
Abstract
Cholesteatomas are non-neoplastic, invasive lesions created by the accumulation of keratinized squamous epithelium in the temporal bone. If left untreated, its expansion may cause local destruction of the surrounding structures, eventually leading to inner ear fistula, dehiscence of tegmen and possible intracranial pathology, and facial nerve paralysis. Surgical resection is the mainstay of curative treatment. We hereby present a case of a giant cholesteatoma in a 62-year-old patient who presented with a right-sided hemifacial spasm with later paralysis who was treated with botulinum toxin injection by a neurologist. CT scan imaging showed a very large cholesteatoma with involvement of the carotid canal, cochlea, and geniculate ganglion. The patient underwent transmastoid and subarcuate approach for resection which led to marked improvement of her symptoms.
Keywords
Introduction
A cholesteatoma consists of keratinizing squamous epithelium in the temporal bone which may produce significant amounts of keratin debris. Its expansion may cause local destruction of surrounding structures. 1 A cochlear fistula is a very uncommon form of inner ear fistula that may arise in the presence of cholesteatoma. 2 The incidence rate is estimated to be about 0.1–2.9%, with most of these arising from the pars tensa. 3 Unfortunately, cochlear fistulas are associated with a poorer functional prognosis when compared against those of other locations. 1 This causes significant patient morbidity, with a significant number of patients presenting with deafness at the time of diagnosis.
Case Report
A 62-year-old woman presented to the otology outpatient clinic with a 2-year history of facial spasms, treated with intramuscular botulinum toxin. The patient presented to our center with a 6-month history of right-sided facial paralysis with associated severe right-sided hearing loss. On examination, the patient had a grade 5/6 facial function. On her physical exam, the tympanic membrane was collapsed with dense keratin debris filling the middle ear. Her audiogram showed mixed hearing loss, with a word recognition score of 52% on the right. On the right, thresholds at frequencies of 0.5, 1, 2, and 4 kHz for air conduction were 80, 80, 70, and 80 dB, respectively. The bone conduction thresholds were 45, 50, and 50 at 0.5, 1, and 2 kHz. The Weber test with the 128 and 512 Hz tuning fork lateralized to the right.
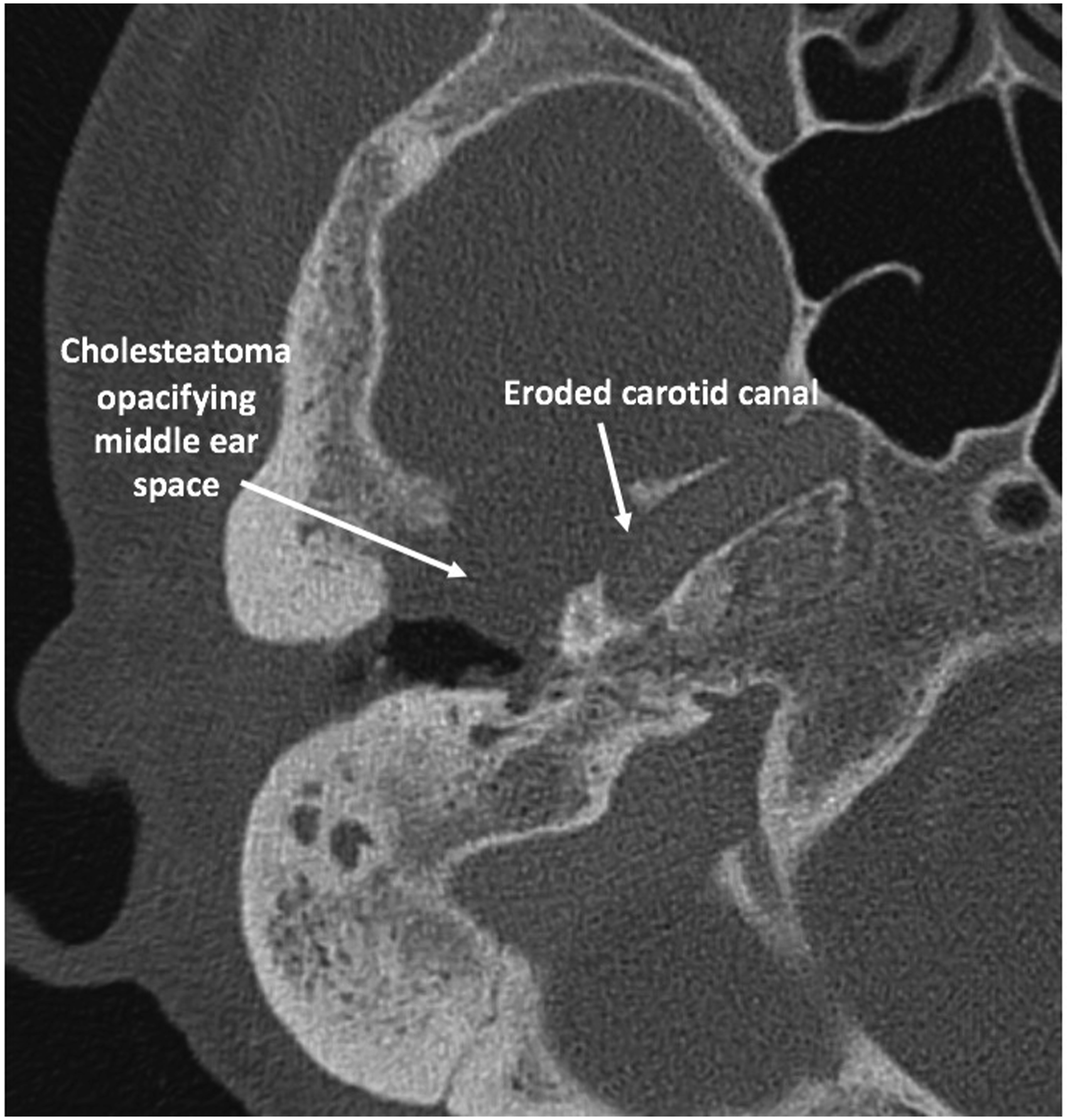
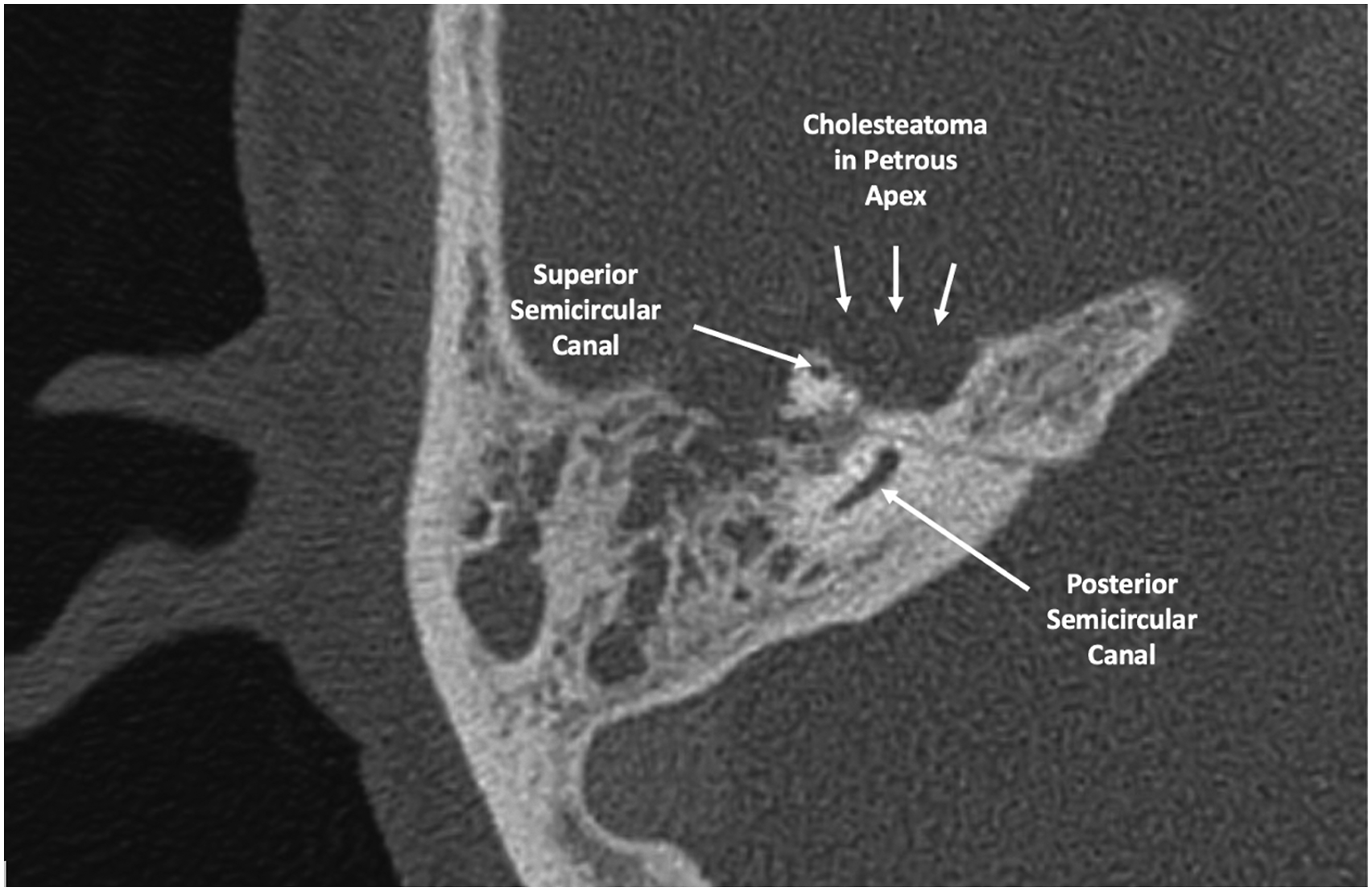
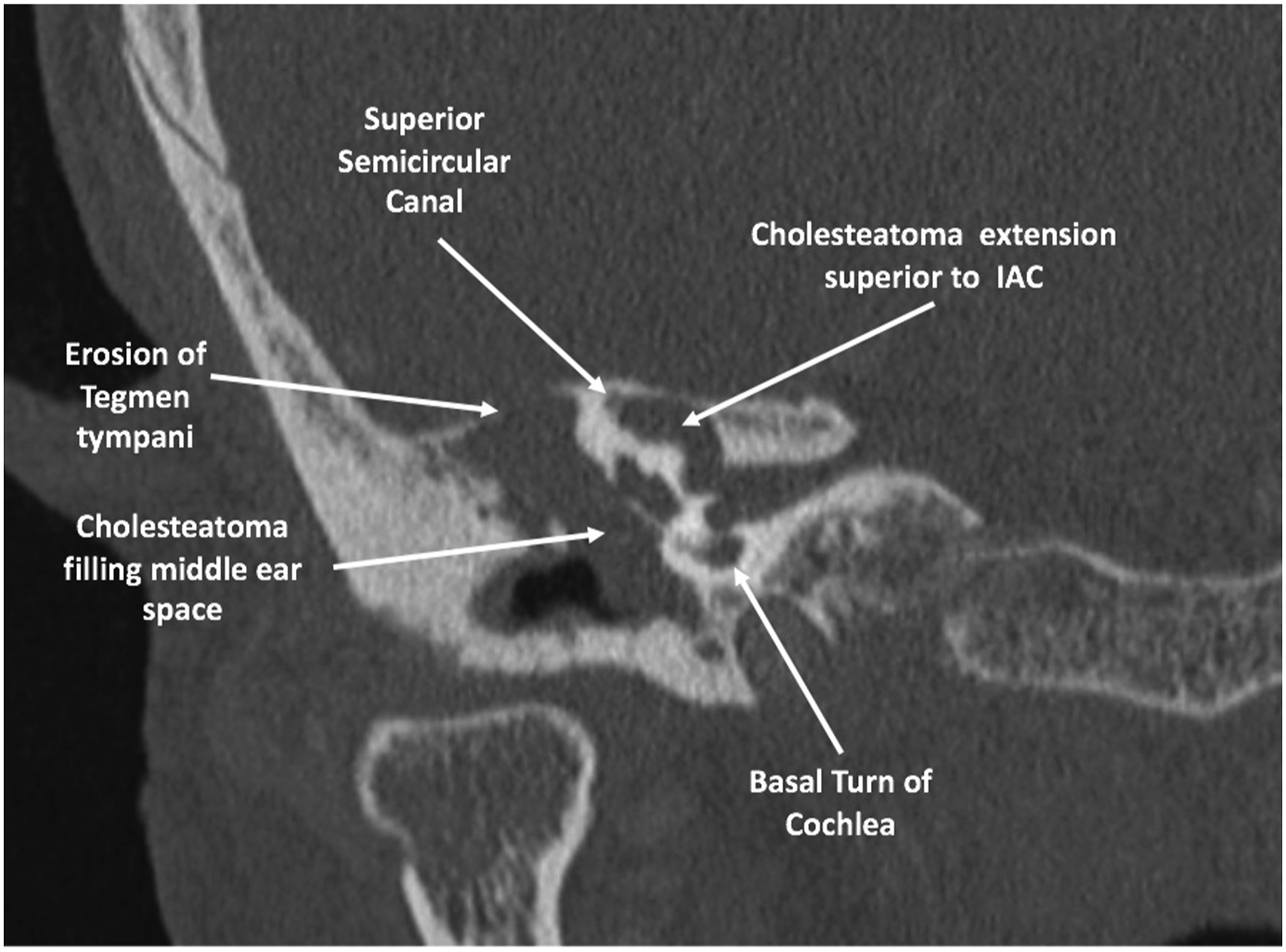
The CT scan of the right temporal bone revealed a large mass opacifying the middle ear space, eroding the apical cochlea, the horizontal semicircular canal (HSC), tegmen tympani, temporomandibular joint (TMJ), and carotid canal, and extending above the internal auditory canal (IAC). There was also an involvement of the region of the geniculate ganglion. This cholesteatoma was also tracked as far medial to the superior semicircular canal. (Figures 1‐4) (A) Axial CT of the right temporal bone demonstrating the cholesteatoma opacifying the middle ear space and eroding the apical cochlea. (B) Axial CT of the right temporal bone showing the cholesteatoma eroding the horizontal semicircular canal. Also note involvement of the region of the geniculate ganglion, which likely contributed to the patient’s facial paralysis. Axial (horizontal) CT of the right temporal bone demonstrating erosion of the horizontal portion of the carotid canal by cholesteatoma. Axial (horizontal) CT of the right temporal bone demonstrating erosion of the petrous apex by cholesteatoma. Coronal CT of the right temporal bone demonstrating extension of cholesteatoma over the right internal auditory canal medial to the superior semicircular canal. Also, note erosion of the tegmen tympani.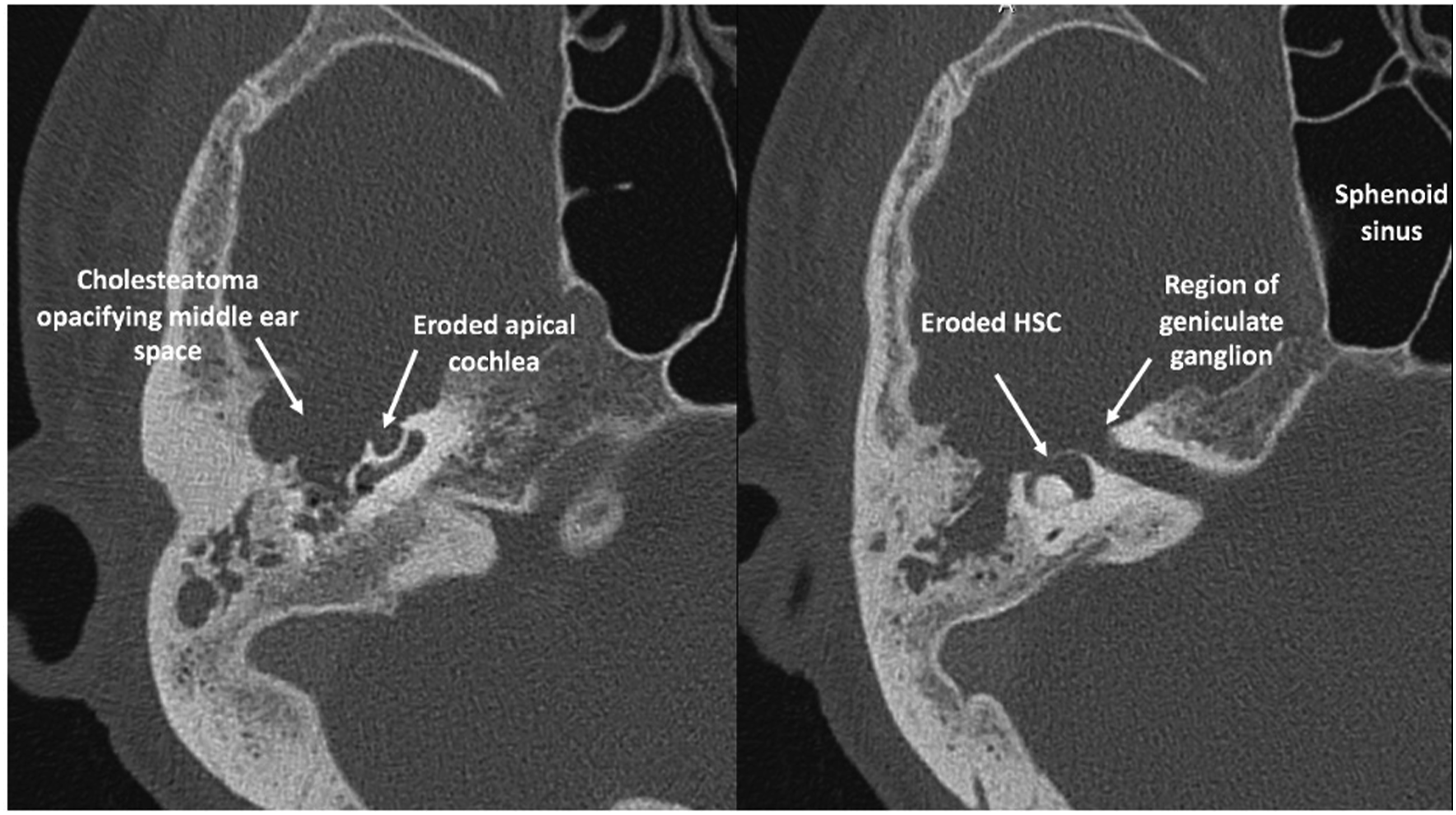
Because there was involvement medial to the labyrinth, exteriorization alone was not the best approach for this patient. As a result, surgery was performed through a canal wall down tympanomastoid approach. Portions of the canal wall were removed to have full access to the cholesteatoma which was separated from the cochlea and the carotid. The area was later reconstructed with cartilage and bone pate. A subarcuate approach was done to reach the medial aspect in the petrous apex and extirpate disease medial to the superior semicircular canal. An autologous fat graft was placed in the middle ear to repair a minor CSF leak in the lateral aspect of the internal auditory canal. The carotid artery was also covered with fat to prevent aeration and subsequent desiccation. The mass was successfully separated from all areas of fistulas and dehiscence, and the cochlea was covered with fascia. The patient had preserved hearing in the right ear immediately post-operatively on bone conduction testing in the recovery room using a 512 Hz tuning fork Weber test. However, at the subsequent follow-up, the audiometric test showed profound sensorineural hearing loss with a no response in the speech awareness threshold on the right. The Weber test with 128 and 512 Hz tuning forks lateralized to the left. On examination, the patient had a grade 5/6 facial function with no perceptible motion other than a mild flicker of the right nasalis.
Discussion
We present a case of a complex, extensive cholesteatoma involving the facial nerve, carotid artery, internal auditory canal, petrous apex, and the cochlea. Cholesteatomas of this extent are rare in the modern era as access to otolaryngology is available in many countries in the world. The extent of the cholesteatoma also indicates the importance of treatment, as continued expansion of cholesteatoma can lead to silent expansion until critical structures are involved. In this patient, the hemifacial spasm was managed primarily by a neurologist who never obtained imaging or performed an otologic examination. The cholesteatoma was quickly diagnosed when the patient developed facial paralysis and was referred to an otolaryngologist. An MRI with and without gadolinium must be obtained to evaluate patients with hemifacial spasm as the spasms could be a harbinger of an underlying mass. Some patients demonstrate facial weakness in conjunction with spasms. This phenomenon can be seen in cholesteatoma involving the facial nerve, facial schwannoma, and Lyme disease. A thorough workup of facial spasms must be undertaken in parallel with treatment.
Various approaches in a giant cholesteatoma such as this may be undertaken. The first approach is to perform a radical mastoidectomy. In this procedure, the cholesteatoma is entirely exteriorized, the tympanic membrane is removed, and the eustachian tube is plugged. In a patient like the one, disease would be left behind on the facial nerve, petrous apex, and carotid artery. This may cause expansion of hidden pockets of the cholesteatoma, which are not fully exteriorized. An inadvertent aggressive suctioning on the carotid artery in clinic can potentially have adverse consequences.
A second approach to a giant cholesteatoma is to resect the cholesteatoma with canal overclosure. This approach risks leaving disease behind which can recur. In a complex case such as this, with involvement of the carotid, it may not be feasible to fully dissect cholesteatoma off the artery. Therefore, the decision to perform canal overclosure cannot be made until that disease has been dissected.
A third potential approach in a patient such as this one is to perform a translabyrinthine with possible transcochlear approach to resect all potential disease. This patient has poor hearing and large openings in the cochlea, which will generally lead to further loss of hearing when removed. Additionally, the disease above the internal auditory canal cannot be removed without sacrifice of hearing. An alternative fourth approach would be to remove the disease in the middle ear and carotid using a tympanomastoidectomy approach and removing the diseased portion above the internal auditory canal with a middle cranial fossa approach. Finally, the fifth potential approach would be to resect all disease and obliterate the areas that have had extirpated disease to prevent desiccation of the carotid artery and prevent meningocele formation.
The prognosis of the facial nerve function in cholesteatoma-induced facial paralysis is generally poor. While we have had return of function in patients with recent onset facial paralysis caused by cholesteatoma, the prospect of this patient returning to normal with nearly 2 years of paralysis is poor. In general, facial paralysis is caused by infiltration of the cholesteatoma between the bony fallopian canal and the nerve. Additionally, inflammatory changes around cholesteatoma, which occurs frequently, can lead to the development of cholesteatoma-induced facial paralysis.4,5 Early surgical intervention is associated with better outcomes of middle ear cholesteatoma complicated by facial paralysis. 5 A study by MA Siddiq et al. showed that recovery could occur even after 7-month of presentation. After this period, recovery is poor. This patient underwent a transmastoid and subarcuate approach for resection of her cholesteatoma, which led to a short-term preservation of hearing.
Conclusion
This case report of a rare giant cholesteatoma with an extra-petrous spread illustrates the need for a more thorough workup in the case of a facial spasm. The treatment of giant cholesteatomas with extensive destruction of the otic capsule and carotid artery can be performed using an approach to preserve the otic capsule, translabyrinthine, or subtotal petrosectomy with canal overclosure. The approach is dictated by the patient’s hearing and thorough review of the imaging. The approach should weigh the risk of recurrence and comorbidities and may have a chance for recovery of the facial function when performed early.
Footnotes
Declaration of Conflicting Interests
Dr. Djalilian has equity in Elinava Technologies, Cactus Medical LLC, and is a consultant to NXT Biomedical. The other author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Submission Statement
This manuscript is original and has not been submitted elsewhere in part or in whole.