
Abstract
Paradoxical vocal fold motion disorder (PVFMD) is a condition involving the inappropriate narrowing of the larynx with symptoms of laryngeal tightness and dyspnea. A 23-year-old woman was diagnosed with PVFMD by imaging, revealing dynamically constricted, supraglottic tissue, an abnormal adduction of the vocal cords with a characteristic “posterior chink” observed. After diagnosis, laryngeal control retraining protocols and biofeedback therapy were initiated. To treat persistent symptoms, interventions such as vocal fold botulinum toxin (BoNT) injections were performed with slight improvements. Ultimately, psychiatry performed 10 repetitive transcranial magnetic stimulations (rTMS) with a right‐sided, low‐frequency approach to treat the patient’s underlying major depressive disorder and comorbid anxious distress. Afterward, the patient’s symptoms were successfully reduced with an improvement in Dyspnea Severity Index. Although most patients with PVFMD were relieved with laryngeal control therapy, some are refractory and lack the literature on the best treatment. In this case, we followed the multidisciplinary approach and individualized our novel therapeutic strategies including especially rTMS, which successfully reduced symptoms. This is the first reported case of refractory PVFMD to be treated with novel interventions, and rTMS might play a role in PVFMD mitigation.
Introduction
Paradoxical vocal fold motion disorder (PVFMD) was first described in 1842 and previously called Munchausen’s stridor. 1 As the availability of laryngoscopy expanded, PVFMD was increasingly reported in the 1970s and understood to be a functional disorder without a structural or innervation cause. The 2013 international consensus conference nomenclature defined the term inducible laryngeal obstruction to describe a narrowing of the vocal folds at the supraglottic level in response to triggers, 2 including exercise, irritants, stress, and otherwise idiopathic without known inciting agent. Symptomatic episode intensity can be acute and variable. Patients describe a laryngeal tightness or strangulation associated with cough, stridor, or dyspnea. The preferred treatment strategy has been a multidisciplinary approach to minimize laryngeal irritation. 3 However, even after traditional therapy, some patients have persistent dyspnea symptoms of refractory PVFMD. Here, we present a case of refractory PVFMD treated with novel strategies that successfully reduced symptoms.
Case Report
A 23-year-old woman presented to the emergency department with desaturation, stridor, barking cough, and a skin rash on the extremities. The tentative impression of anaphylaxis with bronchospasm and she was admitted for evaluation. During her hospitalization, inspiratory stridor occurred twice a day, occasionally with desaturation. For suspected asthma exacerbation, we administered medication with limited effect. Additionally, a pulmonary function test showed no obstructive disease, and imaging of the neck, chest, and brain showed no notable findings. Based upon the clinical presentation, PVFMD was considered and a laryngoscopy was performed, during a symptomatic episode. Diagnostic imaging revealed dynamically constricted, supraglottic tissue and an abnormal adduction of the vocal cords with a characteristic “posterior chink”. (Figure 1) Under the working diagnosis of PVFMD, laryngeal control therapy and respiratory retraining were initiated with a speech language pathologist. Biofeedback therapy was performed using visualization of the larynx via video laryngoscopy. During acute attacks of dyspnea, we guided the patient using respiratory therapies, including pursed lips, sniffing breathing, jaw thrusts, reassurance, and verbal confirmation of normal saturation. Positive pressure support was applied if the other techniques were ineffective. Due to the persistent symptoms over one month, we administered 3, bilateral, vocal fold botulinum toxin (BoNT) injections with the dose increasing from 2.5 units to 10 units. Afterward, a slight improvement (32 to 26 points) was noted on the Dyspnea Severity Index (DSI). After all traditional therapies had been exhausted, symptom attacks and occasional respiratory distress remained persistent, so a tracheostomy was considered. First, psychiatry was consulted and an adjustment disorder with anxious mood was diagnosed. To treat the comorbid anxious mood, repetitive transcranial magnetic stimulation (rTMS) using a right‐sided, low‐frequency approach was performed 10 times over 2 weeks. During the rTMS program, a decreased frequency of PVFMD was noted. Ultimately, the symptoms were successfully reduced with DSI improved to 18 points. Thus, this case demonstrates the efficacy of rTMS, which may play a role in the mitigation of PVFMD. PVFMD with characteristic “posterior chink” observed through laryngoscope during some symptomatic inspiration.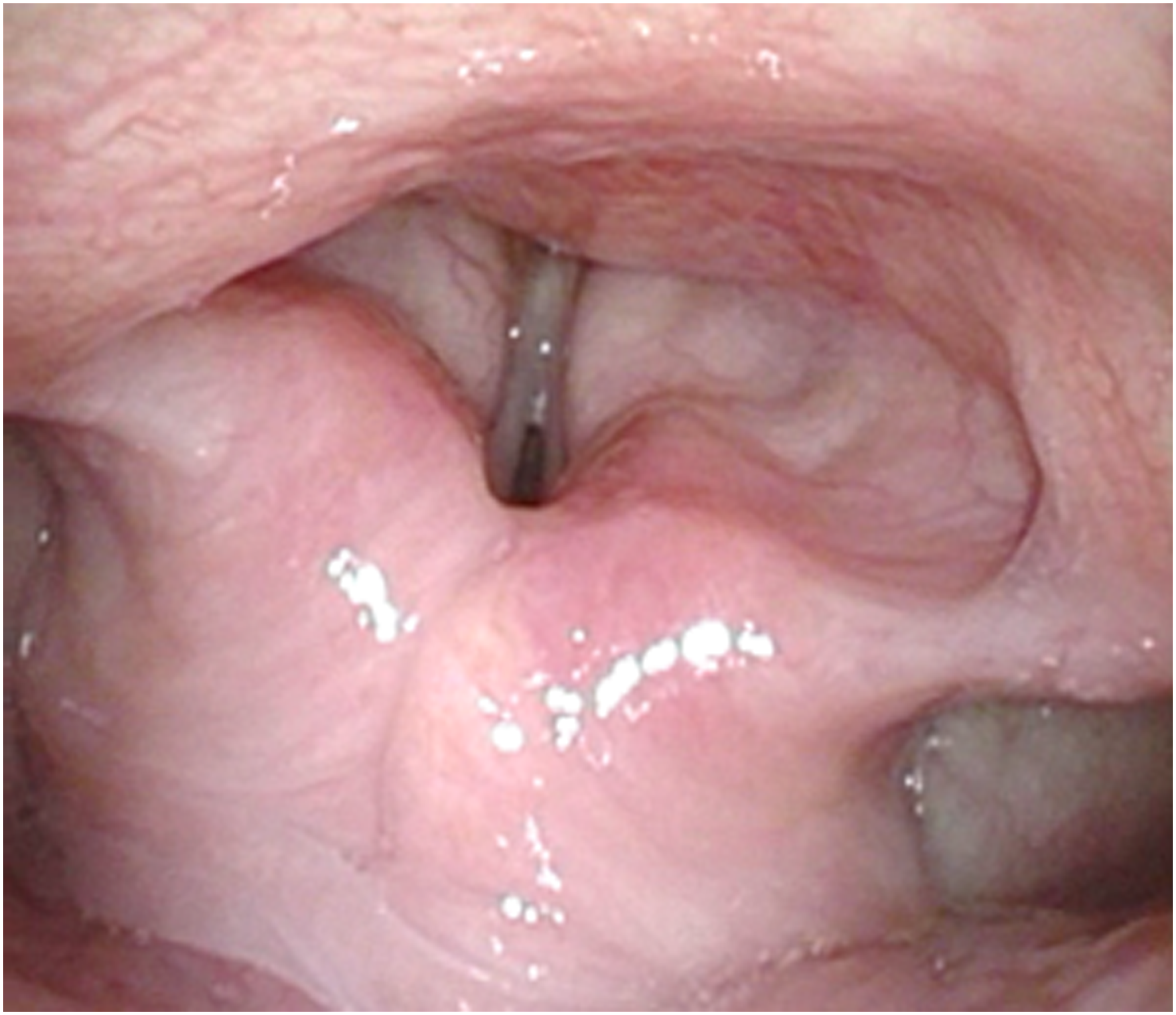
Discussion
Patients with severe symptoms of episodic PVFMD are often sent to the ER in respiratory distress where they receive bronchodilators, steroids, sedatives, or airway interventions. These patients may be misdiagnosed with asthma, undergoing various medication trials. Studies have shown that the median time to PVFMD diagnosis is 4.5 years.4,5 Therefore, accurate, timely diagnosis is the key to avoid unnecessary treatments and reduce healthcare utilization. PVFMD diagnosis is confirmed by visualizing an abnormal adduction of the vocal folds through laryngoscopy, during a symptomatic episode. The glottic aperture may be obliterated during inspiration, except for a posterior, diamond-shaped passage. There are no previous studies that have elucidated this characteristic posterior chink. We hypothesize that it may be caused by the intrinsic laryngeal muscles, including the posterior cricoarytenoid muscles (vocal fold abductors), that simultaneously spasm, while other muscles narrow the laryngeal inlet. Confirmation of this symptomatic mechanism by electromyography is needed , yet would be difficult and risky.
Various treatment strategies are used for PVFMD. However, the standard treatments are empiric, not evidence-based. The multidisciplinary approach of integrated and individualized services, including behavioral therapy, to treat PVFMD patients is considered the mainstay in a nonacute setting. 3 During an acute exacerbation, therapeutic respiratory techniques (pursed lip, sniffing breathing, and jaw thrust) are used to interrupt irregular spasm and allow familiar neurologic signals to re-engage the vocal folds. 4 For persistent symptoms, patients may undergo biofeedback therapy. If other therapies fail, BoNT injection is indicated for refractory PVFMD. 6
BoNT injections have demonstrated effectiveness in the treatment of various laryngeal disorders. 7 In our case, we had exhausted therapeutic breathing techniques and biofeedback sessions in treating the refractory PVFMD. Therefore, we performed 3 BoNT injections, using an initial dose of 2.5 units to the bilateral vocal cords, followed by a repeat injection 2 weeks later. The patient had improved but had recurrent symptoms. Therefore, she received a third injection one month later; a higher dose of 5 units on the left side and 10 units on the right side. The dosage was adjusted according to the degree and duration of improvement. We believe that the different doses on each side provided a new baseline for breathing and vocal cord movement that might facilitate future laryngeal control techniques.
Repetitive transcranial magnetic stimulations, a non-invasive procedure, has been investigated in patients with different medical conditions. By applying electromagnetic pulses to superficial brain regions, the underlying neurons depolarize and modulate activity in cortical regions. The therapeutic efficacy of rTMS has been shown for anxiety symptoms of depression and there is support for the relative efficacy of 3 commonly used, stimulation protocols: left-sided high-frequency, right-sided low-frequency, and sequential bilateral. 8 We performed rTMS 10 times using a right‐sided low‐frequency approach to treat the underlying anxiety. The PVFMD improved dramatically with decreasing durations of the symptomatic episodes. However, the patient may have experienced placebo effect for all of the therapeutic strategies we performed.
Conclusions
Although laryngeal control therapy relieves symptoms in most patients with PVFMD, some patients have refractory symptoms and there is a lack of literature on the treatment strategies for these refractory patients. In this case, we supplemented the multidisciplinary approach through novel, therapeutic strategies, including biofeedback, dose-adjusted BoNT injections, and rTMS, which demonstrated efficacy and successfully reduced symptoms. This is the first reported case of refractory PVFMD treated with novel interventions and specifically rTMS, which might play a role in PVFMD mitigation.
The Institutional Review Board of Tri-Service General Hospital, National Defense Medical Center, had approved this study (Case No. A202215114).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.