
Abstract
Internal maxillary artery (IMA) pseudoaneurysms are rare, and typically occur following trauma or orthognathic surgery. Pseudoaneurysms are life-threatening conditions, and expeditious workup and treatment is critical. Endoscopic treatment of an IMA pseudoaneurysm is a feasible option and should be considered when IR embolization is not available. The objective of this study is to review the literature on IMA pseudoaneurysms and present the first reported case of an IMA pseudoaneurysm successfully treated endoscopically.
Introduction
Pseudoaneurysms occur when there is a disruption in the tunica intima and tunica media of an arterial wall, while the tunica adventitia remains intact. This is in contrast to a true aneurysm, which is bounded by all three layers of the arterial wall. Pseudoaneurysms have a higher chance of rupture due to less support from the surrounding vessel wall. 1 In pseudoaneurysms, there is extravasation of blood into surrounding tissues, which can result in rapid, life-threatening hemorrhage. Internal maxillary artery (IMA) pseudoaneurysms are rare, and typically occur as a result of maxillofacial trauma or orthognathic surgery. Signs and symptoms of an IMA pseudoaneurysm include headaches, an expansile mass, pulsatile edema, recurrent epistaxis, paresthesias, and an audible bruit.1,2
Conventional arterial angiography is the gold standard to diagnose a pseudoaneurysm and it allows for endovascular treatment options such as embolization and stent-graft placement at the time of diagnosis. 3 However, this requires interventional radiology (IR) expertise and is more invasive than other diagnostic tests.4,5 A pseudoaneurysm can also be diagnosed using Computed Tomography (CT) angiography and Magnetic Resonance (MR) angiography, although the sensitivity of these tests is lower than that of conventional angiography. 3 Lastly, duplex ultrasonography can be utilized; however, this study is not as helpful for diagnosing IMA pseudoaneurysms given the bony structures that surround the IMA and location deep in the sinuses.
Depending on the size, location, and associated symptoms of a pseudoaneurysm, multiple treatment options exist. The two main treatment options for IMA pseudoaneurysms include IR embolization and open surgical repair. Here, we present a case of an IMA pseudoaneurysm that was treated exclusively by endoscopic endonasal techniques. A literature search on IMA pseudoaneurysms was performed using PubMed; to our knowledge, this represents the first reported case that was successfully treated entirely endoscopically.
Case Report
A 66-year-old female with a history of diabetes and hypertension experienced a syncopal episode following her COVID-19 vaccination that resulted in left zygomaticomaxillary complex (ZMC) and left maxillary sinus fractures. The fractures were treated non-operatively, however, three months later, she presented to the Otolaryngology clinic at a tertiary care center with progressive left facial pain, epistaxis, and left facial numbness in the distribution of the maxillary branch of the trigeminal nerve. Nasal endoscopy did not demonstrate any masses or lesions within the nasal cavity, but blood was seen in the middle meatus arising from the left maxillary sinus. Given the patient’s recurrent epistaxis and concern for a vascular lesion within the sinuses, a CT maxillofacial with contrast was obtained, which demonstrated heterogenous complete opacification of the left maxillary sinus and dehiscence of the posterior maxillary sinus wall with extension into the retromaxillary soft tissues (Figure 1a, 1b). A CT angiogram demonstrated an IMA pseudoaneurysm protruding through the dehiscent segment of the left posterior maxillary sinus wall (Figure 1c). (A) Soft tissue and (B) bone windows of axial cuts of a CT maxillofacial with contrast showing heterogenous opacification of the left maxillary sinus and dehiscence of the posterior wall with extension into the retromaxillary soft tissues. (C) Sagittal cut of a CT angiogram demonstrating an IMA pseudoaneurysm protruding through the dehiscent left posterior maxillary sinus wall.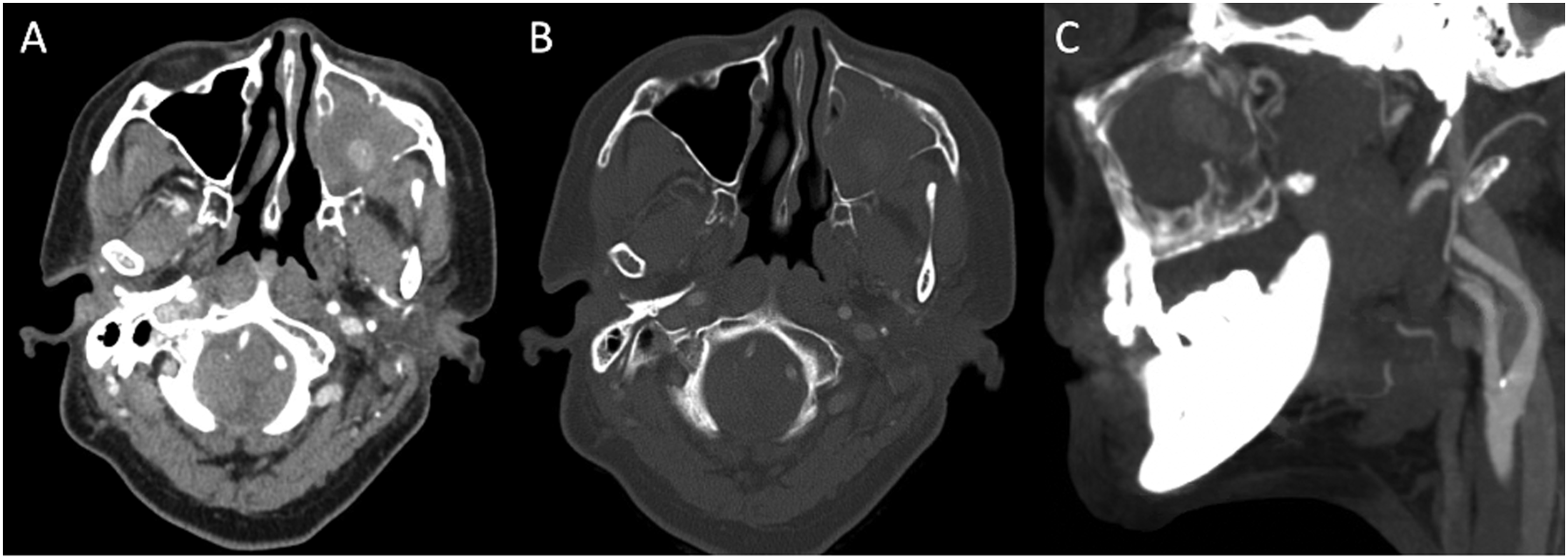
The patient was admitted from clinic due to recurrent epistaxis and severe facial pain. IR was consulted for embolization; however, timely embolization was not possible. Given the ongoing epistaxis and pain, the decision was made to proceed with urgent surgery without embolization. The patient was taken to the operating room; an endoscopic left medial maxillectomy was performed initially, however, this approach did not provide sufficient exposure to the anterior extent of the pseudoaneurysm (Figure 2a). Therefore, a left modified endoscopic Denker’s medial maxillectomy was performed to provide necessary exposure of the pseudoaneurysm (Figure 2b).
6
There was a pulsatile mass filling the left maxillary sinus that bled with any manipulation. A portion of the mass was excised and sent to pathology, which demonstrated blood and fibrin, with no evidence of neoplasia. The mass was then quickly debulked to the posterior maxillary wall using a microdebrider. The posterior maxillary wall defect was then enlarged laterally to expose the proximal IMA, and bipolar electrocautery was used to achieve both proximal and distal control of the IMA. The remainder of the mass was removed from the pterygopalatine fossa to the infratemporal fossa using bipolar cautery. The resulting defect was then reconstructed using a graft of DuraMatrix (Stryker, Kalamazoo, MI), which was secured using Tisseel and Gelfoam. The graft was used to aid in healing by covering the exposed contents of the pterygopalatine fossa and to reduce the risk of bleeding during postoperative debridement and packing removal. The maxillary sinus and nasal cavity were then packed with absorbable nasal packing (Hemapore, Stryker, Kalamazoo, MI). (A) Pseudoaneurysm completely filling the left maxillary sinus following medial maxillectomy. (B) anteromedial maxillectomy via endoscopic Denker’s approach, providing visualization of the anterior portion of the pseudoaneurysm. Legend: NS=nasal septum; NF=nasal floor; MM=medial maxillary sinus wall; AM=anterior maxillary sinus wall; *=pseudoaneurysm.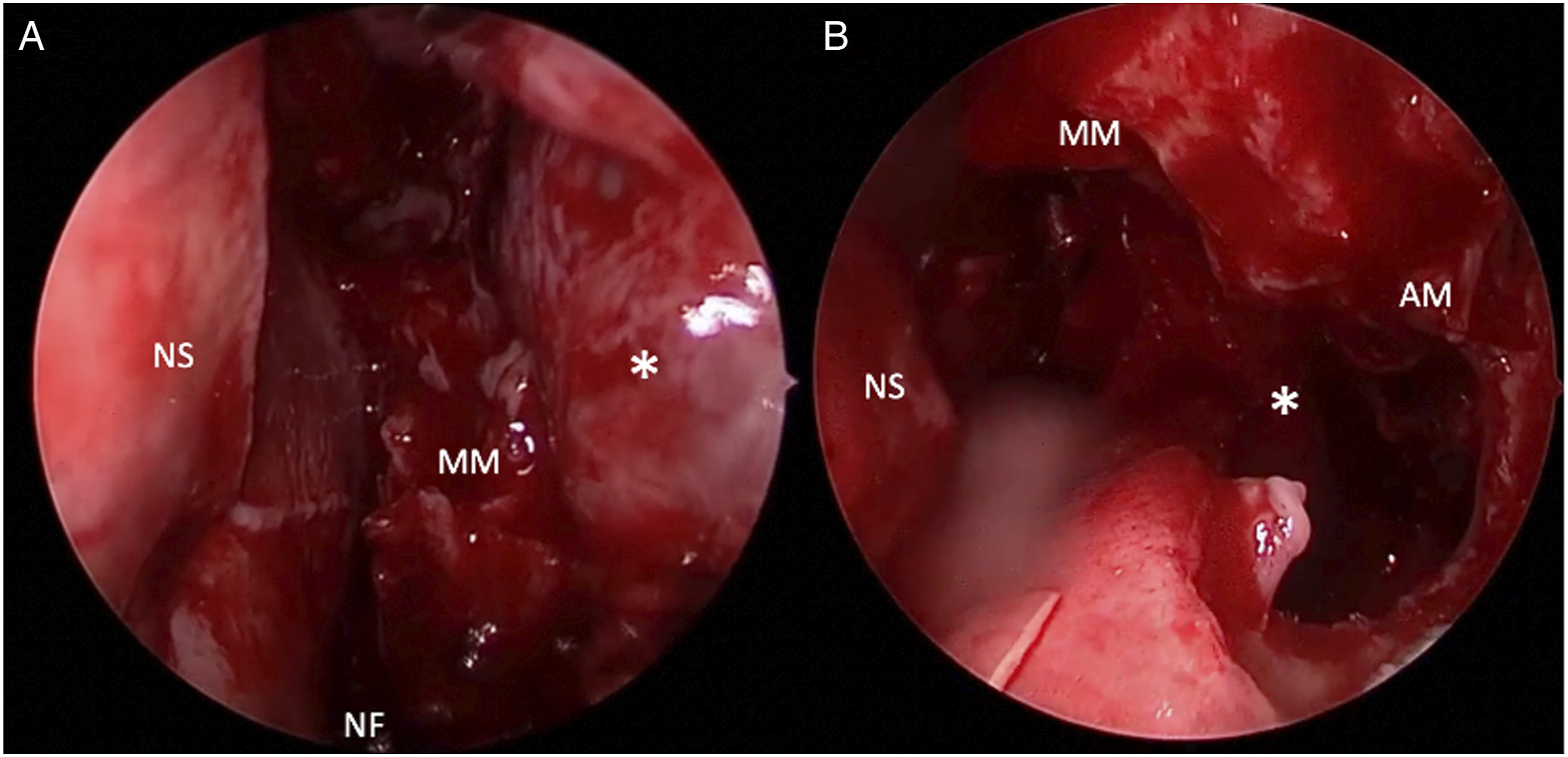
Postoperatively, the patient had quick resolution of her facial pain and epistaxis. She was seen in clinic eight weeks after surgery. Nasal endoscopy demonstrated a well-healed left maxillary sinus, and there was no evidence of recurrent pseudoaneurysm.
Discussion
A review of the literature in PubMed revealed 81 case reports of IMA pseudoaneurysms. The etiology of the pseudoaneurysms were as follows: trauma (71.6%, n = 58), orthognathic surgery (12.3%, n = 10), external beam radiation (8.6%, n = 7), infection (2.5%, n = 2), endoscopic sinus surgery (2.5%, n = 2), and CT-guided biopsy (2.5%, n = 2). These 81 cases were treated with embolization (84%, n = 68), open surgery (13.6%, n = 11), embolization and open surgery (1.2%, n = 1), and observation (1.2%, n = 1). There were no reported cases of IMA pseudoaneurysms being managed with endoscopic techniques.
The advantages of the endoscopic technique for ligation of an IMA pseudoaneurysm compared to an open approach such as a Caldwell Luc include superior visualization, lower morbidity without the sublabial incision, and improved surveillance capabilities provided by the endoscopic approach. In this case, the use of a modified endoscopic Denker’s medial maxillectomy was critical in providing adequate access to the anterior aspect of the pseudoaneurysm. This technique was described by Lee et al. in 2017 and utilizes an endoscopic endonasal anterior maxillotomy with removal of the lateral nasal wall and nasolacrimal duct. 6 This approach obviates the need for a separate sublabial incision to access the anteroinferior and anterolateral aspects of the maxillary sinus, which are otherwise difficult to reach with a standard medial maxillectomy. Additionally, embolization was not available prior to this case, and this report demonstrates that endoscopic surgery can be performed safely if IR is not available. An endoscopic approach can also be utilized if there is a need to clear the maxillary sinus and remove the pseudoaneurysm after embolization is performed by IR.
A pseudoaneurysm can be a life-threatening condition, given the potential rupture resulting in rapid hemorrhage. A pseudoaneurysm should be on the differential diagnosis for an unexplained expansile mass, even if characteristic features such as pulsations and audible bruit are not present. The presentation of a pseudoaneurysm is often delayed from the inciting event, and accurate diagnosis requires a high index of suspicion, as contrast-enhanced scans are not routinely performed for sinus symptoms. In this location, a standard maxillary antrostomy would not provide adequate visualization of the mass for removal and hemostasis. While the literature demonstrates that embolization has become the mainstay treatment for IMA pseudoaneurysms, the proximity of the IMA to the posterior wall of the maxillary sinus makes it accessible for endoscopic management. This report documents the successful treatment of an IMA pseudoaneurysm using an entirely endoscopic approach.
Conclusion
IMA pseudoaneurysms are uncommon and most frequently occur following trauma or orthognathic surgery. This is a potentially life-threatening condition and expeditious workup and treatment is critical. Endoscopic treatment of an IMA pseudoaneurysm is a feasible option and should be considered when IR embolization is not available.
Surgical Link
https://www.dropbox.com/s/tg1163yp7y53s59/pseudoaneurysm1.mp4?dl=0
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.