
Abstract
Horner’s syndrome is characterized by a triad of symptoms (ipsilateral miosis, ptosis, and anhidrosis) with damage of the sympathetic nervous system. The condition may be congenital or acquired from traumatic conditions including cardiovascular surgery. Horner’s syndrome can be also caused by neck trauma especially when cervical vital structures such as blood vessels, the aerodigestive tract, and nerves are disrupted. This report describes a 16-year-old woman with delayed Horner’s syndrome who initially presented with internal jugular vein injury caused by multiple penetrating stab injury to the neck. To the best of our knowledge, this is the first reported case of Horner’s syndrome resulting from neck trauma of which symptoms were presented after a couple of weeks after initial trauma. Understanding this rare clinical course may help surgeons pay attention to not only early hospital course but also long-term complications of patients with neck trauma.
Introduction
Penetrating stab injuries violating the platysma muscle can seriously damage vital structures in the neck, increasing the likelihood of patient morbidity and mortality. 1 Among various types of neck trauma-related complications, Horner’s syndrome is rarely reported since only 4–13% of Horner’s syndrome is trauma-related. 2 This syndrome was first described in animals by Claude Bernard and in humans by Johann Friedrish Horner in 1869. 3 It is known to encompass a triad of symptoms including unilateral miosis, ptosis, and anhidrosis resulting from sympathetic pathway disruption. 2 Even though these conditions are not usually associated with vision problems, clinicians should pay attention to the symptoms since it can be a warning sign of interruption of vital cervical structures. Especially if the triad of symptoms are shown after traumatic event, a patient should be assessed for potential lethal neurovascular injury by enhanced CT or CT angiography of the head and neck. Even though the majority of post-traumatic Horner’s syndromes are immediately diagnosed after traumatic event, the symptoms can be shown in a delayed manner. The present report describes a 16-year-old woman with multiple penetrating stab injuries to the neck caused by a knife attack who experienced unilateral miosis, ptosis, and anhidrosis after 14 days of trauma and initial explorative surgery.
Case Report
A 16-year-old female patient was brought to the emergency room due to multiple stab injury to the neck (Figure 1). Three sharp stab injuries were detected in zone II, one each on the left lateral, anterior, and right lateral sides of the neck, and one sharp wound was detected in zone I, on the right posterior neck (Figure 1A). At presentation to the emergency room, the patient was alert with stable vital signs but complained of a voice change without dyspnea. Photograph (A) and CT imaging (B-E) showing multiple stab injuries. (A) Stab injuries were grossly presented in zone II of the neck. CT images showed stab injuries in the left lateral neck (B), anterior neck (C), right lateral neck (D), and right posterior neck (E). Marked triangles show the trajectories of the knife blade, piercing (B) from the left anterior border of the sternocleidomastoid muscle to the visceral space, (C) from the left anterior neck to the left thyroid, (D) from the right anterior border of the sternocleidomastoid muscle to the visceral space, and (E) from the right posterior neck to the prevertebral space.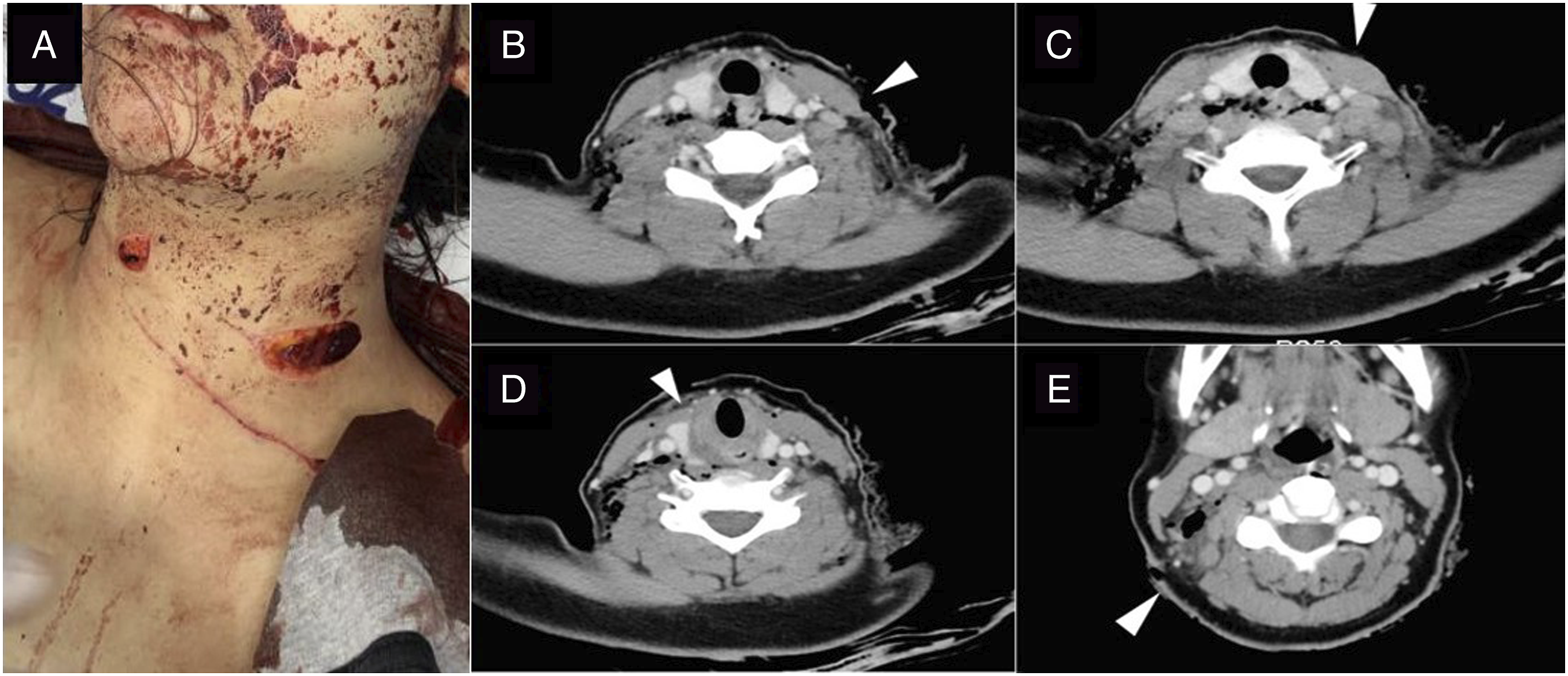
A CT scan of the neck showed the trajectories of the knife blade (1) from both anterior borders of the sternocleidomastoid muscle to the visceral space, (2) from the left anterior neck to the left thyroid, and (3) from the right posterior neck to the prevertebral space (Figures 1B-1E). A CT scan also showed neck emphysema and pneumomediastinum. Immediately after CT imaging, however, she experienced considerable hemorrhaging of the right lateral and posterior neck wounds and was transferred to the operating room for mandatory explorative surgery under general anesthesia. The right external and internal jugular veins had been damaged and were ligated, but other vital structures including carotid artery, vertebral artery, and aerodigestive tract were intact.
A CT scan showed mucosal defect signs on both sides of the esophagus, suggesting perforations on both sides of the cervical esophagus (Figure s2A-2C). The elevated WBC count and CRP concentration and neck swelling suggested that wound infection with abscess formation had progressed around the perforation sites so that a second operation was performed immediately. The rupture site on the right side of the esophagus was found to be an inverted V-shaped wound, about 4 cm in size, and the rupture site on the left side was about 2 cm in size (Figure 2D and 2E). The wound on the left side was closed, whereas the wound on the right side was debrided of some necrotic tissue, followed by primary repair. CT images showed esophageal perforations on both sides (A and B, axial view; C, coronal view). The right esophageal rupture site was an inverted V-shaped wound with relatively irregular margins and inflammation (D). The left esophageal rupture site was a wound about 2 cm in size with clear margins and mucosal eversion (E).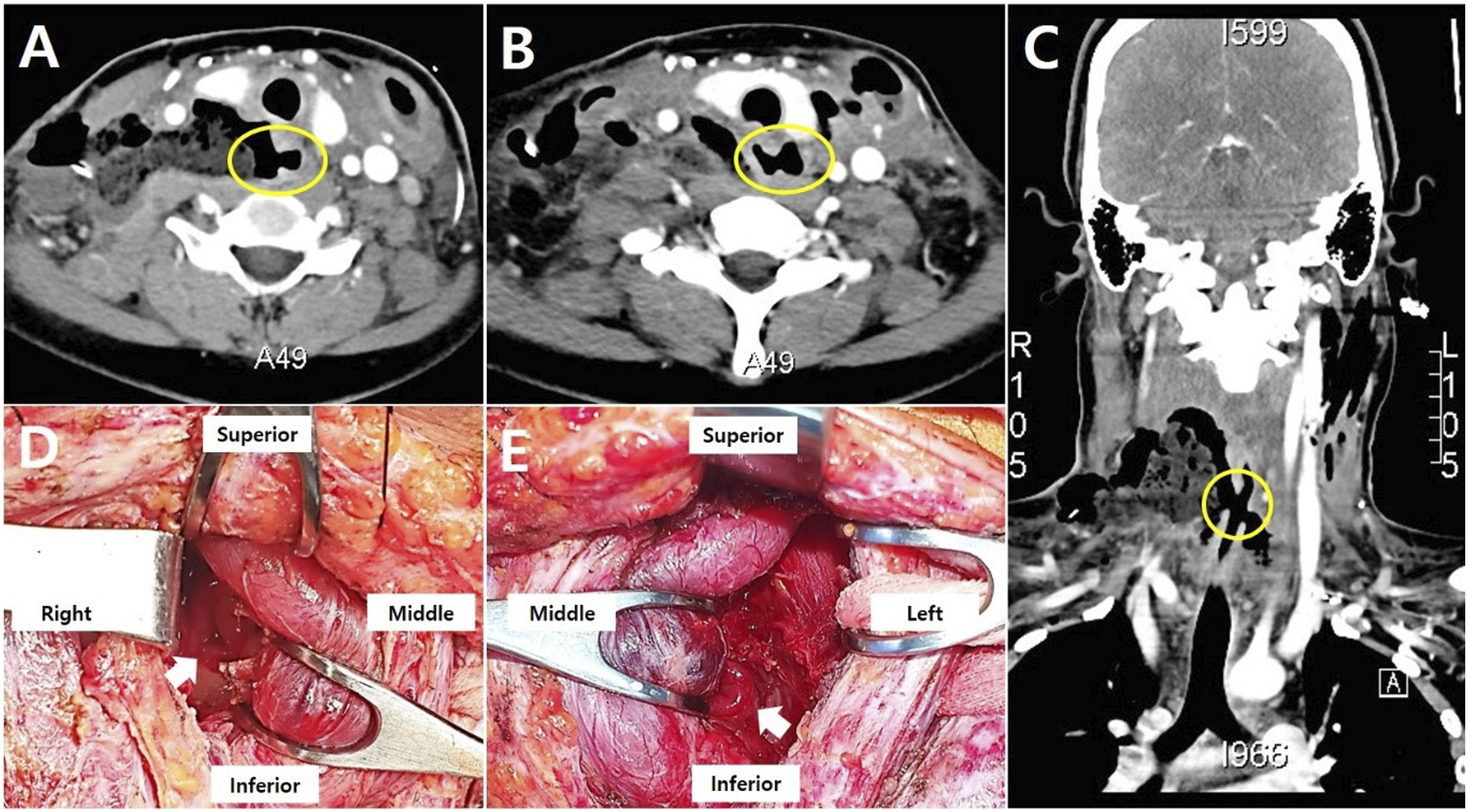
After esophageal recovery was confirmed, bilateral vocal fold paralysis with both vocal cords fixed in a paramedian position was found in laryngoscopic examination (Figure 3A). Because the patient did not experience respiratory difficulty during bed rest, extubation was done without tracheostomy. On the 14th hospital day, right-side ptosis and miosis were newly identified (Figure 3B and 3C). She was diagnosed with Horner’s syndrome based on possible injury to the right-sided sympathetic pathway due to the posterior penetrating wound. There was no visual disturbance on ophthalmic examination. Since additional damage on vital structures in the neck which might cause Horner’s syndrome was not found on follow-up CT scan, the patient was observed without further intervention. At the 3 month outpatient follow-up, the clinical symptoms were still present, but she did not report any difficulties in daily life at home and in school. At last follow-up, 6 months after discharge, the patient fully recovered from Horner’s syndrome without any other interventions. Bilateral vocal fold paralysis, showing both vocal cords fixed at the paramedian position (A). Photographs of the patient, showing right-sided ptosis and miosis, along with Horner’s syndrome (B and C).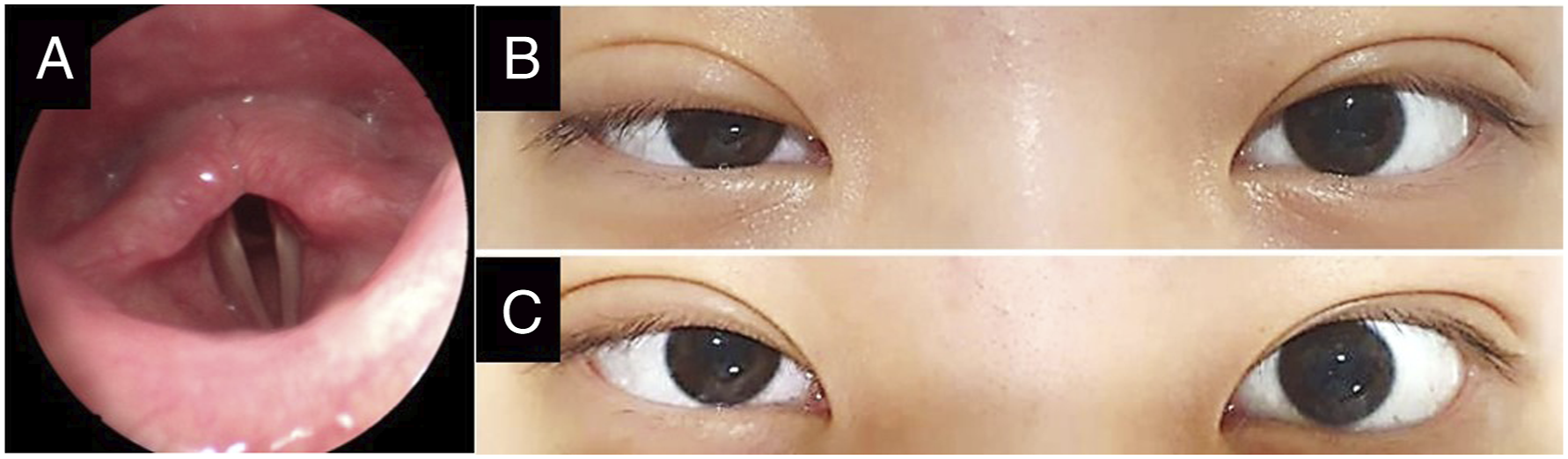
Discussion
Horner’s syndrome is an uncommon clinical state which usually presents with the triad of symptoms including ipsilateral miosis, ptosis, and less commonly, anhidrosis. The most frequent etiology resulting in Horner’s syndrome is tumor related (35–60%), while trauma-related Horner’s syndrome is relatively rare (4–13%). 2 If the symptoms of Horner’s syndrome are shown after either blunt or penetrating cervical trauma, it is essential to evaluate the damage to sympathetic chain. The sympathetic chain responsible for physiological regulation over various body processes includes three neuron systems. To be more specific, the first neurons descend from the hypothalamus to the spinal cord level C8-T2, the second neurons synapses in the superior cervical ganglion, and the third neurons innervates into the skull and the eye.2,3
In order to evaluate the disruption of sympathetic nervous system causing Horner’s syndrome and related major vascular injury, head and neck enhanced CT or CT angiography should be firstly considered. In this current case, right external and internal jugular veins as well as esophagus were damaged by penetrating neck injury. After the vessel ligation and esophagus repair, the patient was well-recovered. However, the triad of symptoms of Horner’s syndrome, miosis, ptosis, and anhydrosis on her left side of face was shown after 14 days of initial cervical trauma and the surgery for vessel ligation.
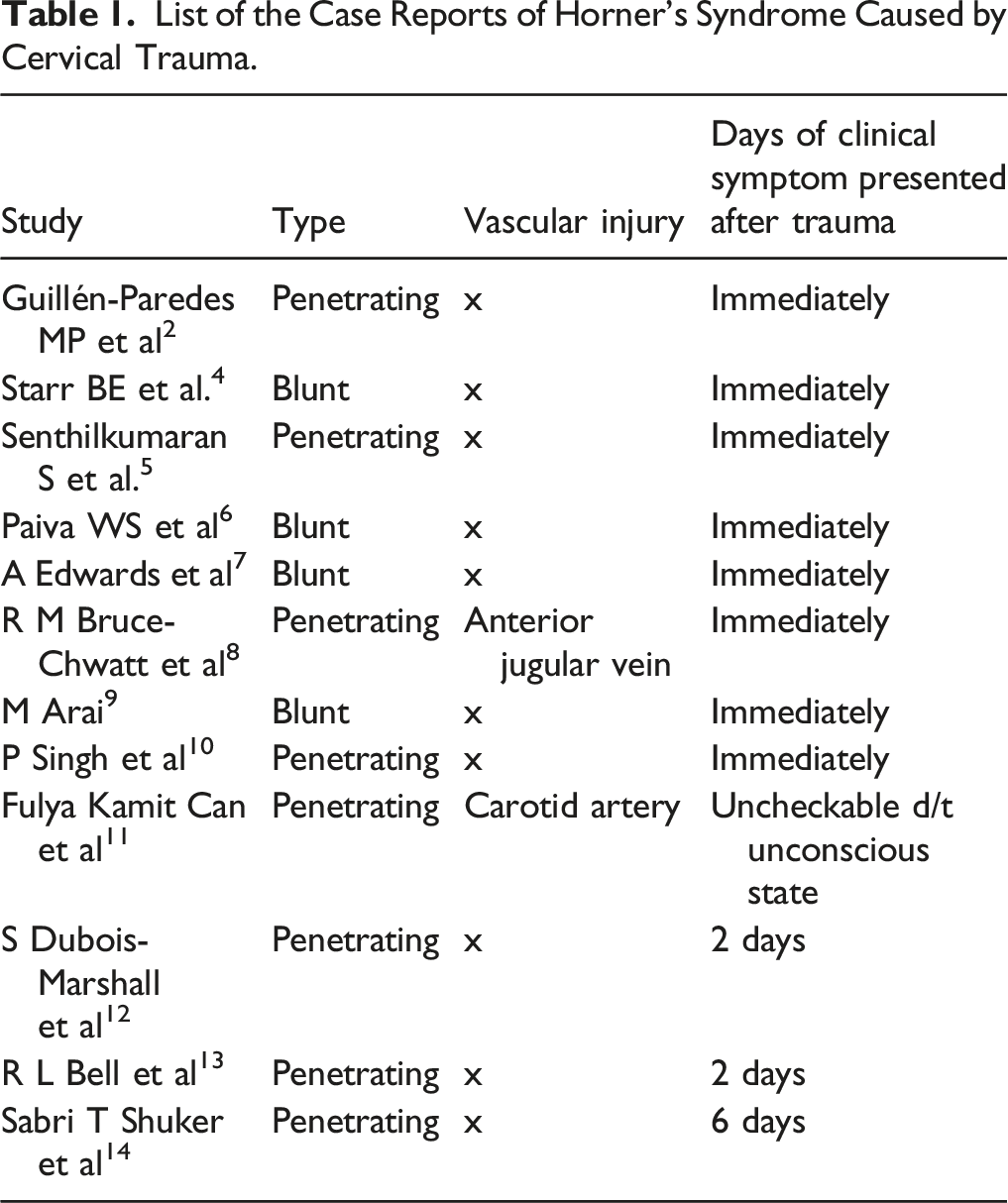
List of the Case Reports of Horner’s Syndrome Caused by Cervical Trauma.
As our case showed no further vascular injury during the two weeks of postoperative course, we hypothesize the damage to sympathetic damage might be caused by postoperative tissue edema and its compression effect. The patient luckily obtained complete recovery from the clinical symptoms of Horner’s syndrome with conservative management because there was no additional injury on vital structures when Horner’s syndrome was diagnosed. In conclusion, clinicians should take a look at the presence of Horner’s syndrome during not only early hospital stay but also long-term follow-up because delayed surgical approach including wound exploration may be required.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.