
Abstract
This case study presents an abnormal complication after routine injection augmentation using calcium hydroxylapatite (CaHA) vocal fold filler in-office on a 73-year-old female. The patient presented initially with severe dysphonia, hypophonia, and a past surgical history of total thyroidectomy, bilateral neck dissection, and a right lateral neck dissection for history of metastatic papillary thyroid carcinoma. She also had a past medical history of hypothyroidism. Post-injection of CaHA, the patient developed severe laryngeal edema, limited vocal cord mobility, obliteration of the pyriform, and a significantly reduced airway aperture requiring intensive care monitoring. Although uncommon, injectable fillers can result in complications which can be severe. Careful technique, the volume of injectate, and hypersensitivity should be considered in reducing complications following injection augmentation. There are multiple injection techniques to consider. The most direct approach is with direct laryngoscopy to allow for visualization of glottic incompetence. A smaller slotted laryngoscope can be considered for vocal fold injection as an alternative and without endotracheal intubation. Although these techniques allow for injection, real-time assessment of vocal fold closure is done in an awake patient. Therefore, laryngeal injection can be considered via percutaneous, per-oral, and trans-nasal approaches.
Introduction
Laryngeal disorders, especially those involving glottal insufficiency, are a relatively common aspect of laryngology and have a wide array of treatment approaches. 1 In office, vocal fold injection augmentation is a routine treatment of glottic insufficiency. Calcium hydroxylapatite (CaHA), a synthetically derived material, is a commonly utilized long-term filler material. For years, calcium hydroxyapatite has been used as an effective long-term vocal fold injection. An in vivo canine fold model and a multi-institutional clinical trial suggested adequate vocal fold medialization for approximately a year without appreciable inflammation.1,2
This substance is known to be both safe as well as well-tolerated and has been in use for over 25 years.3,4 CaHA has been proven to be a stable implant with minimal inflammatory response and no evidence of toxicity. 1 Vocal fold injections have been reported to have been performed for the previous 100 years with various materials. 1 Currently available vocal fold augmentation materials vary in their duration or require a significant amount of preparation.
Case Report
A 73-year-old female presented with a weak and breathy voice to our clinic. She had undergone total thyroidectomy, right modified neck dissection, and right lateral neck dissection with sacrifice of the right recurrent laryngeal nerve (RLN) due to invasive disease with another provider. She also had neuroplasty of the vagus nerve and RLN and reimplantation of the right inferior parathyroid. RLN monitoring was performed in October of 2020. Intra-operative neurorrhaphy of the recurrent laryngeal nerve was not performed. Following thyroidectomy, the right vocal fold was in a paramedian position, and the left vocal fold was atrophied and mobile. Her past medical history was significant for breast cancer, where she underwent a lumpectomy without radiation, vocal fold atrophy with glottic insufficiency, and hypothyroidism. She had a known allergy to penicillin.
Her postoperative videostroboscopy was significant for bilateral vocal fold atrophy, right unilateral vocal fold immobility, and severe glottic insufficiency with secondary supraglottic hyperfunction. The patient stated that she had a “breathy” voice for years prior to her surgery, a symptomatic correlate to bilateral fold atrophy. Preoperative evaluation prior to October 2020 demonstrated bilateral vocal fold atrophy with mobile cords. This was significant as the patient had a history of pre-existing glottic insufficiency and a gap that was exacerbated by vocal fold paralysis. In retrospect, given the large size of the gap (approximately 4 mm), injection augmentation had a lower probability of improvement in voice.
After discussion of her options, including medialization, short-term fillers, and CaHA, the patient was elected for CaHA injection augmentation; the patient underwent flexible laryngoscopy and injection augmentation of the right true vocal fold with 0.6 ccs of CaHA (Prolaryn Plus, Merz North America, Raleigh, NC, USA) in January of 2021.
The patient’s response was suboptimal, and she proceeded with microdirect laryngoscopy and injection augmentation of the bilateral true vocal folds with similar material three months later, in April of 2021. An additional 0.3 cc was injected into the right true vocal fold (TVC) and 0.6 ccs into the left TVC. The procedure was tolerated well, and the patient was discharged home the same day.
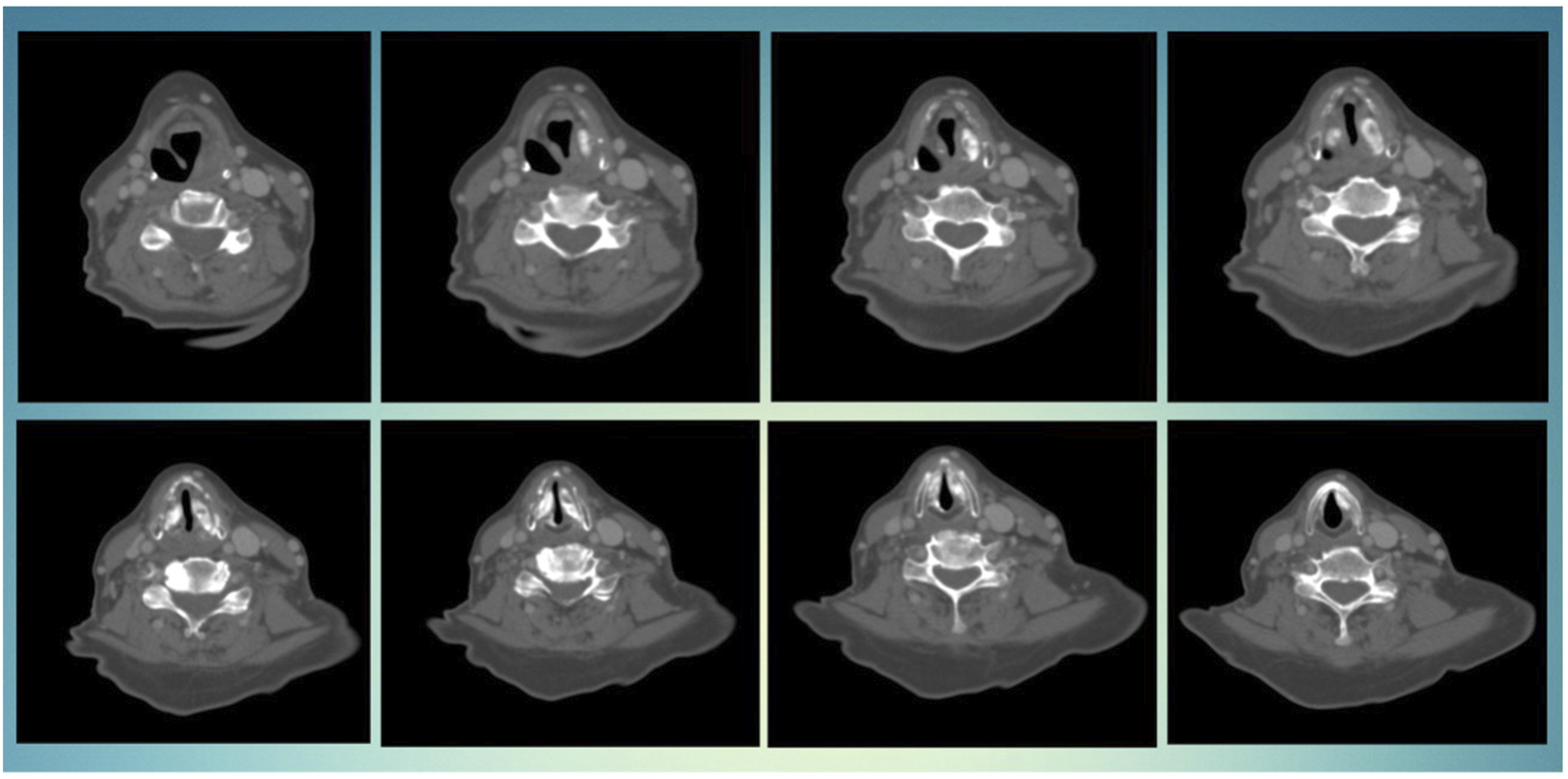
On postoperative day 2, the patient developed stridor and shortness of breath. She was evaluated in the emergency department and was afebrile, and her oxygen saturation was 100% on 5 L nasal cannula. On arrival, her labs were as follows: white blood -count – 4.4, hemoglobin – 13.1, Hhematocrit – 40.9, platelet (thrombocyte) count – 205, and blood glucose – 128, and her comprehensive metabolic panel was otherwise within normal limits. Her examination was significant for inspiratory stridor, rough, strained voice, and suprasternal retraction. The neck examination was normal. Flexible laryngoscopy revealed severe watery bag edema of the left arytenoid edema and obliteration of the pyriform sinus (Figure 1 and Figure 2). The left vocal fold was severely hypomobile secondary to edema. The right vocal fold was edematous, erythematous, and immobile per previous RLN sacrifice. Anterior to posterior coronal view. A total of 0.9 ccs was injected into the right vocal cord, and 0.6 ccs were injected into the left vocal cord. The injection is slightly subglottic as well as superiorly positioned. Glottic stenosis is appreciated. Axial view. Severe edema on the left side with obliteration of the pyriform. An abundance of material in both the left and right cords. The limited airway can also be seen.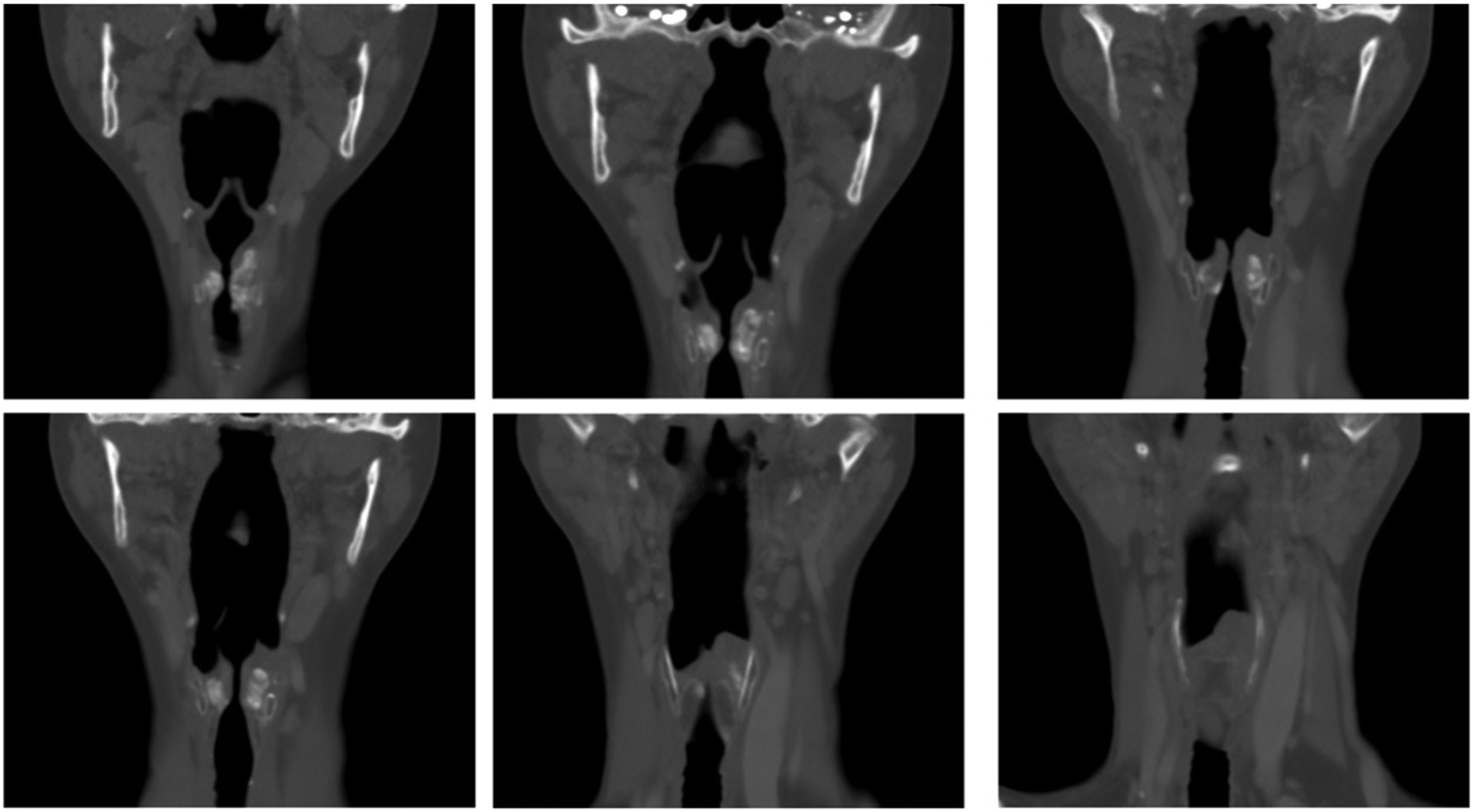
The patient was given racemic epinephrine and 6 mg dexamethasone (Decadron) every 6 hours. Given her penicillin allergy, ceftriaxone was started as an inpatient, and she was transitioned to cefdinir per os. She was admitted to the ICU, where steroids and antibiotics were continued. An emergent airway cart, including a tracheostomy tray and an intubation cart with small bore endotracheal tubes, was kept at the bedside.
There were no events overnight, and flexible laryngoscopy showed significantly improved airway edema and left vocal fold mobility on hospital day 2. The patient’s stridor and retractions resolved, and fiberoptic endoscopic evaluation of swallowing (FEES) showed she was unremarkable for penetration, aspiration, or post-swallow residue. She was discharged home with a puree diet, prednisone, cefdinir, and close outpatient follow-up. Upon complete absorption of CaHA, she will proceed with type I thyroplasty.
Discussion
Complications occurring with CaHA are rare. Similar reactions have been seen with hyaluronic acid (HA). In a review of 467 patients receiving HA, one was intubated, and 3 others were admitted for airway observation. Seven in total (1.7%) developed inflammatory reactions. 5 Review of the literature also demonstrated an extra-thyroidal neck abscess thought to be secondary to extra laryngeal injection of CaHA into the superficial neck space. 6 One patient experienced anaphylaxis after CaHA injection 2 and another pulmonary embolism due to the foreign body. 3
Given the relatively short duration between the 2 injections, the patient described here may have developed a hypersensitivity reaction. There are different hypersensitivities associated with CaHA to consider. The patient's induration and timing before the reaction took place supports a delayed type hypersensitivity. Her immediate response to steroids further supports this.
Others have postulated that over-injection may cause vascular compression and resultant edema. Vascular occlusion is a potentially severe adverse outcome. Although the resultant tissue changes and edema can result in vascular compression, CaHA is also noxious stimuli. The subsequent inflammation, when administered, can worsen vascular edema. The timing of the patient's presentation means foreign body injection must also be considered. 7
CaHA was the corresponding author's injectable of choice at the time of this case. Given the complications, which include airway edema, vocal fold inflammation, and overall non-optimal results, the author has since changed his practice to favor hyaluronic acid (HA) injections in contrast to CaHA. Medialization thyroplasty has been discussed with the patient as well as shorter-term injectables (HA and carboxymethylcellulose); however, the patient did not wish to proceed with open surgery in the near future, which gives reason for the use of a long-term injectable being utilized.
Conclusion
Calcium hydroxylapatite is a routine injectable that can be used to treat various vocal cord pathologies. Although uncommon, severe complications have been reported, as demonstrated here. The volume of injection, position, and duration between injections should be considered in order to minimize the likelihood of a complication.