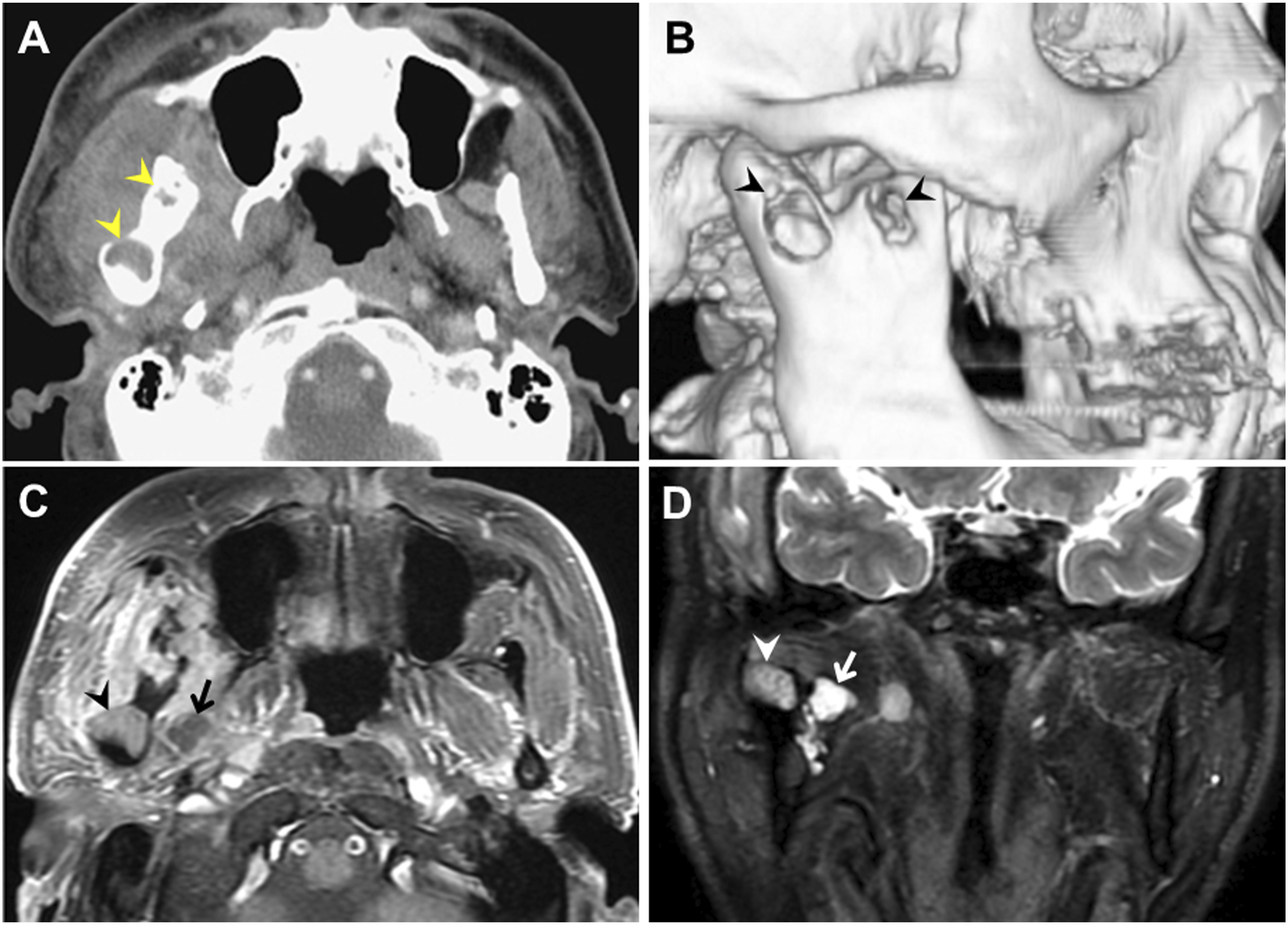
Keratocystic odontogenic tumors (KCOTs) are odontogenic neoplastic diseases derived from the remnants of the dental lamina. 1 They generally occur sporadically, with male patients in their 20s and 30s being most commonly affected. These neoplasms generally present as an asymptomatic multilocular intra-osseous lesion in the posterior mandible. 1 Typically, KCOTs are diagnosed incidentally as isolated lesions, and their presentation in the form of multiple lesions with simultaneous inflammation is rarely observed. 1
The typical findings of KCOTs in CT scans are well-circumscribed, radiolucent lesions with scalloped margins. 2 The MRI features of KCOTs include intermediate to high heterogeneous signal intensities in both T1- and T2-weighted sequences and a uniform slightly enhanced rim corresponding to the cystic wall after contrast administration. 3 However, CT is usually equivocal in discriminating KCOT from other common lesions, especially dentigerous cysts and ameloblastoma. 2 MRI may help in differentiating KCOTs from ameloblastoma because their apparent diffusion coefficient values of unenhanced areas and signal intensity uniformity of cystic components are different. 3 As there are limitations in distinguishing KCOT from other odontogenic tumors using these diagnostic criteria, the definite diagnosis relies on pathologic analysis.2,3
However, the optimal management strategy for KCOTs remains debatable. Radical resection of the region is currently the standard treatment due to its high cure rate; however, it can lead to substantial surgical morbidity. 4 Complete enucleation followed by adjuvant bony curettage or peripheral ostectomy 4 has gradually become one of the optimal treatments because the adjuvant bony management may significantly reduce the recurrence rate by removal of the microscopic remnants compared with enucleation alone. Additional benefits of complete enucleation with adjuvant bony management are that the procedure is less invasive and preserves more anatomical structures than the standard radical resection. 5 Nevertheless, the outcomes of these procedures in treating multilocular lesions within the mandibular ramus are unsatisfactory as the difficult-to-reach anatomic position may significantly limit the visualization of the surgical field. 5
The employment of the endoscopic technique in mandibular disorders was first described in the late 90’s, 6 and a recent review has described endoscopic surgery as an effective and safe procedure for repairing mandibular fractures because it provides comparable outcomes to that of the open approaches but with fewer permanent nerve injuries. 6 Similarly, endoscopic surgery may be advantageous for treating mandibular tumors/cysts as endoscopes may provide a better visualization to facilitate the removal of hidden epithelial layers.6,7 A recent investigation on 57 mandibular odontogenic cysts demonstrated that endoscopic enucleation was associated with lower recurrence rates and fewer permanent mandibular nerve injuries than those of the surgeries performed using the traditional approach. 7 Another outcome analysis reporting 32 cases of KCOTs demonstrated similar results, suggesting endoscopy-assisted enucleation as an effective strategy to manage KCOTs. 8
We reported this case of multiple mandibular KCOTs perforating into the surrounding soft tissues to remind clinicians to consider this diagnosis in patients with recurrent hemifacial swellings. Additionally, we provide an encouraging experience with endoscopic surgery in managing KCOTs located within the mandibular condyle and coronoid process. Nevertheless, vigilant follow-up is required to detect new lesions or early recurrence, especially 5 years from the time of initial treatment.
Footnotes
Author’s Note
This manuscript is original and it, or any part of it, has not been previously published; nor is it under consideration for publication elsewhere.
Authors’ Contributions
Y-HL had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Concept and design: Y-CC, Y-HL.
Acquisition, analysis, or interpretation of data: Y-CC, P-HL, Y-LS, Y-FY, Y-HL.
Drafting the manuscript: Y-CC, Y-HL.
Critical revision of the manuscript for important intellectual content: Y-CC, Y-HL.
Final approval: Y-CC, P-HL, Y-LS, Y-FY, Y-HL
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Yen Tjing Ling Medical Foundation (CI-111-26).