
Abstract
Objectives
To explore the degree to which patients undergoing unilateral endoscopic sinus surgery (ESS) experience post-operative contralateral sinonasal symptoms and determine risk factors for contralateral symptomatology following unilateral ESS.
Methods
Patients who underwent unilateral surgery for chronic rhinosinusitis (CRS) were contacted and asked if they felt symptomatic on the contralateral side at that point in time. Nasal Obstruction Symptom Evaluation (NOSE) scores were obtained based on contralateral symptomatology they recalled at the following time points: pre-ESS, 1 month post-ESS, and 3 months post-ESS. Demographics, contralateral symptomatology, and NOSE scores were compared between those with 2 or fewer sinusotomies versus 3 or more sinusotomies.
Results
Of the 97 patients included in this study, 24% of patients reported contralateral congestion, a median of 24 months post-ESS, and more than 10% of patients reported other contralateral symptoms including swelling, rhinorrhea, difficulty breathing, and hyposmia post-ESS. Those with 2 or fewer sinusotomies were more likely to feel that they had developed worsened sensation of contralateral sinus swelling (P = .008). The median amount of time from the participants’ index surgery until the time they were interviewed was 24 months. There were no differences in long-term contralateral symptomatology between those who did and did not have septoplasty (27%).
Conclusion
Patients who have unilateral ESS for CRS may experience long-term contralateral symptoms. Having a septoplasty did not affect contralateral symptoms.
Keywords
Background
Chronic rhinosinusitis (CRS) is an inflammatory disorder of the paranasal sinuses and nasal passages that lasts for a minimum of 12 weeks.1,2 Although patients with CRS typically suffer from bilateral disease, a minority of patients do suffer from unilateral disease. 3 Though there are a variety of indications for unilateral endoscopic sinus surgery (ESS) including acute sinusitis, CRS with or without nasal polyposis, antrochoanal polyp, fungal sinusitis, mucoceles, and benign or malignant neoplasia,4,5 CRS continues to be the most common diagnosis for patients with unilateral disease requiring surgical intervention.6,7
Investigations that have been conducted to determine outcomes after ESS in patients with CRS do not generally differentiate between unilateral and bilateral disease. One study investigated 39 participants with unilateral chronic rhinosinusitis and found 88% of the participants felt a significant improvement in their presenting complaints of mucopurulent rhinorrhea, nasal obstruction, and facial pain after an average of 26-month follow-up. 8 Studies such as this suggest that ESS is effective for treating unilateral nasal sinusitis. A few studies have compared outcomes after ESS for bilateral CRS versus unilateral CRS. A study investigating 181 participants with CRS with nasal polyposis (23 participants with unilateral CRS and 158 participants with bilateral CRS) found that the extent of nasal polyposis and Lund-Mackay score (LM) did not differ significantly between the two groups post-ESS, but the unilateral group showed significantly better objective outcomes than the bilateral group, suggesting that the developmental mechanisms of the two disease entities may differ. 9 Similarly, a study investigating 190 participants with CRSwNP (171 with bilateral disease and 19 with unilateral disease) found no significant difference in improvement in symptomatic severity post-ESS between the two groups.
Although a few studies have compared post-surgical outcomes after ESS for individuals with unilateral versus bilateral CRS, little published literature has examined post-surgical symptoms for individuals with unilateral CRS. The purpose of this study is to determine the extent to which patients experience contralateral CRS symptoms after unilateral ESS and determine risk factors for contralateral symptomatology following unilateral ESS.
Methods
Data collection
This study received approval from the affiliated Institutional Review Board. In the time period 2015–2020, 174 consecutive patients underwent unilateral ESS by author KCW at Northwestern Memorial Hospital. Of these patients, 77 individuals were not reachable by phone call or refused to participate. The remaining 97 patients were contacted and consented via telephone. The charts of these 97 patients who underwent unilateral ESS performed at Northwestern Memorial Hospital from 2015 to 2020 were reviewed. These participants were contacted via telephone and asked if they recalled feeling symptomatic on the contralateral side at specific points in the post-operative period.
Nasal Obstruction Symptom Evaluation (NOSE) scores were obtained based on contralateral symptomatology the participants recalled from the following time points: Pre-ESS, 1 month post-ESS, and 3 months post-ESS. 10 While each of these patients underwent their unilateral sinus surgery at some point from 2015 to 2020, they were asked to recall symptomatology at each of those time points before and after the surgery. Implementing the NOSE tool, patients were asked to grade their symptoms of congestion, blockage, trouble breathing, trouble sleeping, and having to breathe through their mouth on a 5-point Likert scale. NOSE scores were only obtained for the patients’ contralateral side, which was the side not operated on. In addition, participants were asked whether they felt worsening of contralateral congestion, rhinorrhea, swelling, earache, sense of smell, or difficulty breathing after the unilateral ESS compared to beforehand. Patients’ pre-operative endoscopy results were also reviewed using the Lund-Kennedy endoscopic scoring system in their respective charts. Demographics, contralateral symptomatology, and contralateral NOSE scores were compared between those with 2 or fewer sinusotomies versus 3 or more sinusotomies.
Statistical analysis
Statistical analysis was carried out using Prism GraphPad software version 9 (GraphPad Software, La Jolla, Calif.) and SPSS 24 (Armonk, NY). We assessed variables for normality using Kolmogorov–Smirnov and Shapiro–Wilk tests. Descriptive categorical data is presented as frequency counts and percentages. Descriptive continuous data is presented as median and interquartile range (IQR) when non-normally distributed and mean and standard deviation (SD) when normally distributed. Mann–Whitney U test and independent t-tests were used to analyze differences between the medians and means of two groups, respectively. Pearson’s chi square was used to compare differences in categorical data between groups.
Results
Demographic characteristics.
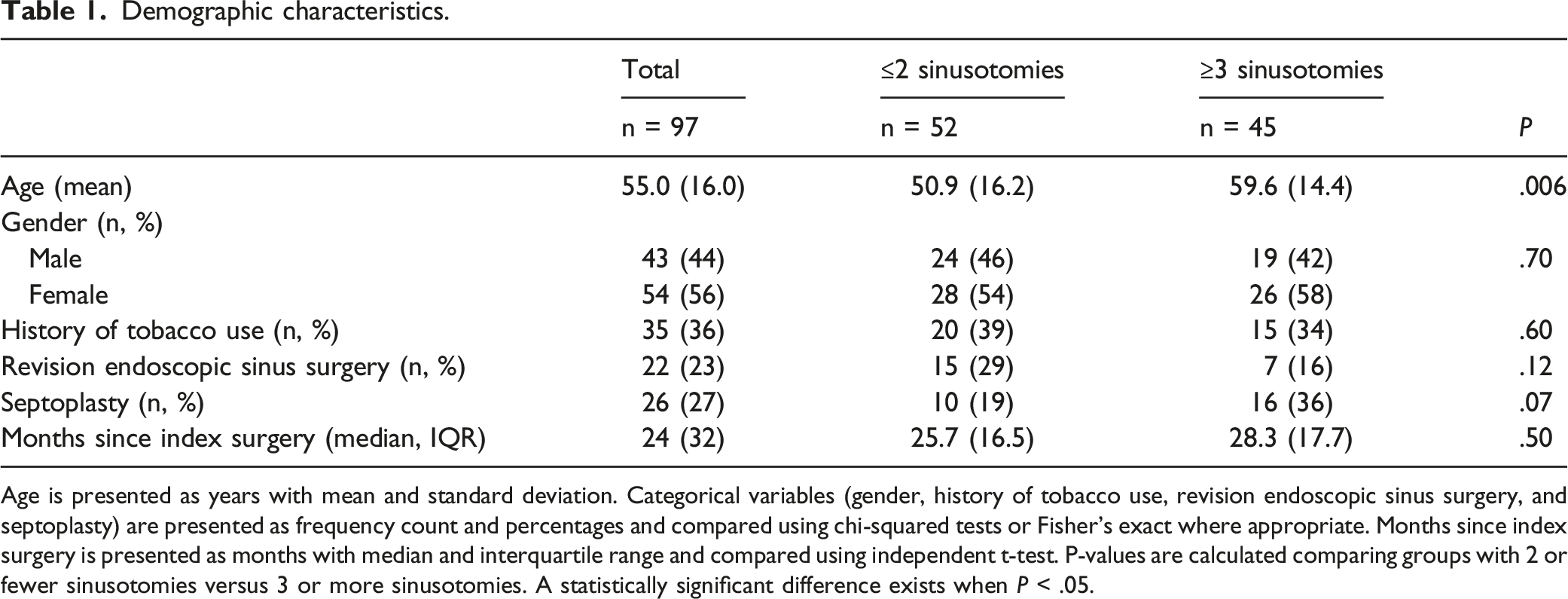
Age is presented as years with mean and standard deviation. Categorical variables (gender, history of tobacco use, revision endoscopic sinus surgery, and septoplasty) are presented as frequency count and percentages and compared using chi-squared tests or Fisher’s exact where appropriate. Months since index surgery is presented as months with median and interquartile range and compared using independent t-test. P-values are calculated comparing groups with 2 or fewer sinusotomies versus 3 or more sinusotomies. A statistically significant difference exists when P < .05.
Table 1 also shows the demographic characteristics of the sample stratified by number of sinusotomies undergone, with one group undergoing 2 or fewer sinusotomies and the other group undergoing 3 or more sinusotomies. This stratification was done for the purposes of statistical analysis particularly regarding comparing demographics between groups including septoplasty. Table 1 indicates no significant difference in demographic characteristics of gender, history of tobacco usage, revision ESS, septoplasty, or time passed since index surgery between the two groups. There was a statistically significant difference in the average age of the two groups, with an average age of 50.9 ± 16.2 years for the group with 2 or fewer sinusotomies versus average age of 59.6 ± 14.4 years for the group with 3 or more sinusotomies (P = .006).
Contralateral chronic rhinosinusitis symptoms post-endoscopic sinus surgery.
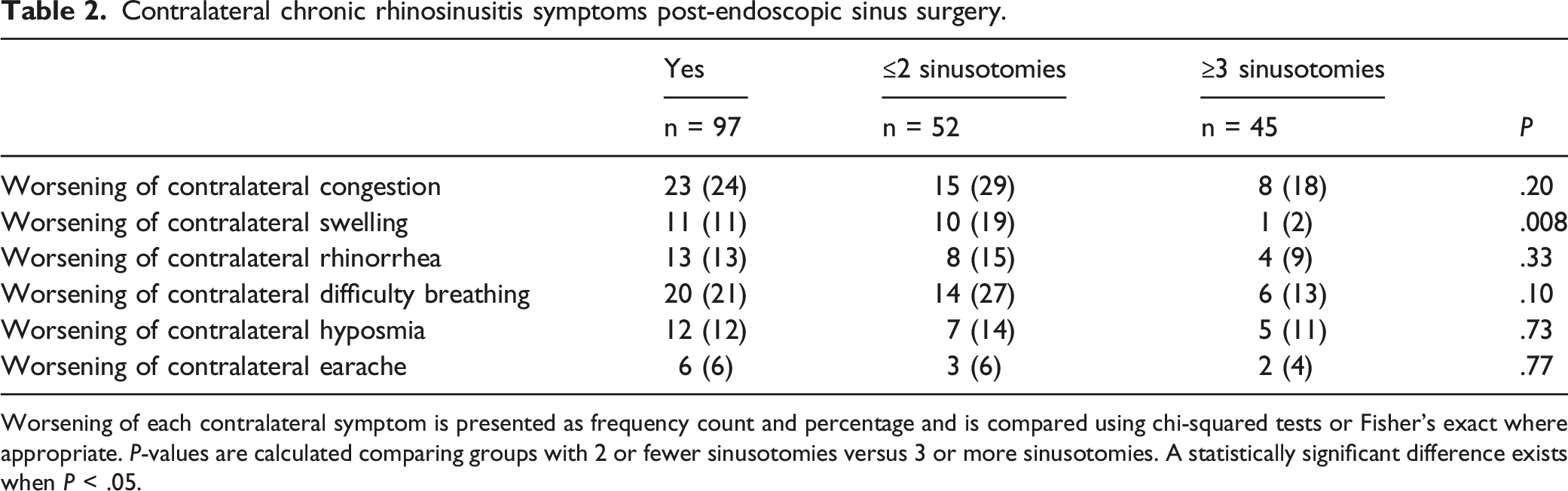
Worsening of each contralateral symptom is presented as frequency count and percentage and is compared using chi-squared tests or Fisher’s exact where appropriate. P-values are calculated comparing groups with 2 or fewer sinusotomies versus 3 or more sinusotomies. A statistically significant difference exists when P < .05.
Table 2 also shows contralateral symptomatology experienced by participants in this study post-ESS stratified by number of sinusotomies undergone. There was a statistically significant difference in number of participants who experienced worsening of contralateral swelling between those who had 2 or fewer sinusotomies compared to 3 or more sinusotomies. 19% of those with 2 or fewer sinusotomies experienced worsening of contralateral swelling, whereas only 2% of those with 3 or more sinusotomies experienced worsening of contralateral swelling (P = .008). Regarding worsening of contralateral difficulty breathing, congestion, rhinorrhea, hyposmia, or earache, there was no statistically significant difference between the groups of 2 or fewer sinusotomies versus 3 or more sinusotomies.
Contralateral nasal obstruction symptom evaluation scores pre-endoscopic sinus surgery (ESS), 1 month post-ESS, and 3 months post-ESS.
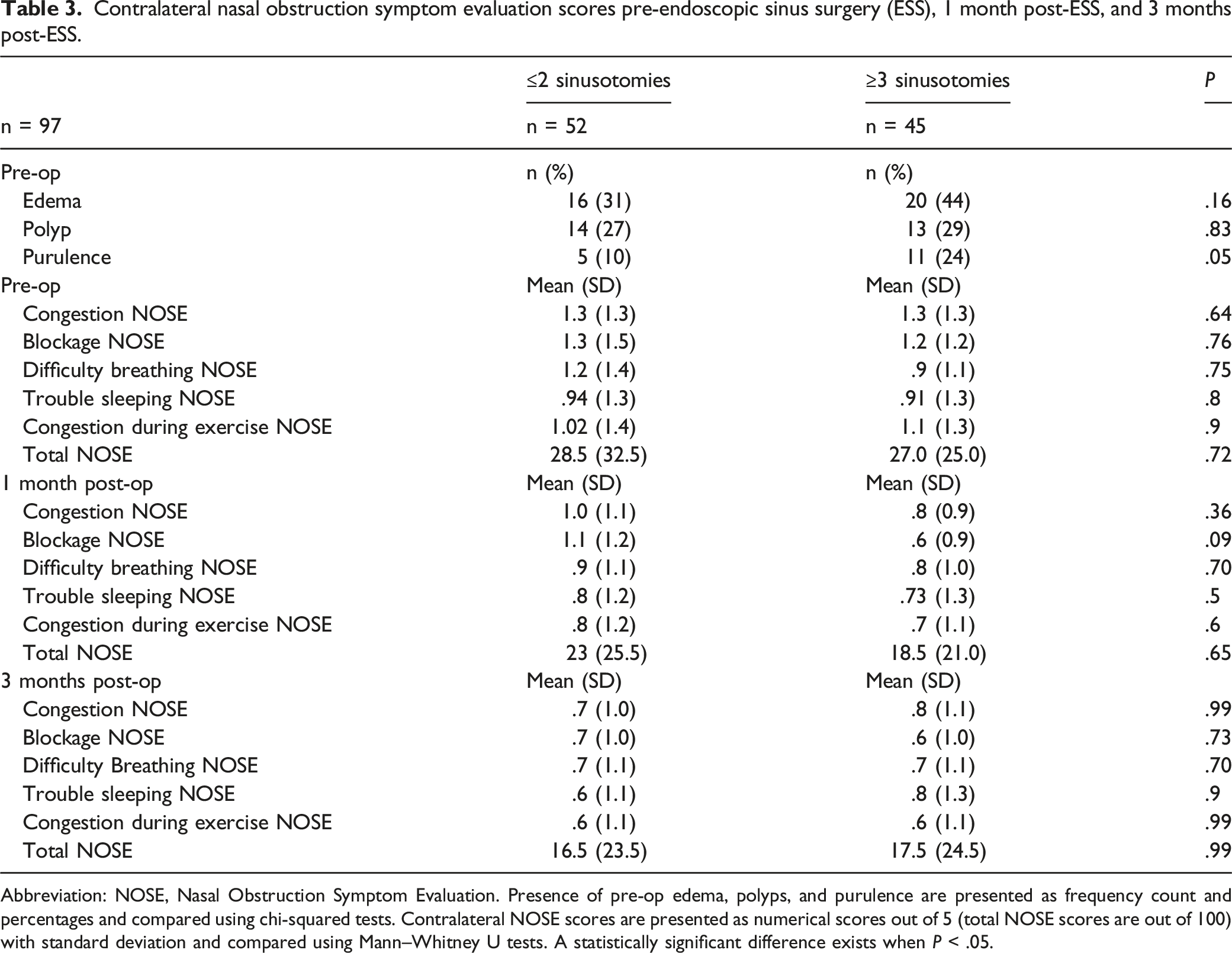
Abbreviation: NOSE, Nasal Obstruction Symptom Evaluation. Presence of pre-op edema, polyps, and purulence are presented as frequency count and percentages and compared using chi-squared tests. Contralateral NOSE scores are presented as numerical scores out of 5 (total NOSE scores are out of 100) with standard deviation and compared using Mann–Whitney U tests. A statistically significant difference exists when P < .05.
Contralateral chronic rhinosinusitis symptoms post-endoscopic sinus surgery stratified by septoplasty.
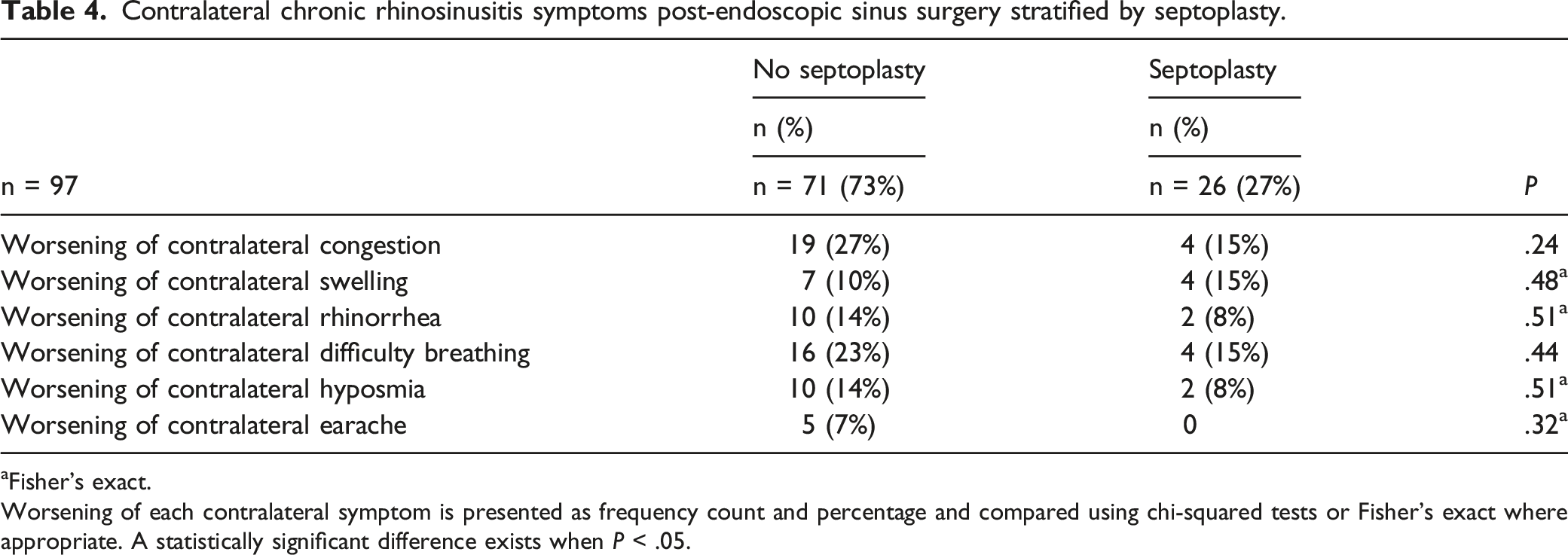
aFisher’s exact.
Worsening of each contralateral symptom is presented as frequency count and percentage and compared using chi-squared tests or Fisher’s exact where appropriate. A statistically significant difference exists when P < .05.
Discussion
In this study, we found that 24% of participants experienced subjective worsening of contralateral congestion, a median of 24 months post-ESS when compared to pre-ESS. More than 10% of participants experienced worsening of other symptomatology including contralateral swelling, rhinorrhea, difficulty breathing, and hyposmia post-ESS. These results indicate that participants who undergo unilateral ESS may go on to experience contralateral symptomatology. Our study is the first to investigate long-term contralateral symptomatology following unilateral ESS. Multiple reasons may exist for individuals experiencing contralateral symptoms following unilateral ESS. For one, ESS has been shown to be an effective mode of management for chronic rhinosinusitis for both bilateral and unilateral sinusitis.8,11-14 Individuals most likely felt a significant improvement on the side on which the unilateral ESS was done. After a drastic improvement on one side of their sinuses, the other side may feel relatively worse. In addition, it could be possible that unilateral ESS may result in worsening the function of the contralateral sinuses.
In this study, we also found that individuals with 2 or fewer sinusotomies were more likely to experience worsening of subjective sensation of contralateral sinus swelling compared to individuals with 3 or more sinusotomies (19% vs 2%, P = .008). Swelling was the only contralateral symptom that had a statistically significant difference in it worsening post-ESS between the 2 cohorts. Although there was a non-statistically significant difference, 27% of those with 2 or fewer sinusotomies experienced worsening of contralateral difficulty breathing, whereas only 13% of those with 3 or more sinusotomies experienced worsening of contralateral difficulty breathing (P = .10). This indicates that individuals who undergo unilateral sinus surgery and have 2 or fewer sinusotomies may be more likely to report worsening of contralateral subjective CRS symptoms than those with more sinusotomies. An explanation may be that the individuals who had 3 or more sinusotomies most likely warranted more surgery originally—as such, they may have been less likely to experience CRS symptomatology post-ESS both on the original side and contralateral side compared to those who required fewer sinusotomies. Further research is needed to determine the role of number of sinusotomies in contralateral symptomatology experienced post-unilateral sinus surgery.
Our study also found that there was no statistically significant difference in contralateral NOSE scores between the 2 cohorts of individuals with 2 or fewer sinusotomies versus 3 or more sinusotomies with the exception of nasal blockage at 1 month post-ESS. In addition, both cohorts reported a decrease in contralateral congestion, blockage, difficulty breathing, and total contralateral NOSE scores from pre-ESS to 1 month post-ESS to 3 months post-ESS. Lastly, there were no differences in contralateral symptomatology between those who did and did not have septoplasty, indicating that septoplasty does not affect the development of contralateral symptoms. These results indicate that while individuals with fewer sinusotomies may more likely report worse contralateral symptoms, all individuals report an improvement in contralateral symptomatology via NOSE scores in the first few months following ESS. It is important to note that a significant portion of patients noted a worsening of contralateral CRS symptoms at the time of survey compared to before the ESS which was median time period of 24 months, as shown in Table 2. This result implies that worsened contralateral symptomatology following ESS may be temporary. Further research with data prospectively collected after the endoscopic surgery is needed to investigate this further.
A few prior studies have compared post-surgical objective outcomes between unilateral and bilateral ESS, but our study is the first to explore the degree to which individuals undergoing unilateral ESS experience contralateral CRS symptoms post-ESS and determine risk factors for contralateral symptomatology following unilateral ESS.3,9 This study is significant because the effect of unilateral ESS on contralateral symptomatology may play a role in patient education and decision-making. The fact that a significant proportion of individuals post-ESS experienced worsening of contralateral congestion, swelling, rhinorrhea, hyposmia, and difficulty breathing should be shared with patients prior to performing unilateral ESS because most would not expect the operation to affect symptoms on the opposite side. Due to our results, we have been more cognizant of alerting our patients who are going to undergo unilateral sinus surgery of the possibility that this may increase contralateral congestive symptoms. Our findings also pose the question as to whether unilateral ESS is beneficial compared to bilateral ESS in patients with unilateral CRS. If a significant portion of patients post-unilateral ESS experience worsening of contralateral CRS symptoms, perhaps it would be more beneficial to operate bilaterally originally. Further research within this field is needed to help answer this question. Future studies can also investigate whether individuals who experience contralateral symptoms after unilateral sinus surgery end up requiring medical treatment or office procedures for the contralateral side.
Our study is novel and has a number of limitations. A recall bias may exist given that NOSE scores were collected on average 24 months after unilateral ESS, which confers significant recall bias. Inquiring the participants about symptoms that they experienced approximately 2 years ago introduces room for several types of recall bias including omission, commission, and forward/backward telescoping. It is often difficult for patients to specifically remember if their right or left sinus was more bothersome since they often interpret sinus symptoms to be from both sides concomitantly. Future studies should involve prospective collection of data to reduce the recall bias noted in this present study. Additionally, prospective evaluation would permit timely evaluation of outcomes at specified time points as well as collection of data regarding the additional medical and/or surgical treatments rendered.
In addition, another weakness within our study is that our timeline of symptomatology only extends to 3 months post-ESS, which may be within the perioperative window for healing from ESS. Participants’ symptomatology experienced at that time point may only indicate the short term results of the surgery. Future studies should go beyond the 3-month post-ESS time point to understand longer-term results and effects of one-sided sinus surgery. Additionally, future studies should include objective radiographic evidence pre- and post-operation of the side operated on and the contralateral side as well in order to help justify the degree of surgery and symptoms experienced by the patient. Despite these limitations, the results of this study contribute toward a better understanding of the contralateral CRS symptoms patients can experience after unilateral ESS.
Conclusion
Unilateral ESS for CRS is not as common as operating for surgical disease; however, understanding the implications of unilateral ESS on the un-operated side is important and not well-studied. Our study is the first to investigate the degree to which patients experience contralateral CRS symptoms post-unilateral ESS and determine risk factors for contralateral symptomatology following unilateral ESS. We find that 24% of patients who had unilateral ESS for CRS experienced long-term contralateral congestion post-ESS and more than 10% of patients experienced other contralateral symptoms, including subjective swelling, rhinorrhea, difficulty breathing, and hyposmia. In addition, our study found that patients who undergo unilateral ESS for CRS and have 2 or fewer sinusotomies were more likely to report subjective contralateral CRS symptoms than individuals who undergo unilateral ESS and have 3 or more sinusotomies. Understanding the effect of unilateral ESS on contralateral CRS symptoms is essential for clinical management and patient education in cases with unilateral chronic rhinosinusitis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.