
Abstract
On a perilymphatic fistula, there is an extravasation of the perilymph fluid into the middle ear cavity. Cross-sectional imaging techniques have very important role in evaluation of inner and middle ear structures and temporal bone. While thin section CT scans can show successfully pneumolabyrinth and temporal bone fracture, high-resolution 3D volumetric MRI sequences can help to demonstrate posttraumatic ear effusion and cerebrospinal fluid fistula into inner ear or middle ear.
Introduction
On a perilymphatic fistula, there is an extravasation of the perilymph fluid into the middle ear cavity secondary to an abnormal connection between middle ear or mastoid cells and inner ear. As a result of this connection, air leak into the inner ear cavity, known as pneumolabyrinth, is an expected finding. This rare entity frequently develops secondary to blunt or penetrating trauma. Accepted other etiologic factors include cholesteatoma, surgical injury, inflammatory processes, and barotrauma.1-3 Typical clinic symptoms include sensorineural hearing loss (fluctuating or stable), tinnitus, vertigo, disequilibrium, aural fullness, and headache.1,4
Diagnosis of perilymphatic fistula is based on clinical history, physical examination, audiometry, radiologic findings, and fistula test. 5 Cross-sectional imaging techniques such as computed tomography (CT) and magnetic resonance imaging (MRI) have very important role in evaluation of inner and middle ear structures and temporal bone, and for etiology of sensorineural hearing loss. 6 CT and MRI scans help also for demonstration other abnormalities associated with perilymphatic fistula. Fracture of temporal bone and pneumolabyrinth can be demonstrated successfully by thin section CT scans with bone algorithm. MRI can reveal posttraumatic ear effusion and cerebrospinal fluid fistula into inner ear or middle ear.
A fistula between the cerebrospinal fluid and perilymphatic space in patients with pneumolabyrinth is a very rare condition. We herein reported thin section CT scan findings of a patient with sensorineural hearing loss secondary to left temporal bone fracture. We also demonstrated 3D volumetric thin slice T2-weighted non–contrast MR cisternography features of a fistula between cerebrospinal fluid and perilymphatic space.
Case Presentation
A 49-year-old male was admitted to our clinic suffering from severe headache, dizziness, vertigo, and left-sided hearing loss. His complaints occurred immediately after a temporal injury following traffic accident. On physical examination, he had left-sided nystagmus. Examination of the external ear was normal. Audiologic examination showed a left-sided sensorineural hearing loss.
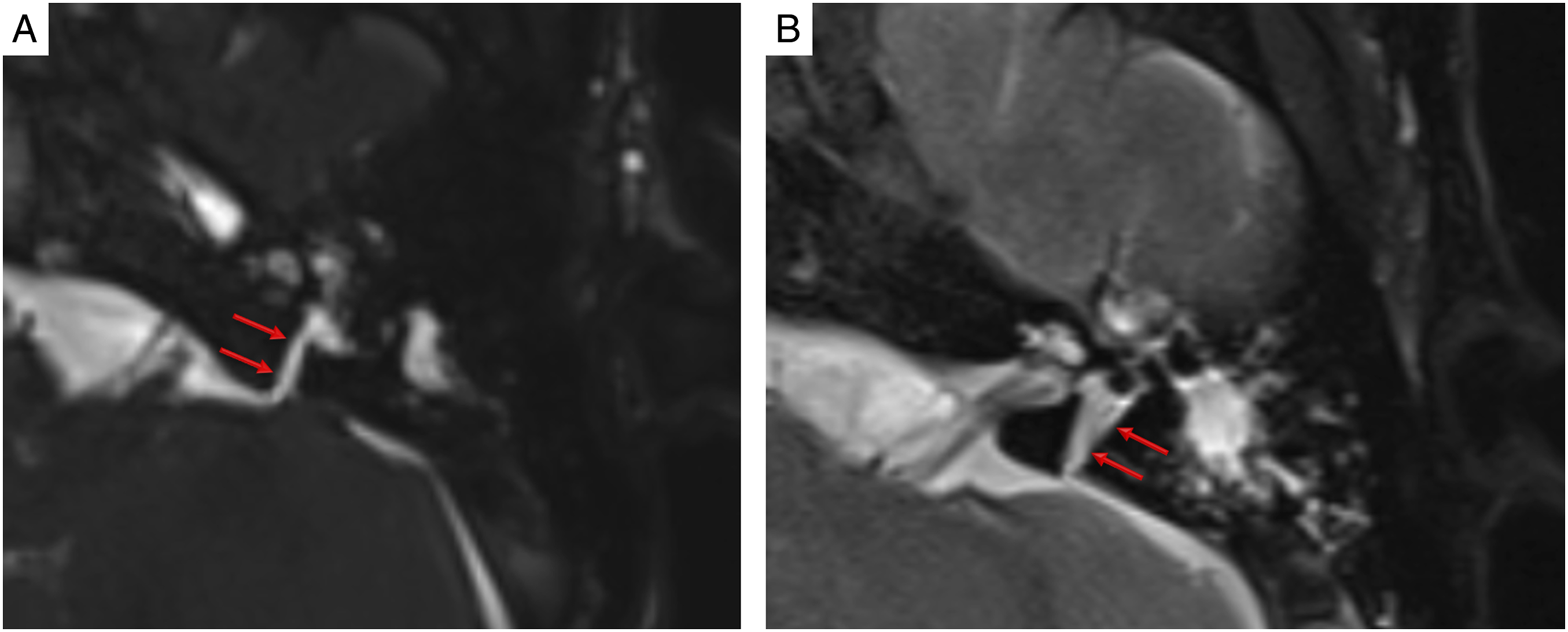
High-resolution temporal bone CT scan revealed a linear fracture extending the otic capsule in the left temporal bone (Figure 1). There was hemorrhagic effusion in the mastoid cells and middle ear cavity. CT scan revealed no disorder of the middle ear ossicle chain. As the very important sign of perilymphatic fistula, high-resolution CT scan revealed multiple air densities compatible with pneumolabyrinth in the left cochlea, vestibule, and semicircular canals (Figure 1(a) and (b)). For evaluation inner ear structures and their associations with cerebrospinal fluid, non–contrast high-resolution MRI cisternography was performed. Thin section volumetric T2-weighted non–contrast MRI cisternography sequences demonstrated clearly a fistula tract between the cerebrospinal fluid and perilymphatic fluid (Figure 2(a) and (b)). Axial (a) and coronal (b) high-resolution temporal bone CT scans show transverse fracture (red arrows) extending the otic capsule in left temporal bone and hemorrhagic effusion (asterisk) in the mastoid cells and middle ear cavity. CT scans also reveal air densities (yellow arrows) compatible with pneumolabyrinth in the left cochlea, vestibule, and semicircular canals. 3D heavy constructive interference in steady state (a) and thin section turbo spin echo (b) T2-weighted sequences demonstrate a fistula tract (red arrows) between the cerebrospinal fluid and perilymphatic fluid.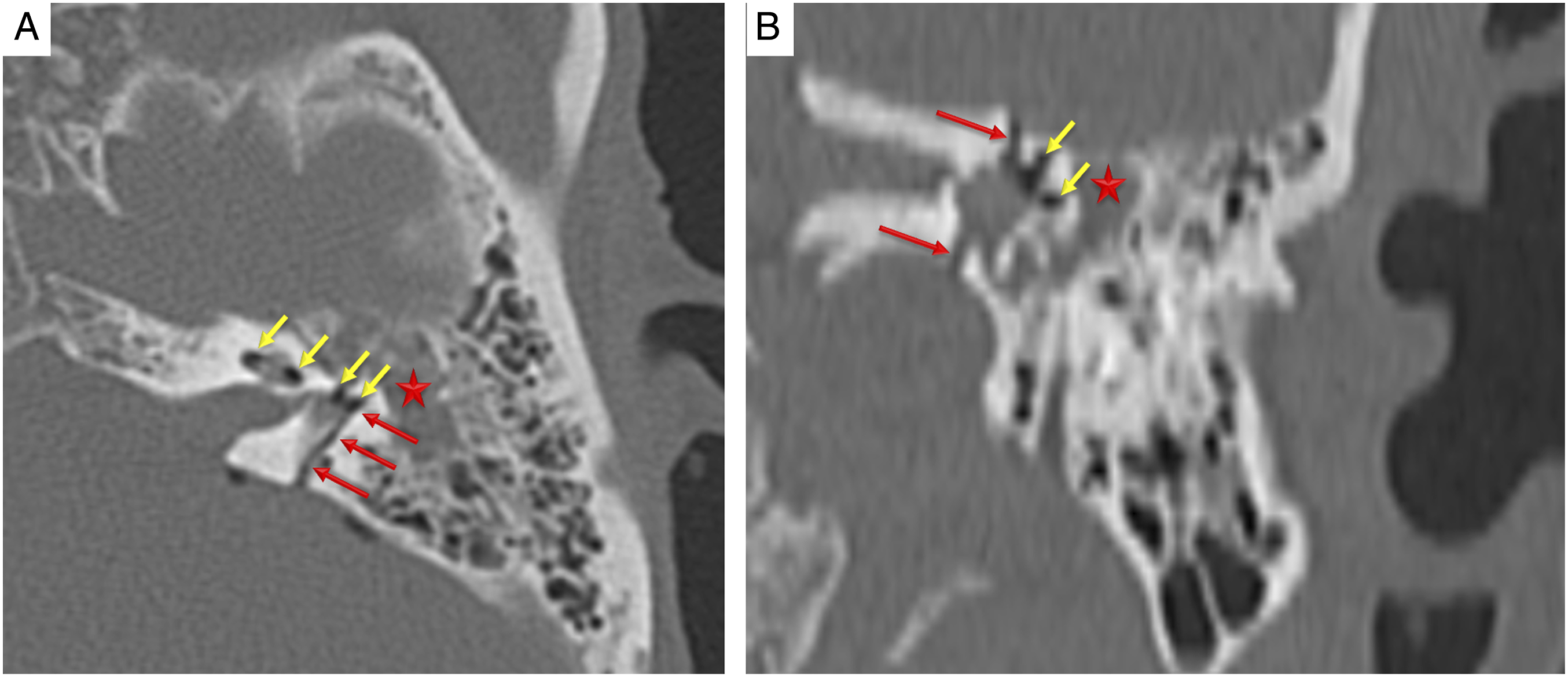
Exploratory tympanotomy was performed 1 week after trauma. A perilymphatic fistula was detected in the surgical operation. The defective area was sealed.
Conclusion
Routine MRI sequences including T2-weighted and non-contrast T1-weighted are the preferred method to investigate the inner ear structures in posttraumatic patients. Vestibulocochlear nerve integrity, membranous labyrinth pathologies, and volumes of the utricle and saccule are commonly evaluated by conventional MRI sequences. The use of 3D heavy T2 sequences (turbo spin echo and constructive interference in steady state) produces thinner image slices with the submilimetric thickness, which enhances effectiveness of the imaging. Multiplanar reconstruction and volume rendering images also provides fine contrast between the perilymphatic space and surrounding anatomical structures.
The inner ear organs and perilymphatic space in posttraumatic patients should be carefully evaluated with high-resolution 3D volumetric MRI techniques. In case of a suspicion of a perilymphatic fistula, high-resolution 3D volumetric heavy T2 sequences without intrathecal contrast infusion in especially 3T can help demonstrate the fistula tract.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Significance Statement
On a perilymphatic fistula, there is an extravasation of the perilymph fluid into the middle ear cavity. Cross-sectional imaging techniques have very important role in evaluation of inner and middle ear structures and temporal bone. While thin section CT scans can show successfully pneumolabyrinth and temporal bone fracture, high-resolution 3D volumetric MRI sequences can help to demonstrate posttraumatic ear effusion and cerebrospinal fluid fistula into inner ear or middle ear.