
Abstract

We cared for a 59-year-old female smoker who presented with a supraglottic lesion mimicking a laryngeal saccular cyst. The lesion was found to be a oncocytic papillary cystadenoma. This is a rare, benign neoplasm that accounts for 2–4.7% of minor salivary gland neoplasms. Oncocytic papillary cystadenoma of the larynx is even more rare, compromising less than 1% of all benign laryngeal neoplasms. This case highlights the importance of comprehensive differential diagnosis for cystic laryngeal lesions.
A 59-year-old female with dysphonia presented to an otolaryngologist. She described a raspy quality to her voice that had been present for several months and progressively worsening. She had a 40-year pack smoking history. She denied shortness of breath, dysphagia, odynophagia, neck masses, and weight loss, and she had no history of head and neck cancer. Physical examination was unremarkable. Flexible laryngoscopy and videostroboscopy revealed a large, submucosal, left supraglottic, cystic-appearing lesion obstructing the left anterior glottis (Figure 1). The patient’s vocal folds were mobile, and no other abnormalities were noted. Pre-operative image of supraglottic cystic lesion (A) taken with flexible videostroboscopy; (B) Epiglottis; (C) True vocal folds.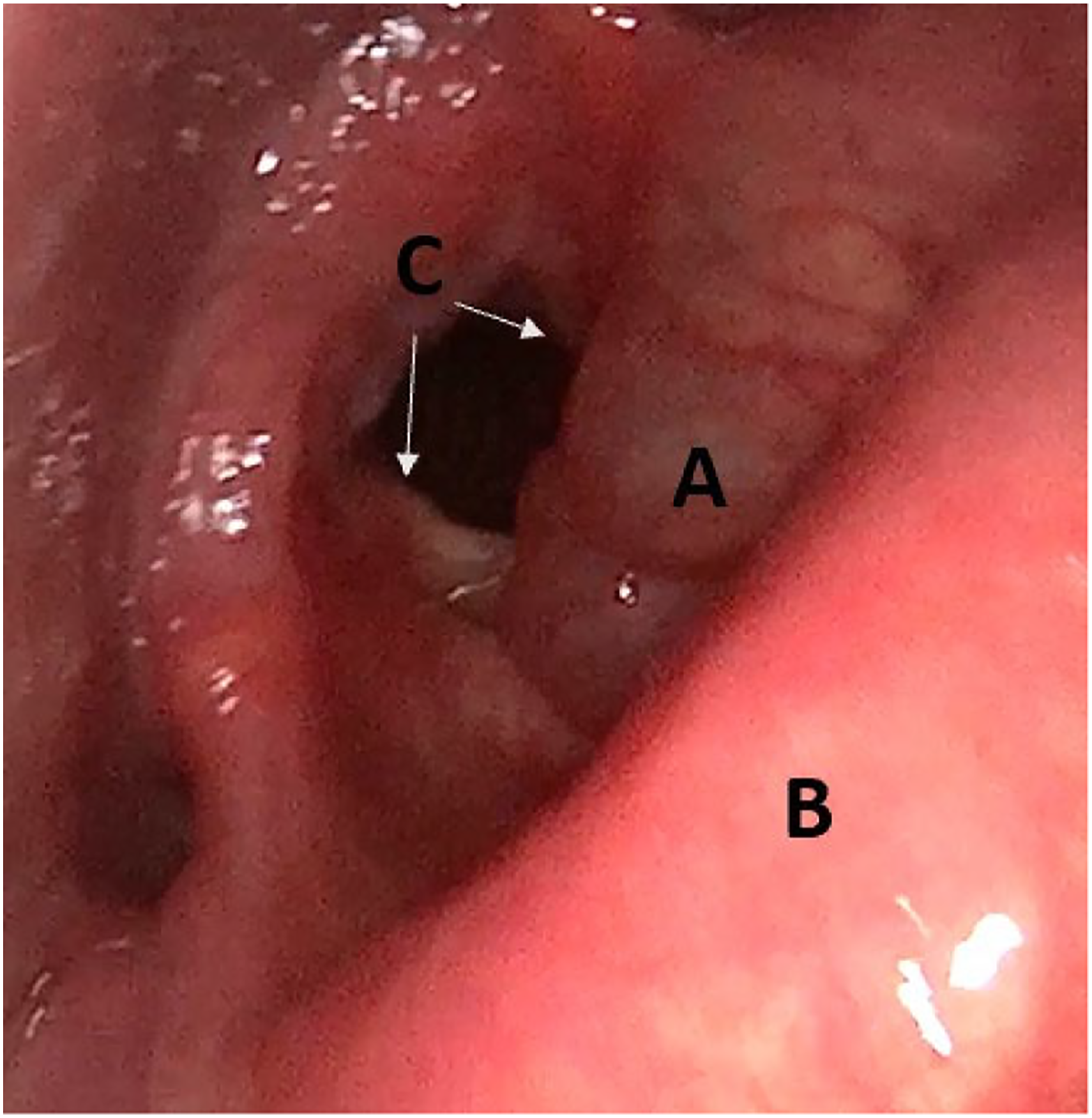
In-office ultrasound revealed an approximate 3 cm cystic lesion extending from the left glottis to the left supraglottis confined within the thyroid lamina with no apparent thyroid cartilage invasion. (Figure 2). There was no cervical lymphadenopathy. Ultrasound image of (A) left laryngeal cystic lesion at level of the glottis; (B) Thyroid cartilage; (C) true vocal folds.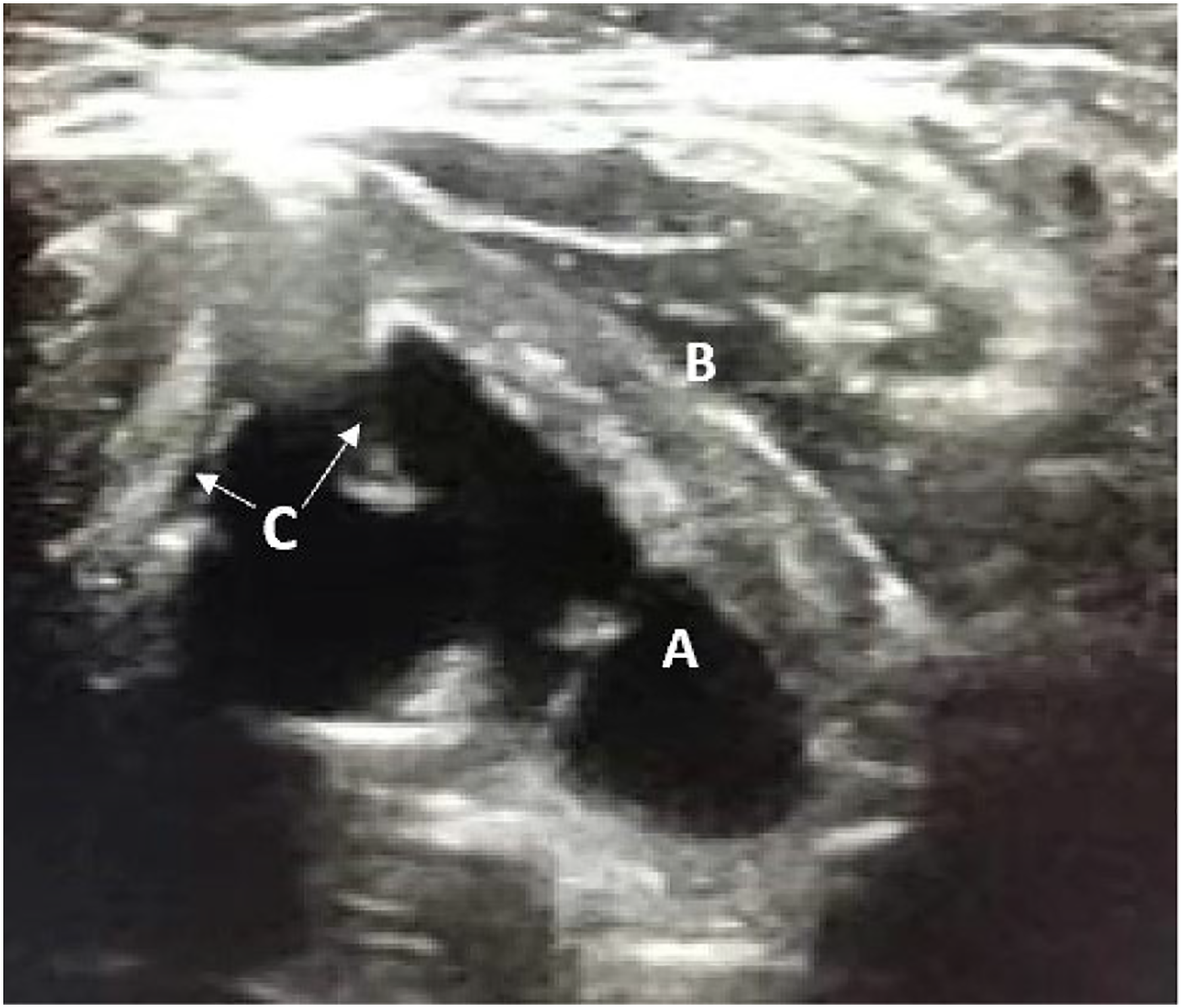
Computed tomography with IV contrast of the neck showed a 2.9 cm left supraglottic mass involving the left aryepiglottic fold and extending into the left paraglottic fat, as well as a component within the left lateral pharyngeal wall (Figure 3) Computed tomography with IV contrast of the neck in axial (a) and sagittal (b) view. (A) Supraglottic mass. (B) Thyroid cartilage. (C) Petiole of epiglottis. (D) Vallecula.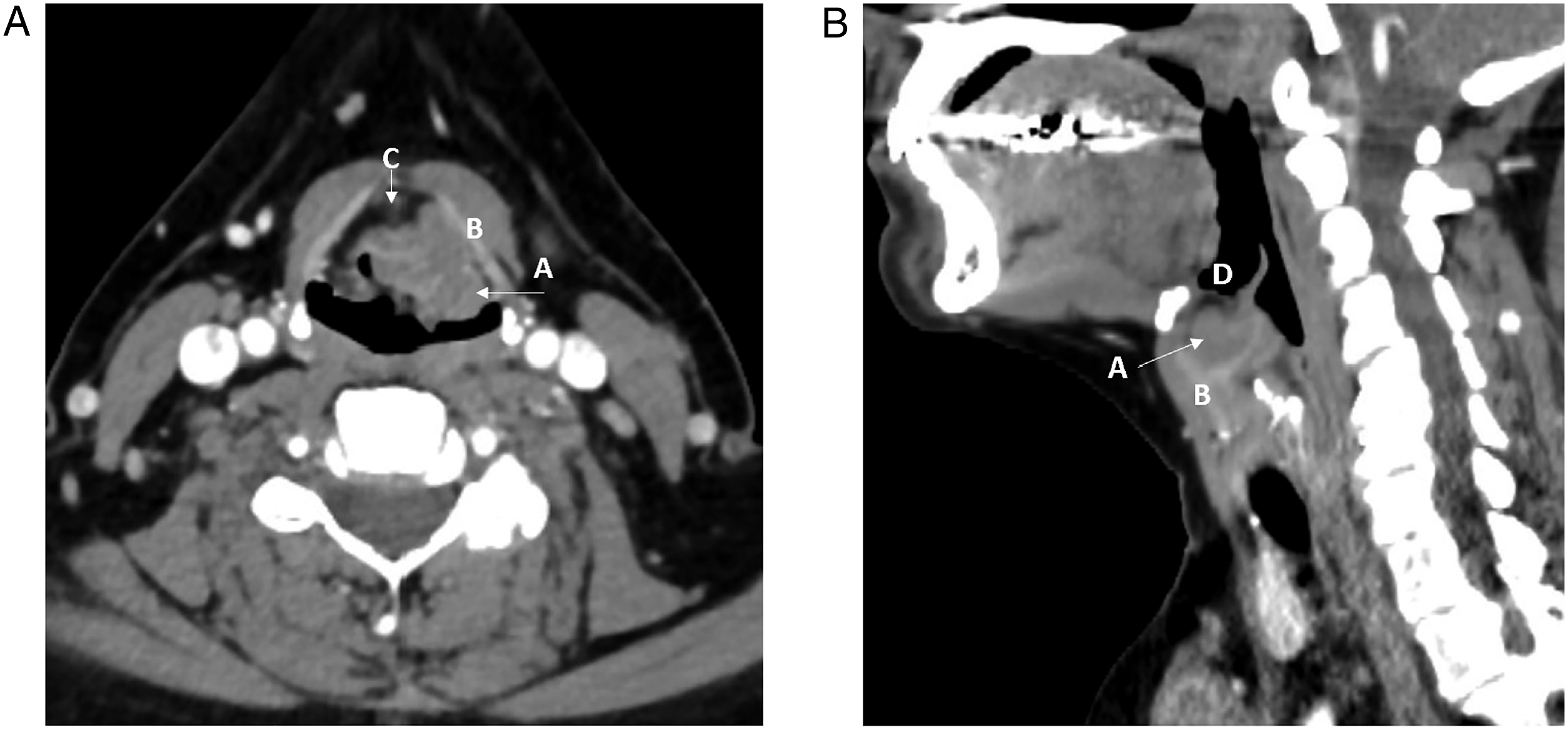
The patient was taken to the operating room for direct laryngoscopy and excision of the laryngeal lesion. Intraoperatively, a large submucosal cystic lesion emanating from the left laryngeal ventricle and extending to the supraglottis confined within the thyroid lamina was excised in its entirety via a transoral endoscopic approach. Pathology showed cystic oncocytic proliferation with papillary infoldings within the submucosa, consistent with a oncocytic papillary cystadenoma. Postoperatively, the patient did well, and she complained of mild, but improved, hoarseness. She continued to smoke.
Cystadenoma, more commonly referred to as oncocytic cystadenoma, is a type of cystic adenoma arising in salivary gland tissue. It is an extremely rare benign tumor and accounts for 2–4.7% of all minor salivary gland neoplasms. 1 Cystadenomas are divided further into papillary and mucinous subtypes. Typically, they are composed of glandular and cystic structures, often with a papillary cystic configuration, and they are lined by an epithelial bilayer comprised of oncocytes and basal cells. They closely resemble Warthin’s tumors (papillary cystadenoma lymphomatosum) but lack the lymphoid element. 2 Oncocytes are large, irregularly shaped cells, with eosinophilic cytoplasm rich in mitochondria. The incidence of oncocytic metaplasia in salivary glands increases with age. 3
Oncocytic cystadenomas most commonly affect females (2:1 ratio of females to males) in the 7th–8th decade. 4 Similar to Warthin’s tumors, smoking is considered a risk factor for the metaplastic cellular changes resulting in oncocytic cystadenomas. 5 The most frequent presentation of a salivary oncocytic cystadenoma is a painless submucosal mass of the palate, lip or buccal mucosa. 2
In the larynx, they are much more rare, representing less than 1% of all benign laryngeal tumors 5 . The majority of laryngeal oncocytic cystadenomas occurs in the supraglottis, more specifically the ventricle and false folds in which minor salivary gland tissue is most dense. 6 They most commonly present as a single lesion, but occasionally they are diffuse or multifocal. Hoarseness is the most common symptoms; and if large enough, they can cause airway obstruction. 7
Surgical excision with clear margins is the standard treatment for laryngeal oncocytic cystadenoma, typically by means of transoral endoscopic technique.1,2 Endoscopic CO2 laser excision is being utilized increasingly. 3 Open surgical excision may be considered if the neoplasm is extensive or recurrent.5,7 No adjuvant treatment is recommended. 7 Recurrence is rare but has been reported and is thought to be due to incomplete surgical excision.2,5 While oncocytic cystadenomas are benign tumors, a case of laryngeal carcinoma arising within an oncocytic cystadenoma has been reported. 8 Regular follow-up is recommended.1-3,7
Although rare, oncocytic cystadenoma should be considered in the differential diagnosis of any cystic-appearing laryngeal mass, especially in elderly female smokers. In our case, given that the in-office ultrasound revealed largely cystic lesions, laryngeal saccular cyst and mucolaryngocele were at the top of our differential diagnosis. For that reason, surgical marsupialization was considered as an option intraoperatively. Retrospectively, complete surgical excision was the preferred surgical approach, as risk of recurrence and need for re-excision would have been heightened with marsupialization alone. Salivary gland pathology such as oncocytic papillary cystadenoma should be considered in the differential diagnosis of a supraglottic cystic-appearing mass. Complete surgical excision is curative, but regular follow-up is recommended because incomplete excision (possibly unrecognized) can lead to recurrence.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.