
Abstract
Reinke’s edema and variceal hemorrhage are complex structural pathologies that affect the vocal cord mucosa. The vocal cords are highly susceptible to environmental stressors, such as smoking and vocal cord usage, thus, treatment involves their corresponding cessation.1 Here, we report a case of a patient with severe Reinke’s edema and bilateral chronic vocal cord varices. The patient had a 30-pack-year history of cigarette smoking and was obstructed with intubation due to acute variceal hemorrhage and severe swelling of Reinke’s edema. Moreover, a review of the literature regarding Reinke’s edema and variceal hemorrhage treatment and their complications was performed.
Introduction
Reinke’s Edema occurs as a result of chronic edematous submucosal swelling located in the Reinke's space that can affect one or both of the vocal cords and is usually due to cigarette smoking, alcohol, and vaping. 1 This is a benign laryngeal condition caused by swelling in the lamina propria and can have up to a 3% chance of malignant dysplasia.1,2 We now report a case of a 56-year-old female cigarette smoker who presented with severe Reinke’s Edema and bilateral varices of the vocal cords.
Case Presentation
A 56-year-old female presented with worsening hoarseness and a 30-pack-year history of cigarette smoking. The patient’s hoarseness was worsening over the last 6 months. The patient had mild shortness of breath, potentially due to her inadequate exercise regimen and long history of cigarette smoke. Before conducting a laryngoscopy, the patient had a full preoperative clearance due to her smoking history and was subsequently referred to a hypnotherapist to assist with smoking cessation.
On video strobolaryngoscopy, the patient had large polyps and varices on the right and left vocal cord and was sent to speech therapy for assessment (Figure 1). The patient requested that the polyps be removed due to the negative effect they had on her daily activities. Thus, the preoperative plan was to remove the right polyp and possibly the left polyp, which would be determined intraoperatively. A laser endotracheal tube would be used to allow KTP laser of the varices. On video strobolaryngoscopy, the patient had large polyps and varices on the right and left vocal cord.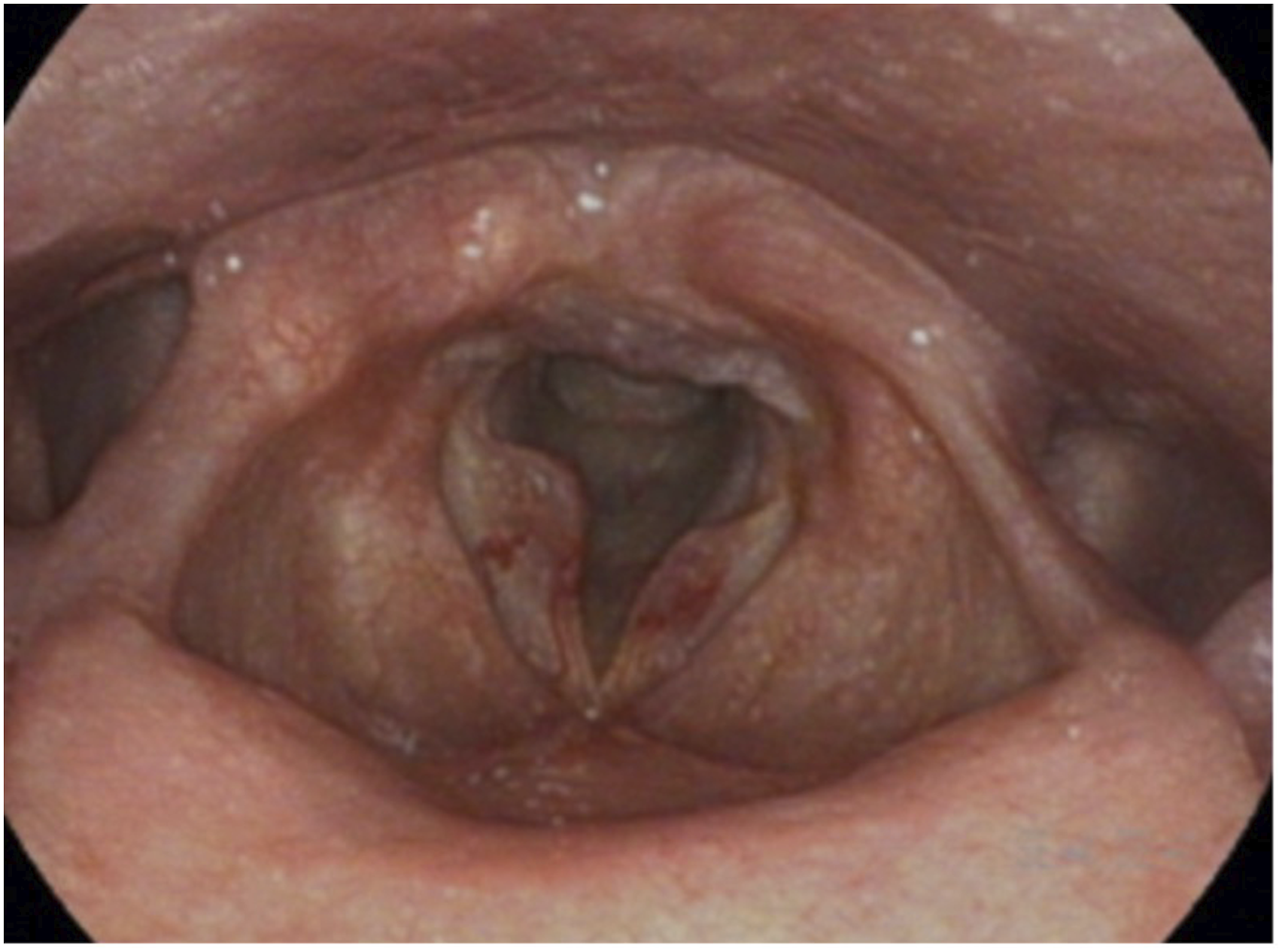
Intraoperatively, the patient was intubated successfully on the first attempt with an endotracheal tube under direct Kantor Berci video-laryngoscopy visualization by an experienced thoracic anesthesiologist. As soon as the laryngoscope was suspended, it was evident that there was no airway present due to acute hemorrhage of the bilateral varices and substantial acute swelling of Reinke's edema (Figure 2A). Additionally, the polyps were overlapping the 6.0 laser endotracheal tube, resulting in no visible glottic/subglottic airway. (A). Acute hemorrhage of the bilateral varices and substantial acute swelling of Reinke’s edema. (B). Softening of hemorrhage with a 75% airway improvement after additional right sided resection and steroids were given.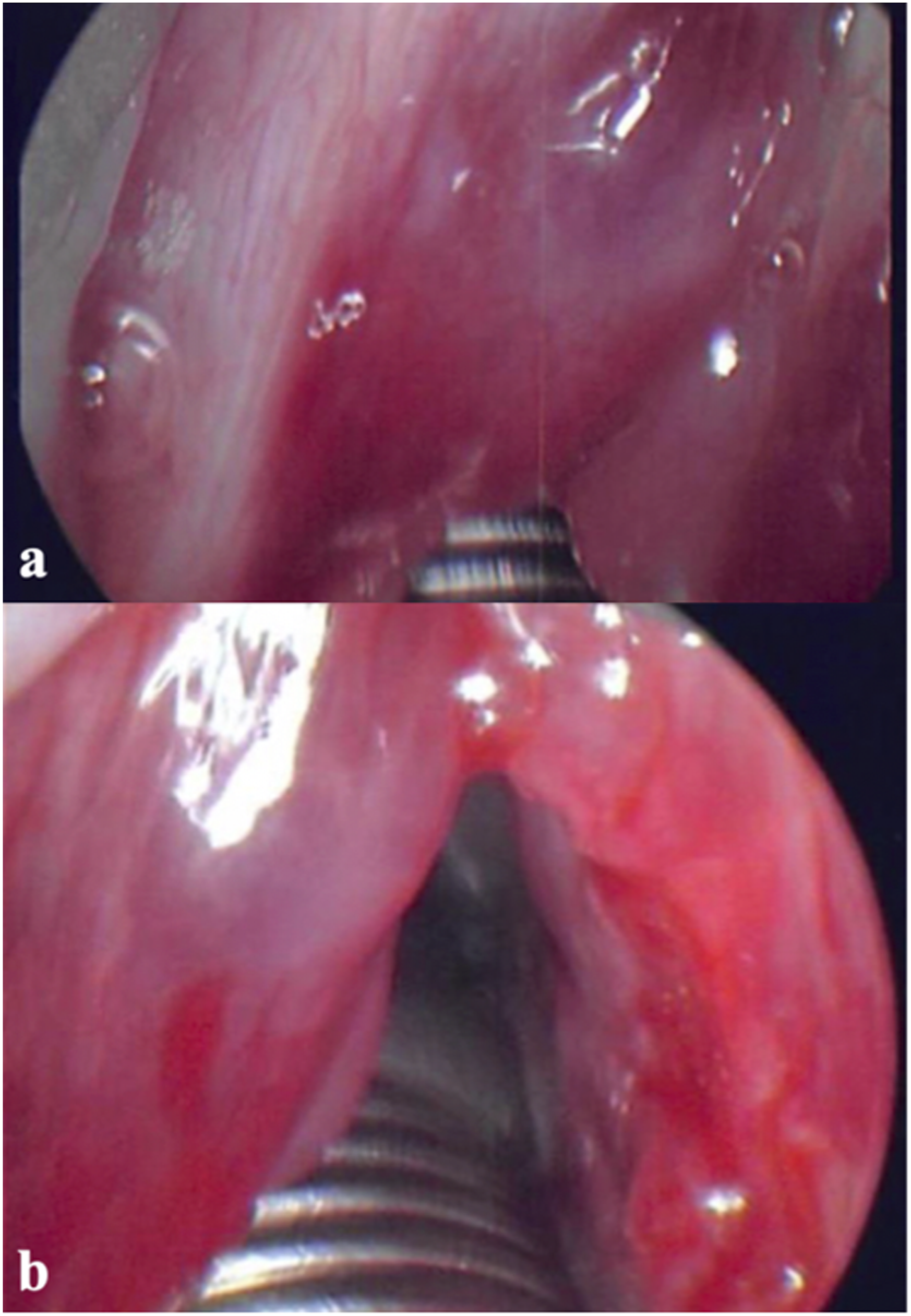
During the procedure, the edematous right vocal cord polyp was removed via sharp dissection, but there was still edema and hemorrhage present in the area causing poor visualization of the airway. After 30 minutes of dissection, there was still no visible airway present. Thus, the patient was left intubated overnight. The anesthesiologist felt that it was too great of a risk to replace the laser endotracheal tube, as the airway was swollen and bloody, and replacement of the tube may have resulted in the loss of airway. The patient was placed on steroids and prophylactic antibiotics, as well as IV H2 blockers.
On the following day, the patient was given additional steroids and was taken to the operating room for direct laryngoscopy. Upon suspension, it was apparent that the hemorrhage of the left vocal cord had softened, and the airway had a 75% improvement. The patient was then extubated in the operating room (Figure 2B).
On laryngoscopy after 18 hours postoperatively, it was seen that the vocal cords were improving, but there was post-glottic irritation present from the laser endotracheal tube (Figure 3A). On postoperative day 4, there was post-glottic irritation present from the last tube that persisted (Figure 3B). Two weeks after the surgery, the area of posterior irritation showed signs of mild vocal cord granuloma/granulation, but the patient was doing better symptomatically, even with the persisting left vocal cord polyp. She was maintained on a PPI and an H2 blocker, as well as an acid reflux diet. (A). Laryngoscopy 18 hours postoperatively with laser ridges present. (B). Laryngoscopy 4 days postoperatively with the last ridges still present.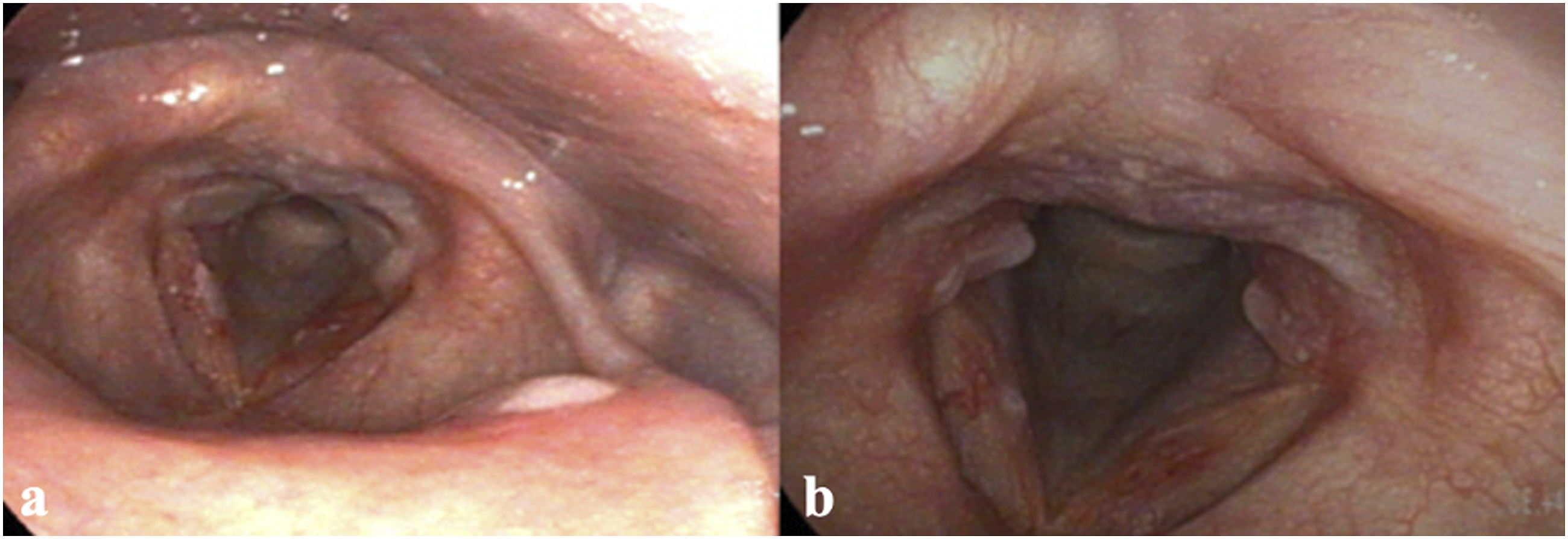
Discussion
Reinke’s edema is a benign structural pathology of the mucosal folds that include the expansion of the vocal cord subepithelial region. 1 Tobacco use is the main risk factor for developing Reinke’s edema and can be affected by the length and amount of smoking, as well as frequent and excessive alcohol use. According to a study conducted by Marcotullio et al., the histological classification of 64 patients showed that a longer duration of cigarette smoke exposure correlated with higher degrees of damage and increased severity of lesions. 3 Additionally, an in-vitro study found that specific genes, when associated with the combination of cigarette smoke and vocal cord vibration, had greater effects on the pathophysiology of Reinke’s edema. 4 We believe that this patient’s edema did not occur as a direct result of the type of endotracheal tube used but due to her persistent smoking before the procedure, which led to hemorrhage and inflammation of the vocal cords during intubation. Thus, to prevent the exacerbation of Reinke’s edema, we recommend that the patient remain on voice rest for 7 to 10 days and stops smoking 6 weeks before the procedure.
Correspondingly, there are a few treatment modalities that have been presented in the literature as effective management for Reinke’s edema. In a study of 44 patients, steroid injections to the vocal cords were shown to present a significant improvement in mild Reinke’s edema. 5 Furthermore, stripping of the vocal cords is an aggressive approach that can result in vocal cord complications (sulcus vocalis) but is thought to increase airway diameter and improve the voice. According to Nielsen et al., in an assessment of 120 patients who underwent vocal cord stripping, 81% of patients presented with vocal issues, 68% presented with hoarseness, and 58% of patients had Reinke’s edema recurrence. 6 Thus, it was determined that the curative effect of limited vocal cord stripping is minimal, and the mainstay conservative treatment for Reinke’s edema is the elimination of environmental factors such as smoking and vocal abuse. 6
Moreover, vocal cord varices are at increased risk for hemorrhage and can be asymptomatic and difficult to diagnose. Vocal cord varices had a 10 times increased risk for hemorrhage compared to those without varices. 7 A study done by Lennon et al. found that 26% of patients with vocal cord hemorrhage had a recurrence, but there was a 48% increased chance of developing hemorrhage recurrence in patients with corresponding varices. 8 Treatment of vocal cord hemorrhage includes corticosteroids and phonosurgical interventions, with surgery showing to be the most effective modality. 9
Conclusion
Reinke’s edema is a multifaceted condition that is thought to occur due to smoking and vocal cord usage, though a literature search shows that most of the pathophysiology is still not understood. Treatment of this condition has multiple approaches, with some methods resulting in significant complications to vocal cord function. Therefore, a combination of surgical therapies and environmental factors is crucial in the treatment of Reinke’s edema and the prevention of its recurrence.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Submission Statement
This manuscript is original and has not been submitted elsewhere in part or in whole.