
Abstract
This case report presents a 72-year-old man with longstanding recurrent respiratory papillomatosis (RRP). He has undergone multiple procedures for the condition, including an apparent urgent surgical airway followed by tracheoplasty repair. Modern management of complicated RRP should include both local debulking and systemic approaches. Systemic bevacizumab (Avastin) has shown some initial success as an effective treatment option, in addition to other medications such as pembrolizumab. Other future care strategies may include an HPV vaccination and other adjuvants; vaccination has been reported to have the possibility of drastically reducing the incidence of RRP.
Keywords
Introduction
Recurrent respiratory papilloma (RRP) is a chronic respiratory tract disease of viral etiology that causes recurrent benign papilloma growth,1-4 classically described as a benign neoplasm of the larynx.5,6 The causative virus is HPV subtypes 6 and 11, and it mainly affects the larynx, although the oral cavity and trachea are frequently involved. 6 RRP is characterized by the proliferation of benign squamous papilloma within the aerodigestive tract and, although benign, can undergo malignant conversion. 6
It is important to note that RRP occurs in both adults and children, although the juvenile form occurs before age 12 and is far more aggressive than the adult form.6-8 Following voice changes, stridor has been reported to be the second most common symptom—inspiratory than basic. 6 Recent literature concludes that the biology of RRP is still not well known, but it is known that RRP becomes more aggressive in the context of immune suppression. 8 There is no known cure, and the mode of transmission in adults is unclear. 6
Case presentation
The patient is a 72-year-old man with a past medical history of hypertension, Type-II diabetes mellitus, and prostate cancer who presented with dysphonia and dyspnea. In-office flexible laryngoscopy revealed papillomatosis of the epiglottic petiole, bilateral false vocal folds, and bilateral true vocal folds with visible shadowing in the subglottis. He is a former tobacco user and reported quitting smoking in the 1970s. He was initially diagnosed at age 10 on the small Caribbean Island where he was born. At that time, he was taken to Jamaica for his initial surgical therapy and pathological confirmation of the diagnosis; he returned there several times for care. He has come to the US on several occasions for care and has been seen by 2 physicians in the same practice since May 2011, prior to coming under the senior author’s care in September 2021.
Due to the fractured nature of his care, the details of some of his previous medical history are unclear. In 2007, a left vocal fold (VF) immobility was identified. He has an unexplained right thyroid lamina fracture and underwent a vaguely described laryngotracheoplasty with iliac crest bone grafting in Jamaica at an unclear point in time. In 2009, he was in Jamaica with profound respiratory distress, which resulted in intubation and tracheostomy; he has since been decannulated. In 2011, he presented in New York with a note from his doctor in Jamaica requesting advanced care and outlining his past medical and surgical history. Additional care included at least 5 surgical debridements by physicians in the senior author’s practice, dating back to 2011.
In January 2016, an anterior commissure laryngoscope was used to expose the glottis clearly and identify the anatomic components of the airway. The anesthesia team was able to place a 5.0 standard endotracheal tube (ETT) during that episode of care. Tissue biopsies were taken, and the pathology at this time was “squamous papilloma with mild dysplasia and mild acute inflammation.” In November of 2017, the description in the operative note reflects “obstructive papilloma at the mid-trachea circumferentially, involving the site of the prior tracheoplasty.” The pathology at that time was “fragments of squamous papilloma with mild to moderate dysplasia.” In March 2019, a Benjamin slimline laryngoscope was required to secure his airway. Biopsies taken at each surgery resulted in “fragments of squamous papilloma with mild to moderate dysplasia.” In November 2020, 80% luminal patency was achieved in the distal airway, but a 5.0 ETT was required to ventilate him at the end of the case.
In September of 2021, the senior author performed a microlaryngoscopy, achieving airway exposure with a Lindholm laryngoscope, allowing more working space. Ventilation was managed with high flow nasal cannula oxygenation so that the airway could be examined and treated without an endotracheal tube in place. The pathology again similarly resulted in fragments of squamous papilloma, this time with focal mild dysplasia. Intraoperative photos show diffuse proliferation of exophytic papilloma lesions (Figure 1). (A–F): Operative photos from the procedure. (A) Endoscopic view of the trachea, approaching the level of the prior tracheostomy and tracheoplasty; (B) endoscopic view of bulky papilloma at the site of the prior tracheostomy and tracheoplasty; (C) endoscopic view of the interarytenoid space; (D) endoscopic view of the subglottis, above the level of the tracheostomy/tracheoplasty; (E) endoscopic survey view of the glottis and infrahyoid epiglottis, and (F) close-up view of the posterior aspect of the glottis.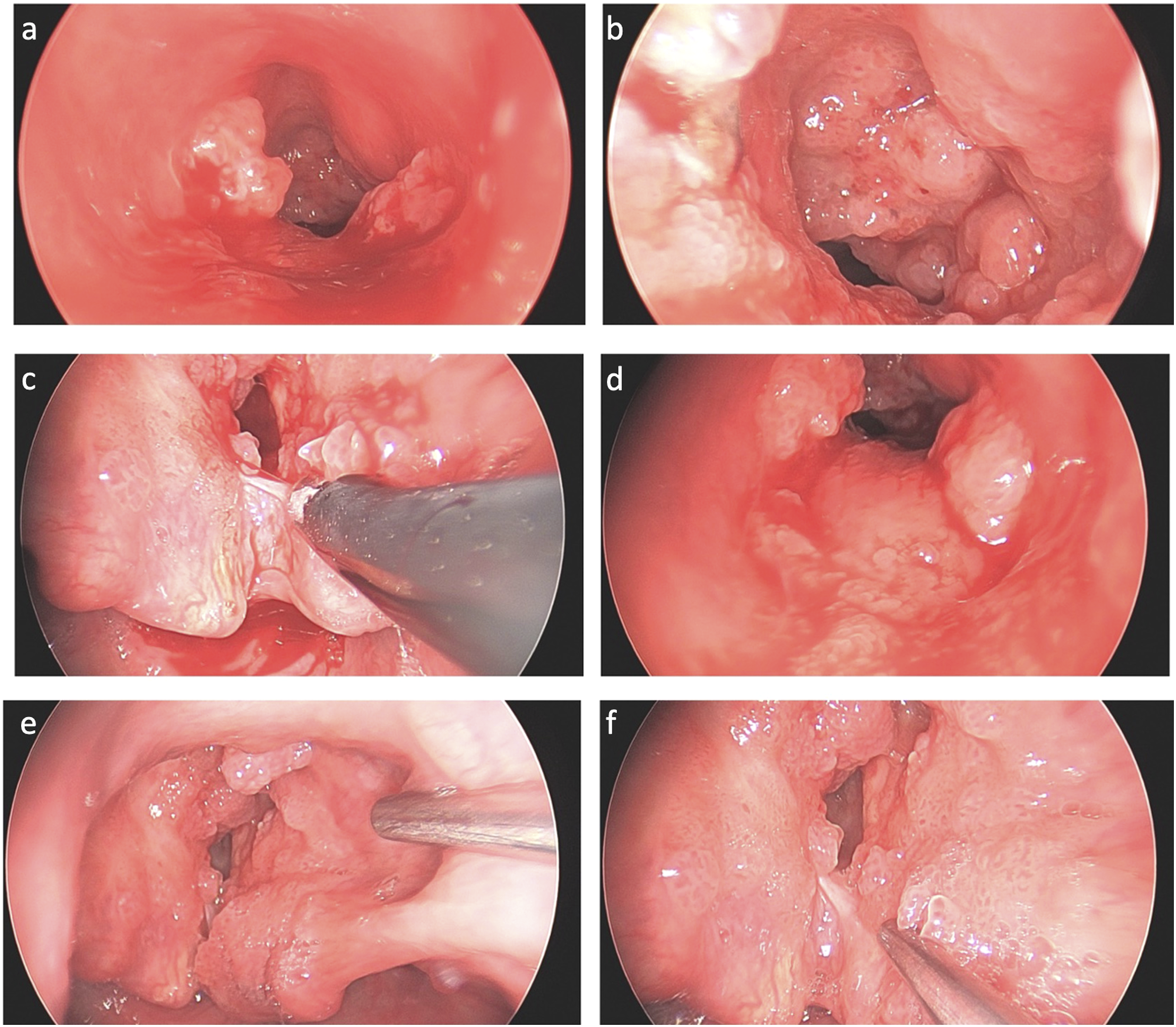
While the microdebrider had been used in the past, the coblator was employed on this occasion to remove the bulky lesions. The senior author preferred this tool since it combines ablative and coagulation functions. As this care episode occurred during the SARS-CoV-2 pandemic, additional draping was used to reduce respiratory droplet aerosolization while using the HiFLow NC Oxygen. In addition, standard universal precautions were in place, and all staff wore appropriate high filtration masks (N95) and eye protection in accordance with OSHA, CDC, and JCAHO guidelines.
Since the patient has had this condition for over 60 years and had frequent gaps in care (due to traveling between his island, Jamaica, and New York), it is essential to consider his risk for distal parenchymal disease. A chest radiograph series showed that he has no cavitary or consolidated lesions, although it does not mean there is not more distal mucosal involvement (Figure 2). He remains at risk for malignant transformation but, to date, has never progressed beyond moderate dysplasia Chest X-ray showing no cavitary or consolidated lesions.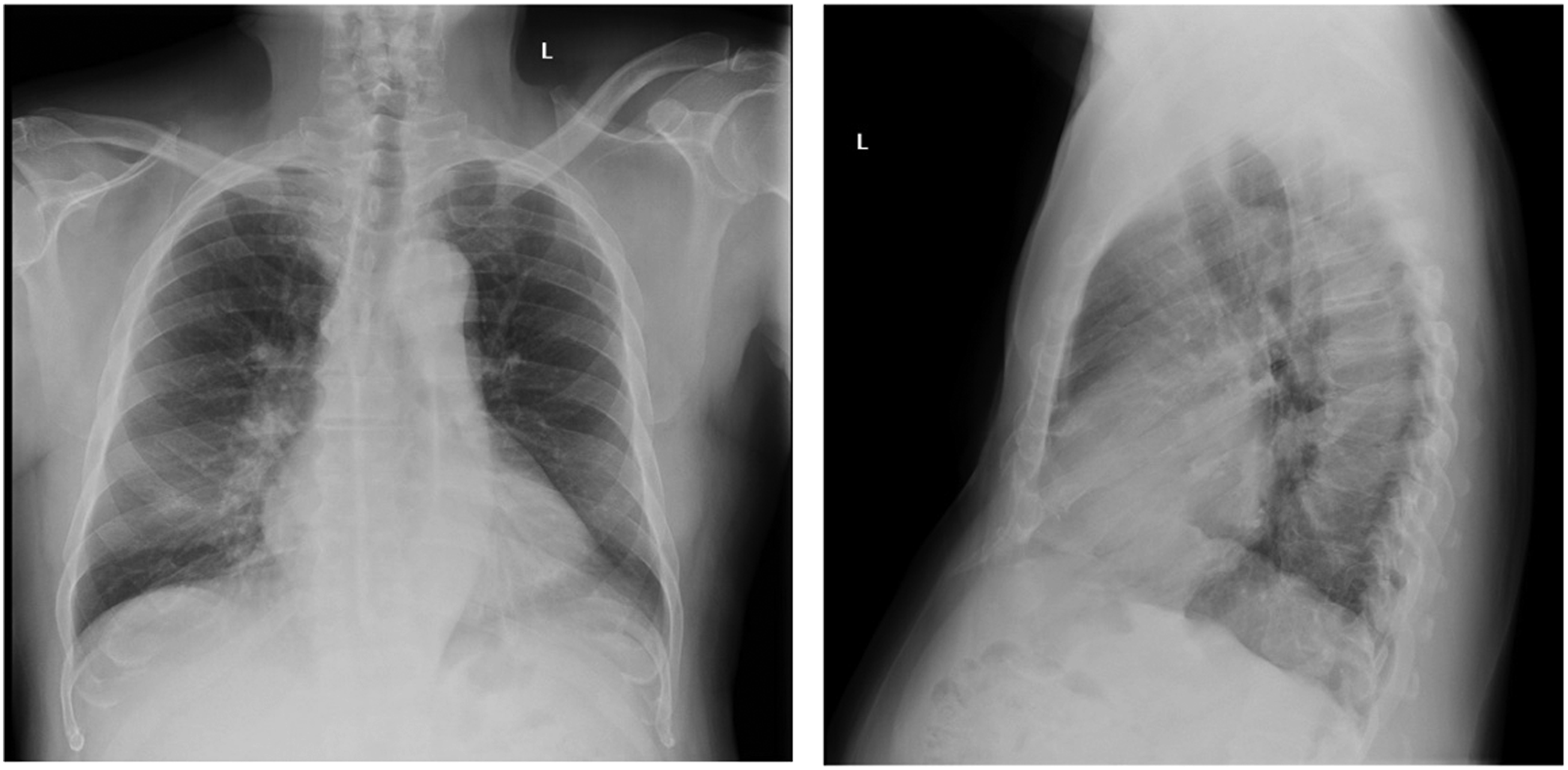
Discussion
The projected incidence of RRP in the USA, based on a 1995 study, is about 1.8 per 100,000 in adults. 9 The morbidity of this condition is low, and the prognosis is reported to be often good but may be variable with clinical behavior. 9 The burden of RRP is high despite the low prevalence. Larson et al. cite the reason for the high burden being that multiple procedures are required of the patients with this diagnosis. 10 This disease places not only a significant economic burden on individual patients and their families but on society, with adult patients requiring more than 40 lifetime procedures and estimated lifetime cost to be between $60,000 and $470,000 in the United States. 10 In addition, the disease affects the quality of life due to airway obstruction and dysphonia. 5
The treatment of respiratory papillomatosis has evolved over the years from tracheostomy to an armamentarium, including debridement of lesions with cup forceps, LASER, microdebrider, or plasma field tools. Surgery is needed to ensure airway patency, preserve underlying laryngeal tissues, and maintain acceptable voice quality. However, multiple surgeries may be needed in a short period of time due to numerous lesions requiring excision. 9 The choice of technique depends on the availability and familiarity of the operating surgeon. Each of these surgical techniques holds its own complications. Laser ablation has been shown to increase respiratory tract burns and laryngeal scarring. The microdebrider tool is far more precise, but resection is still frequent given the nature of the disease. 11 Issues arising from treatment may include resistance to therapies, recurrence, or dissemination or extension of the growths to lower airways, correlating with a poorer prognosis. 9
It is essential to consider systemic treatment in a case such as this one, with medications such as pembrolizumab, which has been shown to decrease the need for routine surgical intervention and has also shown consistent benefits.12,13 Systemic bevacizumab (Avastin) has proven to be an effective treatment option as it has demonstrated significant treatment-resistant and aggressive papillomatosis results and includes a low complication profile.14-16 It is a VEGF inhibitor that has been shown to reduce recurrent papilloma epithelial growth and improve dose-related quality of life. 17 Patients have experienced increased time between surgeries, and as an adjunctive treatment, bevacizumab has been shown to resolve symptoms of pulmonary papilloma. Minor complications are extremely rare and have been seen as hemoptysis and proteinuria. 16 Working with a team of thoracic surgeons and medical oncologists may prove necessary due to certain risks, such as bleeding. 18 With this being said, medical treatment alone is unable to control or eradicate the disease. 9
Overall treatment should include both local debulking and systemic approaches, including considering an HPV vaccination, although this consideration has not been proven to be medical therapy. 19 Monitoring progression is a high priority in light of the absolute disease burden and the length of time the patient has been infected. Chaturvedi et al. reports concluded that the action of anti-viral drugs at regular intervals in addition to a short course term of oral steroids led to rapid recovery and prevented latent virus activation within the laryngotracheal system, maintaining long-term improvement. 20
Transformation of RRP to dysplasia and invasive carcinoma can occur, with disease onset being the strongest predictor of dysplastic transformation in both the adult and pediatric populations. 5 One study found that dysplasia was discovered in more than 20% of adult patients with RRP studied over a 6-year period. Age, tobacco history, and operative frequency were not identified as risk factors for dysplasia presence. 21 In another study of 159 RRP patients, age of disease onset was a predictor of transformation to dysplasia of carcinoma-ex-papillomatosis in adults and pediatric populations, and it was found that no other demographic or behavioral factors were associated with this transformation. 5 Dysplasia can be reported to be common in those with RRP, and the progression of dysplasia from an initial dysplastic grading of benign or mild is reportedly rare. 22 The study by Karatayli-Ozgursoy et al. found that age of disease onset is predictive of dysplasia or carcinoma-ex-papillomatosis in both adult- and juvenile-onset recurrent respiratory papillomatosis and adults who are eventually diagnosed with dysplastic or malignant degeneration initially present more than a decade later in life (56 vs. 45 years old, P = 0.005). 5
In 2018, Derkay et al. reported that there may be new treatments for RRP. Advances in the treatment of RRP include novel DNA vaccine development and differential ligand expression in the papillomatous milieu and investigational use of therapies previously used for viral hepatitis or ocular neoplastic disease. 23 For example, Derkay et al. reports the use of pegylated interferon, used as a hepatitis C treatment and cure, in treating a child with severe RRP with good response. 23 Bevacizumab (Avastin) has also been studied and has been reported to be on the rise as a treatment.
As of 2018, best practice recommendations for systemic bevacizumab administration in those with RRP include a partnership with oncology for off-label consent and arranging for infusions with hospital approval. 23 The main side effects include hypertension, thrombus, electrolyte imbalances, and renal damage. Derkay et al. recommend screening for sequelae and obtaining baseline studies, including a cardiac echocardiogram. They also report that the patient’s disease should first be debrided in the operating room, followed by Avastin 10 mg/kg infusions for 90 minutes, with the following procedure and infusion after 3 weeks, with intervals ranging from 2 to 3 months.
Conclusion
The patient in this case is a 72-year-old man who presented with recurrent respiratory papillomatosis (RRP), which is a chronic respiratory tract disease of viral etiology that causes recurrent benign papilloma growth, classically described as a benign neoplasm of the larynx, along with focal mild dysplasia following diagnoses of left vocal cord immobility, right thyroid lamina fracture, a laryngotracheoplasty with iliac crest bone grafting, and a tracheotomy. There is no known cure, and the mode of transmission in adults is unclear.
Treatment should involve both local debulking and systemic treatments. Systemic bevacizumab (Avastin) has been proven to be an effective therapeutic option for treatment-resistant and aggressive papillomatosis, with considerable outcomes. Other future care strategies may include an HPV vaccination. Monitoring of progression is critical, and regular follow-up is needed for this chronic disease.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Consultant for Smith & Nephew.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.