
Abstract
The occurrence of chyle leak after neck dissection for thyroid carcinoma is uncommon, but it usually occurs within 1–10 days after surgery. We encountered a 30-year-old patient with chyle leak 19 days after the operation for thyroid carcinoma. The initial symptom was swelling of the neck, which was quickly diagnosed as chyle leak by puncture. This report describes the patient’s presentation and discusses the conservative management of this complication. We highlight that more attention should be given to chyle leak in high-risk patients, and stricter dietary management for these patients after surgery may avoid this complication. In addition, timely diagnosis and rapid implementation of various conservative treatment measures play an important role in patient recovery.
Keywords
Introduction
Chyle leak a known complication in neck dissection, leading to injury of the thoracic duct. The incidence of chyle leak varies from 0.5% to 8.3% of patients after neck dissection for thyroid cancer.1-3 Although the rate of occurrence is low, the clinical outcomes are serious.4,5 Early and rapid diagnosis and treatment are very important for the prognosis of the disease. To date, there are rare cases of long-term complications after lateral neck dissections. 6 No literature has reported chyle leak occurring more than 10 days after surgery. There is no consensus or guide on the treatment of chyle leak after neck dissection.
We present a case of a patient who returned to the outpatient department with neck swelling 19 days following extended radical thyroid surgery. In this case, multiple conservative methods were used to try to control chyle leak, but it took a long time for the patient to recover. We reported the patient’s presentation and discuss the conservative management of this complication.
Case presentation
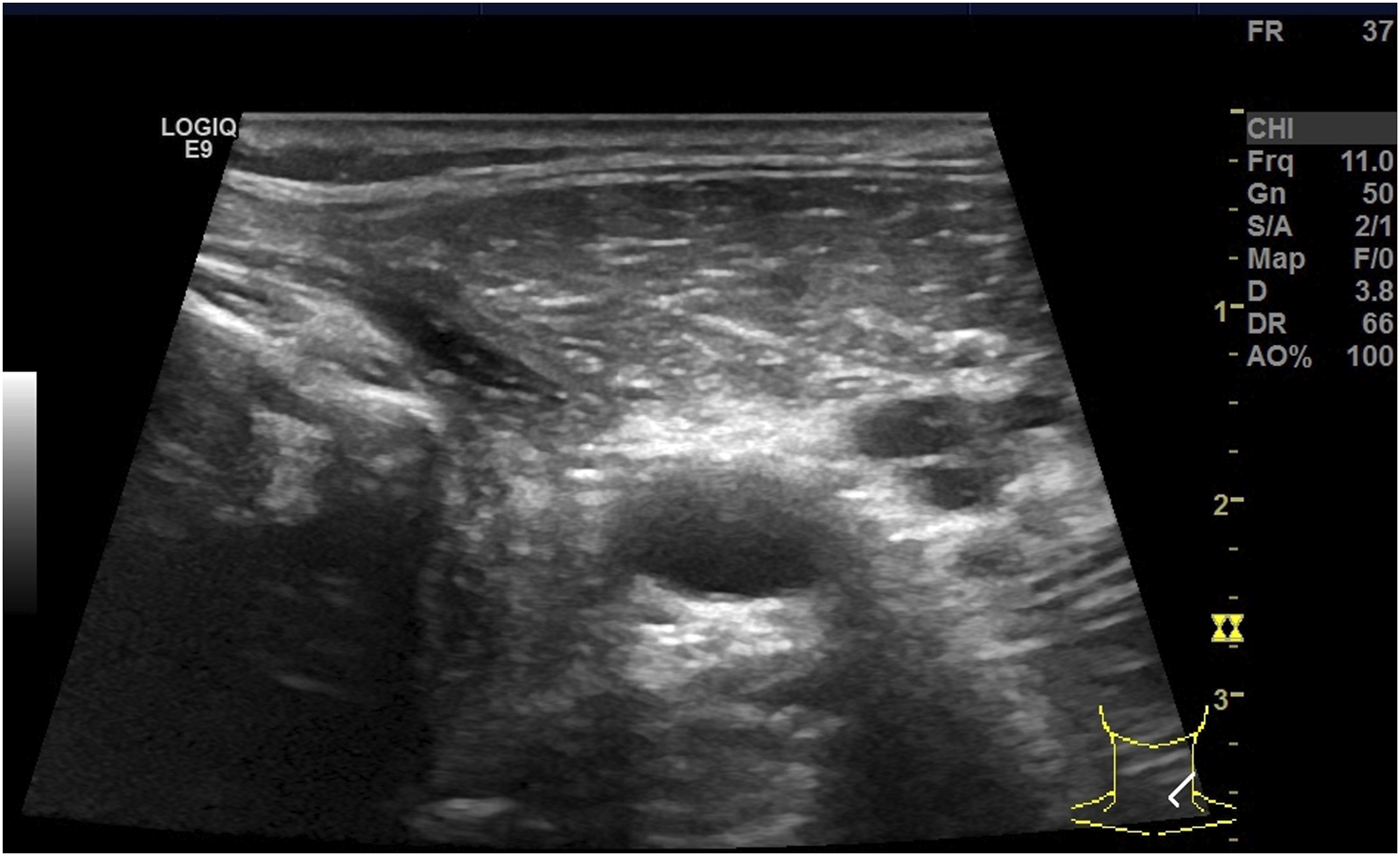
Approval for developing this case report was first obtained from the ethics committee of Zhejiang University School of Medicine Second Affiliated Hospital (Y2022-0396). A 30-year-old male was referred for a 1.2 cm solid nodule in the left thyroid lobe. The sonographic features of the nodule suggested papillary thyroid carcinoma, but fine-needle aspiration biopsy suggested an indeterminate nodule. The patient underwent an extended radical operation of the thyroid (a total thyroidectomy, isthmectomy, central compartment lymphadenectomy, and left lymph node dissection). Postoperative pathology confirmed that the nodule was papillary thyroid carcinoma with left lymph node metastasis. The patient had an uneventful postoperative recovery and was discharged 4 days later. The patient strictly adhered to a fat-free diet for 1 week after discharge and a low-fat diet for the following week, and he returned to a normal diet 2 weeks after discharge. On the 22nd postoperative day, the patient attended the outpatient department with left neck swelling that had been gradually increasing in size for three days due to a fatty diet. Physical examination revealed tense and slightly red fluctuating swelling in the thyroid bed area of the neck, and ultrasonography revealed a 7.9 × 3.8 cm cystic mass (Figure 1). Attempted needle aspiration of the swollen area produced 150 mL of milky fluid with resolution of the swelling. The patient was hospitalized twice with a series of conservative treatments, including negative pressure chyle drainage, compressive bandaging and strict dietary management, and the peak chyle output reached 1020 mL/d. After 14 days of conservative treatment in the hospital, there was no additional chyle production. The patient was then discharged with regular postoperative follow-up and seasonal ultrasound examinations. Fourteen months later, the results of the ultrasound examination were normal (Figure 2). Ultrasound examination: The left neck swelling of the patient 22 days after surgery. Ultrasound examination: The chyle leak was fully absorbed after 14 months.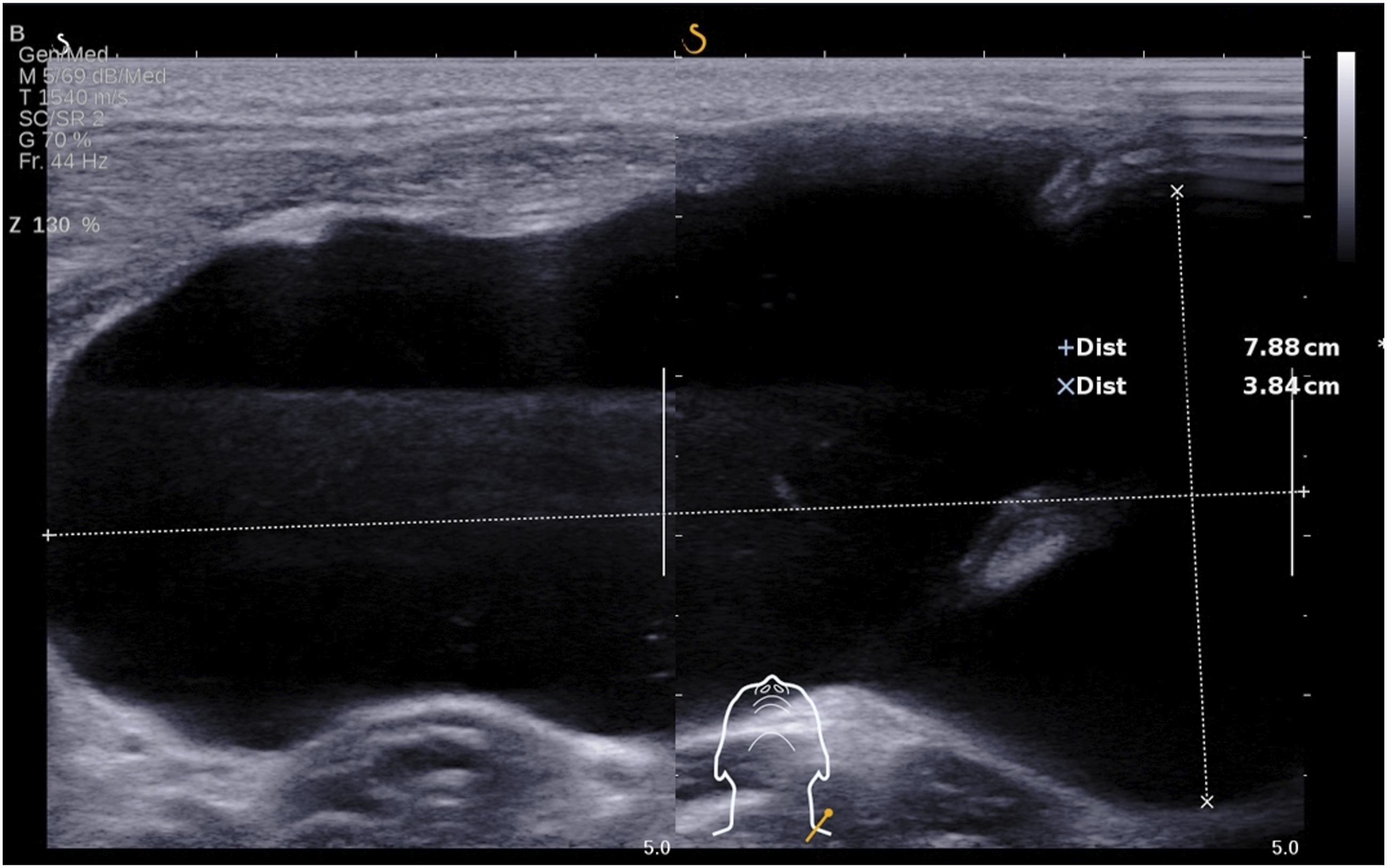
Discussion
Chyle leak is a complication of radical thyroidectomy and can be detected early by the color of the drainage liquid. The main cause is injury to the thoracic duct or right lymphatic duct in the cervical region. Some studies have found that the occurrence of chyle leak is related to the area of lymph node dissection, the number of lymph nodes dissected, and the surgical method. In other words, level IV lymph node dissection (especially on the left side), a greater number of lymph nodes dissected, and more aggressive surgical procedures are risk factors for chyle leak.6-9 Chyle leak usually occurs 1–10 days after surgery and may lead to severe metabolic disorders that affect postoperative recovery and prolong hospital stays.6,10-12
To date, there is no consensus on clear therapeutic options for chyle leak. The main treatments fall into four broad categories: intraoperative recognition of injury with repair, conservative postoperative management, using interventional radiology or minimally invasive endoscopic surgery, and re-exploration of the wound with repair. 13 In addition, chyle leak may be categorized as low output (<500–1000 mL/day) and high output based on the drainage output.12,14,15 Low output chyle leak could be treated effectively with conservative management, including bed rest, dynamic assessment of neck symptoms, dietary measures, compressive bandaging, and suction drainage.12,16 However, Delaney et al. considered that conservative management alone usually responded unsatisfactorily for high output chyle leak and that surgical intervention was necessary. 12
In this case, the patient developed a rare neck mass 19 days after surgery. After reviewing the patient’s condition, the patient underwent level IV left lymph node dissection, with a total of 27 lymph nodes removed and a large surgical range, which was closely related to the occurrence of chyle leak. Finally, the neck mass was confirmed as chyle leak by ultrasound-guided puncture. It took 14 months for this patient to recover. In this case, the patient’s peak chyle output reached 1020 mL/d, but it was treated with conservative management. Although conservative management had a good effect, the recovery time may have been shortened if we had performed timely surgical intervention.
Therefore, we should pay attention to the postoperative management of patients with high-risk factors for chyle leak. One treatment method was to extend the strict lipid intake restriction, as the patient developed symptoms soon after eating fatty food. In addition, once chyle leak occurs, the appropriate treatment should be chosen according to the amount and duration of the leakage.
Early recognition and treatment could avoid extended hospital stays. Physical examination and ultrasound could help in the early detection of a neck mass. Ultrasound-guided puncture is an appropriate method for the diagnosis of chyle leak.
Conservative treatment, such as bed rest, dynamic assessment of neck symptoms, dietary measures, compressive bandaging, and suction drainage, plays an important role in the treatment of chyle leak patients, which could alleviate symptoms and promote recovery.
Conclusion
We are the first to report a case of chyle leak occurring 19 days after thyroid cancer surgery. For patients at high risk of chyle leak, we should pay more attention to postoperative management, especially dietary management. Appropriate extension of fat-free and low-fat diets is necessary. Timely diagnosis and rapid implementation of various conservative treatment measures play an important role in patient recovery.
Footnotes
Declaration of conflicting interests
The author(s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval to report this case was obtained from the ethics committee of Zhejiang University School of Medicine Second Affiliated Hospital (Y2022-0396).
Statement of informed consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.