
Abstract
This case study describes a 72-year-old female with a history of stapedectomy 40 years prior. She presented experiencing vertigo, fogginess, and imbalance for 9 months. Computed tomography (CT) imaging revealed that the prosthesis was displaced into the vestibule by approximately 2.1 to 2.4 mm. The patient was presented with treatment options, including observation, removal, replacement of the prosthesis, and an oval window patch. The patient opted for observation as the symptoms she was experiencing did not significantly impact her quality of life. Although a stapedectomy may fail for a multitude of reasons, some of the most common causes are prosthesis displacement, especially out of the oval window into the middle ear or away from the incus. Incus necrosis may also play a substantial role in failure.
Introduction
Stapedectomy or stapedotomy are surgical procedures that bypass the fixation of the stapes footplate. It is most often performed for patients with otosclerosis. The surgical procedure is conducted via the external auditory canal using an operative microscope or endoscope. After disarticulating the stapes from the incus, a laser, microdrill, or micropick are used to eliminate a portion of the footplate (stapedotomy) or the entire footplate (stapedectomy). 1 A stapes prosthesis is inserted between the incus and footplate to bridge the gap created by the removed stapes.
A common adverse effect after stapes surgery is dizziness or vertigo, which occurs in between 27 and 47% of primary stapes cases. 2 Symptoms typically resolve within weeks of the surgery, and it is rare to have delayed adverse effects from stapes surgery.
Case Report
The patient is a 72-year-old female who presented with a history of stapedectomy occurring 40 years prior. The patient stated she was currently experiencing vertigo, fogginess, and imbalance for 9 months. She reported that her symptoms lasted for seconds, resolved spontaneously, and were aggravated by altitude changes, loud sounds, and strenuous activity. These episodes occurred about 1 to 4 times a week. The patient reported no tinnitus, autophony, vertigo, nausea, headache, photo- or phono-phobia, scotoma, or recent changes in hearing. She had no previous history of migraine. Her symptoms did not prevent her from her activities of daily life.
The patient was referred to the primary author by an outside facility. A microscopic examination of the right ear was normal. Weber tuning fork examination lateralized to the right side, and Rinne was positive bilaterally. The audiogram (Figure 1) shows a mixed loss with an 88%-word recognition score on her right side (where she had her stapedectomy 40 years prior). The rotary chair showed a mild high-frequency phase lead with normal gain, Video Head Impulse Test (vHIT) was low gain, covert, and overt saccades noted for her right posterior canal, and the cervical Vestibular Evoked Myogenic Potential (cVEMP) and ocular Vestibular Evoked Myogenic Potential (oVEMP) were unremarkable. Video nystagmography (VNG) produced a vestibulo-ocular reflex of 0°/second in the right ear and 12°/second in the left, indicating a right unilateral weakness of 100%. Patient was referred by an outside facility for this audiogram. The right side shows a mixed loss, AD WRS is 88%, and AR WRS is 96%. The right side is where she had the stapedectomy 40 years prior.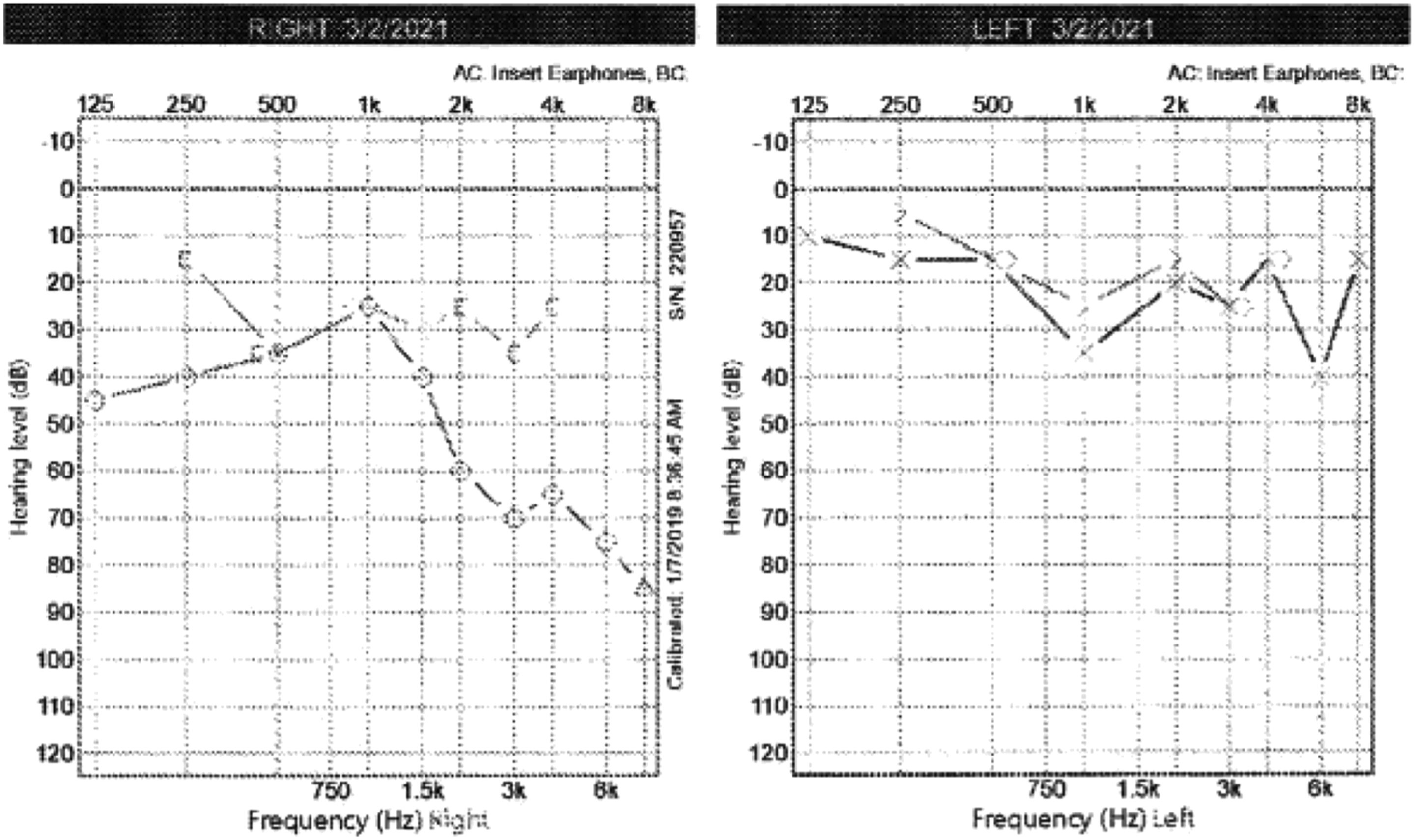
An operative report from her surgery 40 years prior was unavailable; thus, information about the prosthesis type and composition was unavailable.
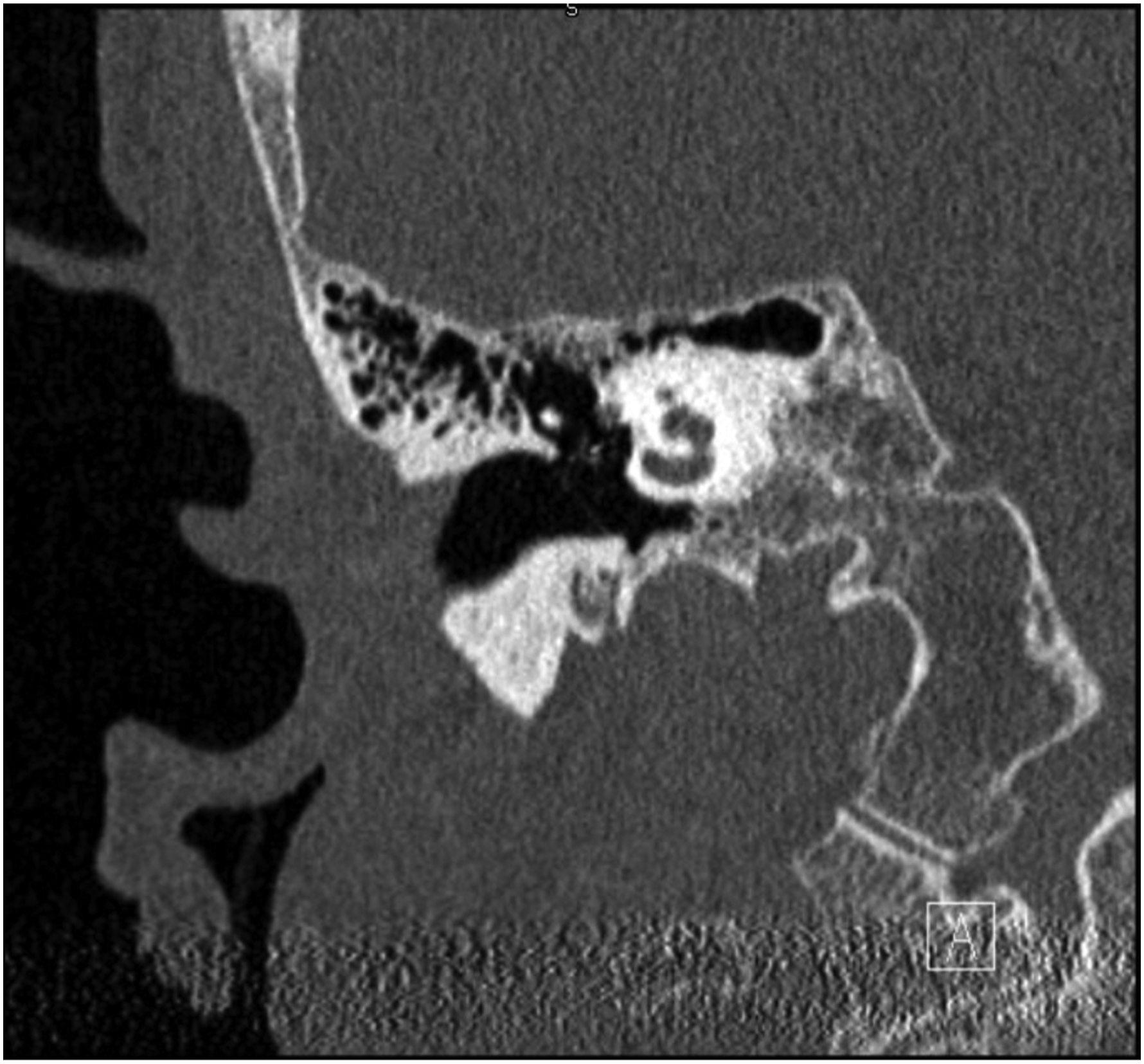
Given her history of stapedectomy, a computed tomography (CT) scan was ordered (Figure 2). The patient’s prosthesis can be seen entering her vestibule approximately 2.1 to 2.4 mm. There was no obvious dislocation of the incus or prosthesis from the incus visible on the CT (Figure 3). CT scan shows the prosthesis penetrating the patient’s vestibule between 2.1 and 2.4 mm. Coronal image of prosthesis attachment to the incus.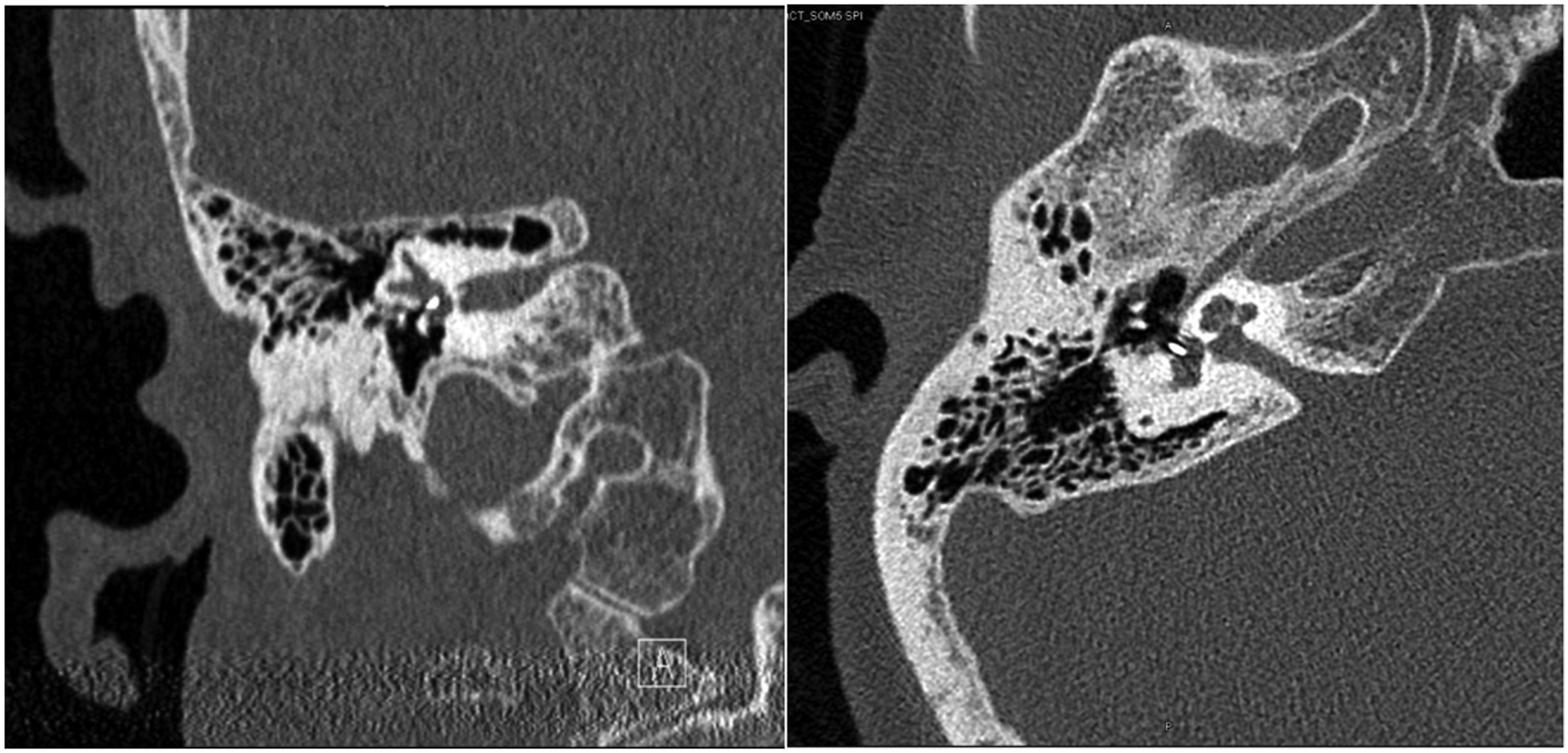
A literature review was conducted, and the patient was presented with 3 options, one of which was to observe, and the other 2 options were to remove or replace the prosthesis. The risks of each option were discussed as well. It was explained to the patient that due to the prosthesis depth of penetration, any prosthesis movement could tear the membranous labyrinth and cause complete deafness in the operated ear.
The patient opted to observe and was recommended a hearing aid to manage this hearing loss. She felt she could live with the occasional dizziness as it did not interfere with her everyday activities.
Discussion
There are only a few reports of displaced stapes prosthesis into the vestibule, and the literature does not give much direction as to how to manage these cases. A literature search on stapes surgery indicates that the most common cause of stapedectomy failure was prosthesis displacement.3-5 In most cases, the prosthesis is displaced out of the oval window and into the middle ear. However, this case illustrates a displaced prosthesis into the vestibule, which caused delayed symptoms of dizziness and imbalance that were experienced in brief episodes. Symptoms aggravated by loud sounds, altitude changes, and strenuous activity are suggestive of a third window phenomenon. With this patient’s previous history of stapes surgery, a CT scan was immediately ordered.
A similar case in a patient with delayed dizziness after stapedectomy is a 49-year-old who presented with dizziness 12 years after her stapedectomy. Her symptoms were aggravated by pressing or lying on her left side. A CT scan demonstrated her prosthesis penetrating deep into her vestibule. The authors did not discuss how they managed it. 6
Causse proposed a mechanism for the displacement of the prosthesis into the vestibule that he thought was due to Eustachian tube dysfunction. He postulated that negative pressure caused retraction of the tympanic membrane (TM). 9 As the ossicles move inward with the TM, the prosthesis would be pushed into the vestibule. Furthermore, he felt that this would possibly result in Meniere’s syndrome with resulting tinnitus, imbalance, and rotary vertigo.
Pickuth et al. discussed the role of high-resolution CT in patients with vertigo after stapes surgery. Findings in their study included the prosthesis shaft entering the vestibule and compressing the saccule, similar to what is seen in this case. Other findings found on CT in patients with vertigo after stapes surgery included complete dislocation of the stapes prosthesis, air bubbles, and fluid collections within the vestibule and outside the oval window indicating a perilymph fistula (PLF), and bony fragments leading to compression of the basal saccule. The authors concluded that patients with persistent, recurrent vertigo should be imaged with high-resolution CT, which will determine the etiology in the majority of cases. 7
In presenting the options for treatment to the patient, the depth of prosthesis penetration into the vestibule guided the discussion. An anatomic study of 10 normal and 11 osteosclerotic temporal bones concluded that no adverse effects were likely as long as instrumentation did not advance more than 1 mm deep to the footplate. Beyond that, the risks of penetrating the membranous labyrinth are significant. 8
In this case, the prosthesis penetrated beyond 2 mm, and therefore, there was a significant possibility that the prosthesis was either pushing into or adherent to the membranous labyrinth. In either case, removing the prosthesis would pose a high risk of tearing the membranous labyrinth, which would likely cause deafness. If surgery had been pursued, it would have been done under local with IV sedation anesthetic and terminated without removing the prosthesis if vertigo was experienced with manipulation of the prosthesis.
As there was no access to the patient’s original operative report, the type and material used in the prosthesis are not known. Since surgery was done 40 years ago when there were fewer prosthesis options available, some assumptions about the type of prosthesis can be made. Computed tomography features provide more information and, in this case, indicate a radio-intense piston as opposed to a wire prosthesis. The connection to the incus seems less radio-intense, indicative of a crimped prosthesis as opposed to a bucket handle. Despite the type of prosthesis, however, the depth of penetration would seem to apply the same risk of deafness to any prosthesis type.
There was no obvious inciting event in our presented case; however, she did not have a significant history of sinus or allergy-like symptoms, and a temporary Eustachian tube dysfunction could have been the cause for the displaced prosthesis. There was no history of trauma to suggest that as an etiology.
Conclusion
Higher resolution CT imaging is indicated in cases of post-operative dizziness after stapes surgery. Vertigo following stapedectomy can be due to prosthesis displacement into the vestibule, but other causes include a peri-lymphatic fistula, hydrops, and benign positional vertigo. Extreme caution should be exercised retrieving any object deeper than 1 mm below the footplate for fear of penetrating the membranous labyrinth and potentially causing deafness.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Submission Statement
This manuscript is original and has not been submitted elsewhere in part or in whole.