
Abstract
Objectives
Our objective was to study the efficacy and safety of intratymapanic dexamethasone (ITD) for treating in Méniere’s disease in southern China.
Methods
A total of 124 patients with Méniere’s disease were randomly divided into 2 groups: ITD group (n = 62) and intratympanic lidocaine (ITL) group (n = 62). The ITD group was further randomly divided into 2 groups based on dexamethasone dosage: ITD1 (2 mg/ml) (n = 31) and ITD2 (5 mg/ml) group (n = 31). Symptom alleviation and complications were recorded after every treatment.
Results
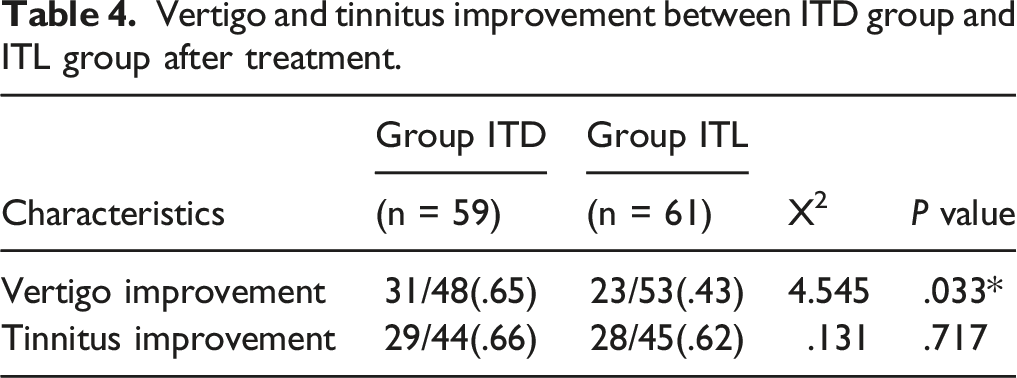
Vertigo was improved in 65% of patients who received ITD compared with 55% of patients who received ITL patients (P < .05). Three patients in the ITD2 group had from otomycosis, and 2 of these patients had a perforation; no tympanic membrane perforation was observed in the ITL and ITD1 group.
Conclusions
Compared with lidocaine, dexamethasone is more effective in alleviating vertigo, and a lower concentration of dexamethasone can reduce the occurrence of complications.
Keywords
Introduction
Intratympanic dexamethasone (ITD) is used to treat a number of inner ear diseases, such as Méniere’s disease, sensorineural hearing loss (SNHL), autoimmune inner ear disease, and idiopathic sudden deafness.1-3 Previous studies have shown that ITD does not cause long-term complications that can affect a patients’ quality of life; minor complications include local pain, bleeding, and temporary dizziness during injection. While ITD is effective for treating inner ear diseases, we have observed that some patients develop otomycosis after ITD, which may be related to the concentration of dexamethasone. In severe cases, we have also observed persistent perforation of the tympanic membrane. As such, ITD can be associated with long-term side effects, and every specialist should master the management of these complications.
The effectiveness of ITD for treating tinnitus associated with Méniere’s disease is 57%. 1 Intratympanic lidocaine (ITL) is also used to treat tinnitus caused by Méniere’s disease, with a reported effective rate of over 67.8%. 4 ITL is also widely used to treat Méniere’s disease at our center.
The purpose of this study was to compare the effectiveness and safety of ITD and ITL for treating Méniere’s disease.
Material and Methods
Patient Selection
This study was carried out at the Department of Otolaryngology–Head and Neck Surgery of the Third Affiliated Hospital of Sun Yat-sen University from January 2016 to June 2019. Patients with Meniere’s disease who received either ITD or ITL to treat tinnitus associated with Méniere’s disease were enrolled in the study. Patients were divided into an ITD group and ITL group using the random table method. A total of 124 patients were enrolled: 62 in the ITD group and 62 in the ITL group. All patients were diagnosed with Méniere’s disease according to Bárány Society criteria: 5
(1). Two or more spontaneous episodes of vertigo, each lasting 20 minutes to 12 hours. (2) Audiometrically documented low- to medium-frequency sensorineural hearing loss in one ear, defining the affected ear on at least one occasion before, during, or after an episode of vertigo. (3) Fluctuating aural symptoms (hearing, tinnitus, or fullness) in the affected ear. (4) Symptoms not better accounted for by another vestibular diagnosis.
Exclusion criteria were: (1) External ear, middle ear, and other local inner ear diseases; (2) Systemic disease such as diabetes and hypertension; and (3) Malignancy. Patients who could not complete the follow-up were also excluded. This study was approved by the Ethics Committee of the Third Affiliated Hospital of Sun Yat-sen University. All patients provided written informed consent for participation in the study.
Study Design
ITD Group
The ITD group included 62 patients who were diagnosed with Méniere’s disease (83 ears). Méniere’s disease was strictly diagnosed according to symptoms including episodic vertigo, aural fullness, tinnitus, and hearing loss, based on the criteria previously described. All patients had complete audiologic and caloric examinations. Patients in ITD group were further randomly divided into the ITD1 group (2 mg dexamethasone/ml, n = 31) and ITD2 group (5 mg dexamethasone/ml, n = 31). Dexamethasone was injected into the eardrum under endoscopic guidance, with the patient lying on the side with the affected ear facing upwards. Dexamethasone was added to the middle ear cavity, and the round window membrane was immersed in the solution for an appropriate time. The patient lied with the ear up for 20 minutes so that the round window membrane would be bathed in the solution for a proper time. Patients received ITD every 3 days for a total 10 treatments. Treatment was initiated during hospitalization, and if 10 treatments were not completed by discharged, the remaining treatments were performed in the outpatient department.
ITL Group
A total of 62 patients (91 ears) who met the aforementioned criteria for diagnosis of Méniere’s disease were treated with ITL. The concentration of lidocaine 20 mg/ml, and the method and frequency of injection were the same as the ITD group.
During treatment, all patients in both groups received betahistine 12 mg tid and mecobalamin .5 mg tid orally to improve inner ear microcirculation and neural function.
Follow-up
Before treatment, every patient was given health education indicating the importance of each follow-up visit. Patients received a total of 10 intratympanic injections, 1 every 3 days, and the total follow-up period was 1 month. All injections were given by the same doctor, and injection complications were recorded in detail.
Patients with tinnitus or dizziness were scored using the Tinnitus Handicap Inventory (THI; Newman et al 1996) 6 or the Dizziness Handicap Inventory (DHI; Jacobson et al 1990), 7 respectively, before each treatment and the last follow-up. A lower score after treatment is considered an improvement of symptoms. If secretions were present in the external canal they were sent for fungal smear and fungal culture. CHROMagar Candida medium was used to identify Candida species. The diagnostic criteria for otomycosis included: (a) subjective symptoms of one or more of the following: ear itching, ear pain, sensation of foreign matter in the ear, fluid flow in the ear, and hearing loss; (b) otoendoscopy examination showing the skin of the external auditory meatus exhibited flaky, punctate, or blotchy gray or brown fungal hyphae; fungal spores or other lesions; and the skin of the external auditory meatus was congested with yellow, purulent secretions; and (c) positive fungal smear of ear canal secretions.
Patients diagnosed with otomycosis were treated by cleaning the fungal secretions from the external auditory meatus and filling it with antifungal triamcinolone acetonide clotrimazole cream (Parrishon; Yeung Sum Pharmaceutical Co, Xi’an, China). A number of studies have reported the effectiveness of triamcinolone acetonide clotrimazole cream for treating fungal infections of the external auditory meatus.8,9 After treatment patients were considered cured if they were symptom-free and no abnormal secretions were observed in the external auditory canal by otoendoscopy. Otherwise, the treatment was deemed unsuccessful.
Statistical Analysis
Measurement data were presented as mean ± standard deviation, and Student’s t-test or analysis of variance was used for comparisons between groups. Categorical data were compared with the chi-square test. A value of P < .05 was considered to indicate statistical significance. Statistical analysis was performed with SPSS version 22.0 software.
Results
Data Collection
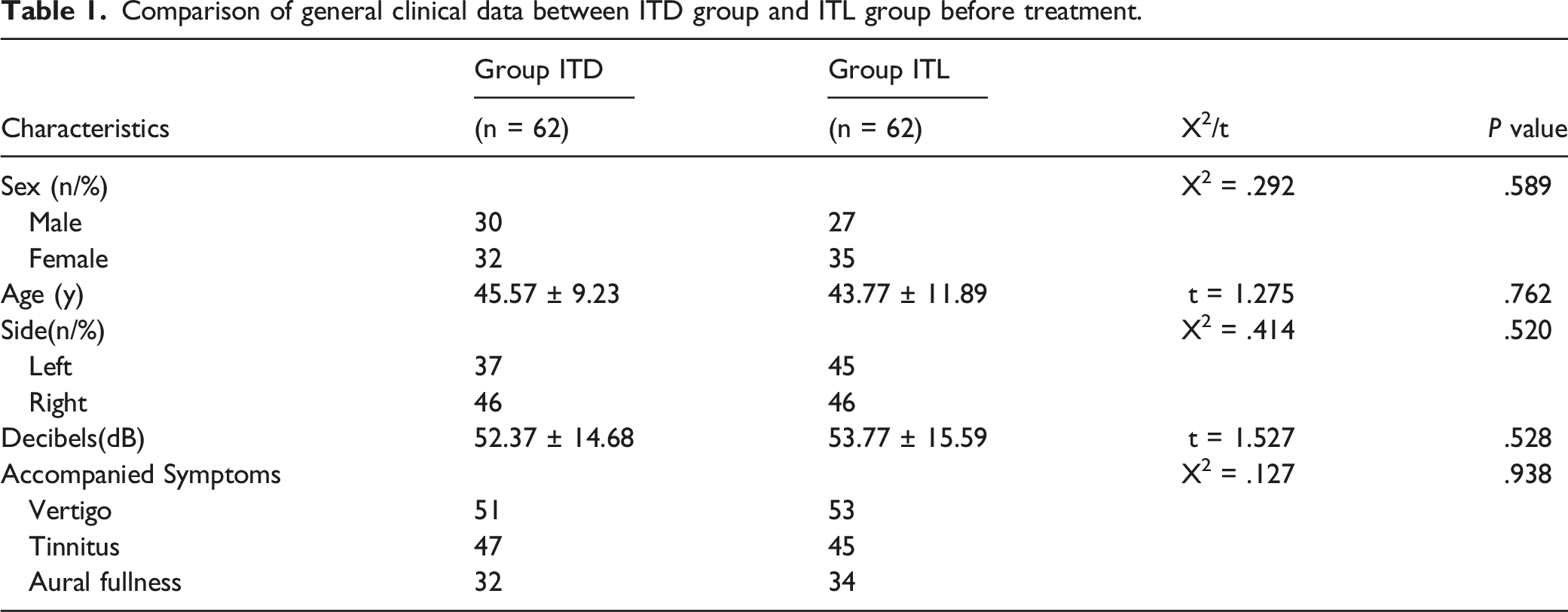
Comparison of general clinical data between ITD group and ITL group before treatment.
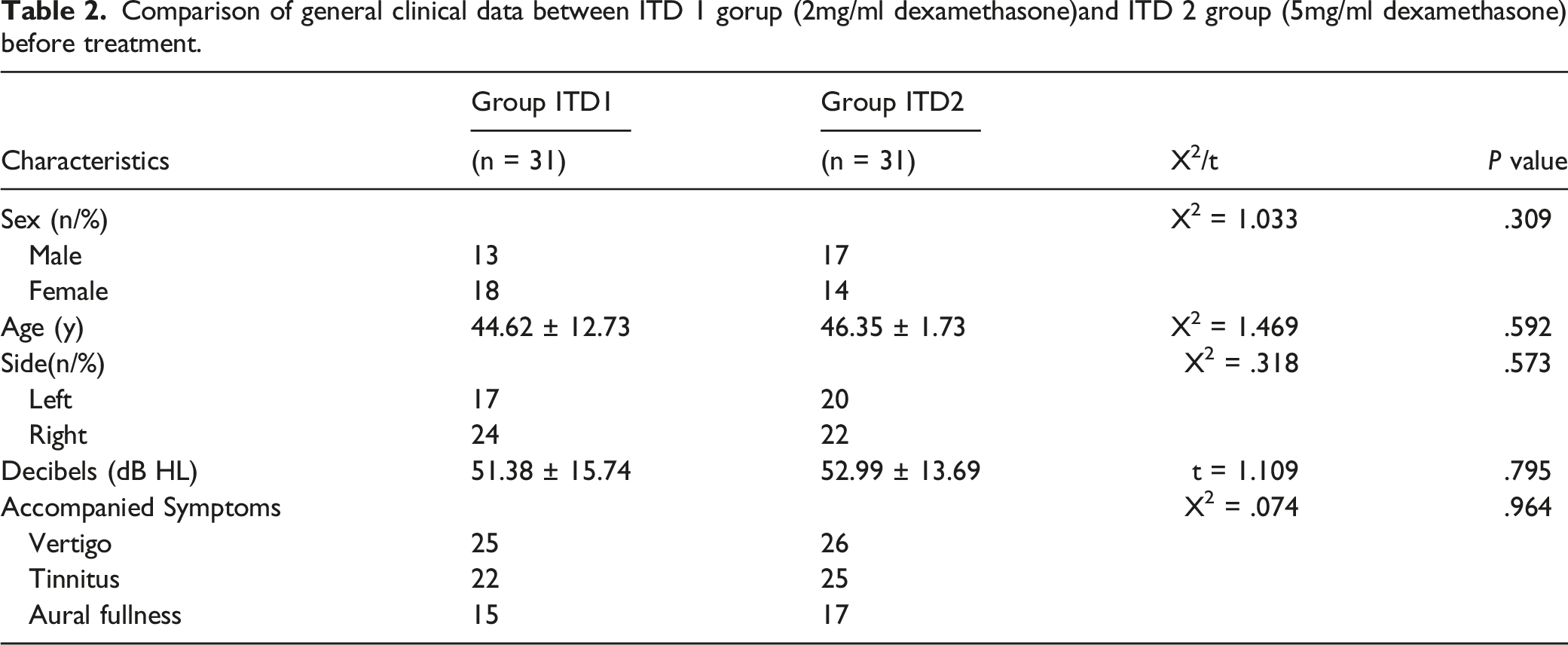
Comparison of general clinical data between ITD 1 gorup (2mg/ml dexamethasone)and ITD 2 group (5mg/ml dexamethasone) before treatment.
Complications in ITD and ITL groups
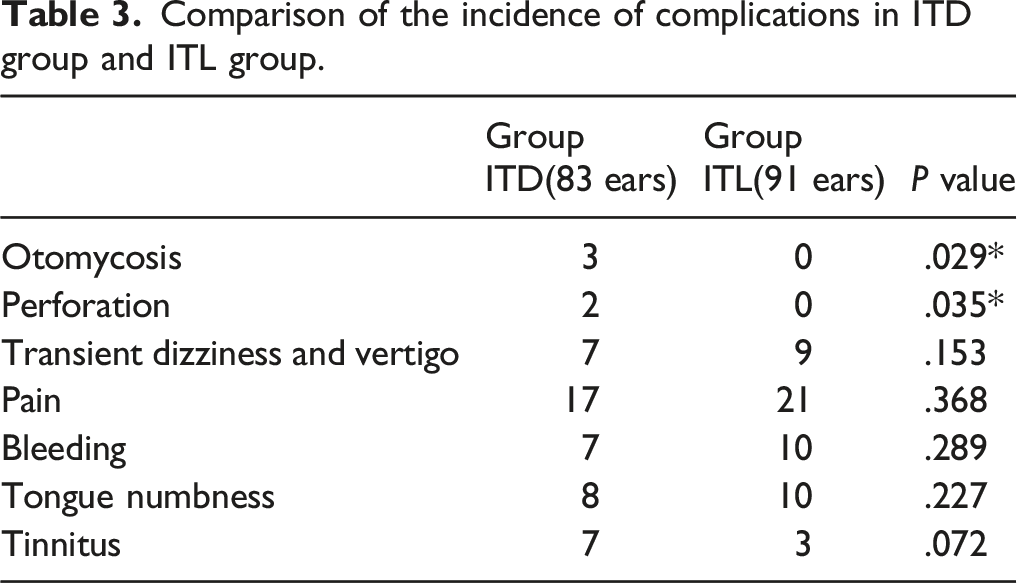
Comparison of the incidence of complications in ITD group and ITL group.
Otomycosis
Three patients in the ITD2 group developed otomycosis after treatment. One patient developed otomycosis 12 days after the beginning of treatment and was observed as a thick black fungus silk on the left tympanic membrane. Fungal culture was positive for Aspergillus niger. The patient was treated with triamcinolone acetonide and econazole cream injected into the external auditory canal for 4 weeks. The treatment was effective at eliminating the fungal infection, and ITD treatments were resumed (Figure 1A). Images of otomycosis after ITD.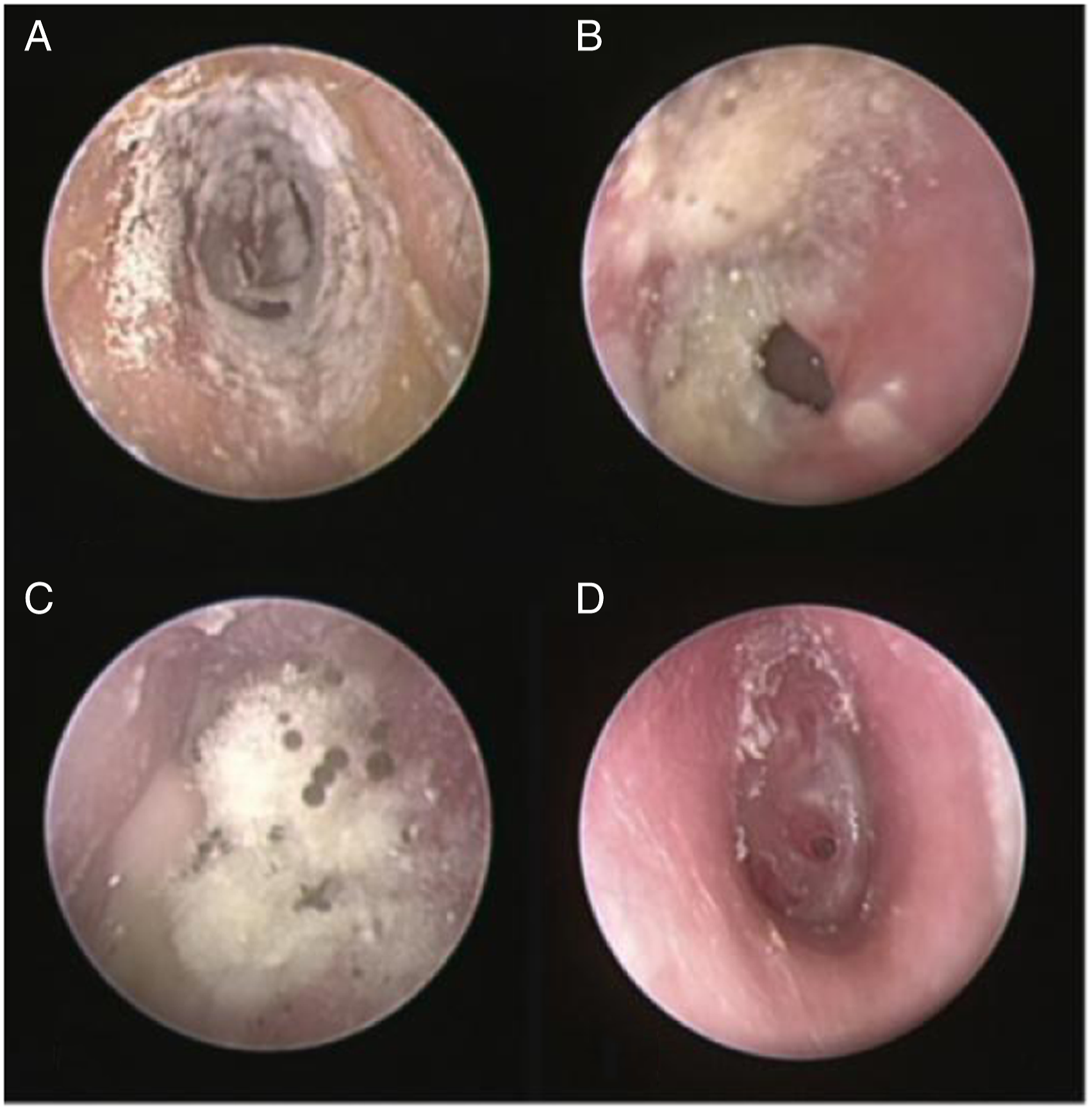
The second patient developed a fungal infection in the external canal after 21 days after beginning treatment. Initially, a large amount of white, brown, and yellow fungi were noted in the right external canal. Fungal culture was positive for Aspergillus flavus. The patient developed right otitis 7 days later. He was treated with antibiotics, and applied triamcinolone acetonide and econazole cream injected into the external canal. The infection was controlled after 14 days later, but he experienced a perforation of the eardrum after 3 months. Treatment with triamcinolone acetonide and econazole cream was continued weekly for 4 weeks; the fungal infection resolved but a persistent perforation remained (Figure 1B).
The third patient developed otomycosis 18 days after beginning treatment. She had received the first 2 injections over 7 days she was an inpatient. A 18 days she complained of itching, loss of hearing in the right ear, and some green secretions from the ear. Endotoscope examination showed mycoses were so thick that they covered all the membrane, as well as white, brown, and black secretions. After clearing the ear canal, a needle-like perforation in the anterior-inferior quadrant of tympanic membrane was noted, and membrane atrophy/thinning was seen around the perforation. Fungal culture was positive for Aspergillus niger. She was treated with triamcinolone acetonide and econazole cream in the external canal weekly for 4 weeks. After treatment, the fungal infection was resolved and the perforation was healed (Figures 1C and 1D).
Curative Effect Analysis
Vertigo and tinnitus improvement between ITD group and ITL group after treatment.
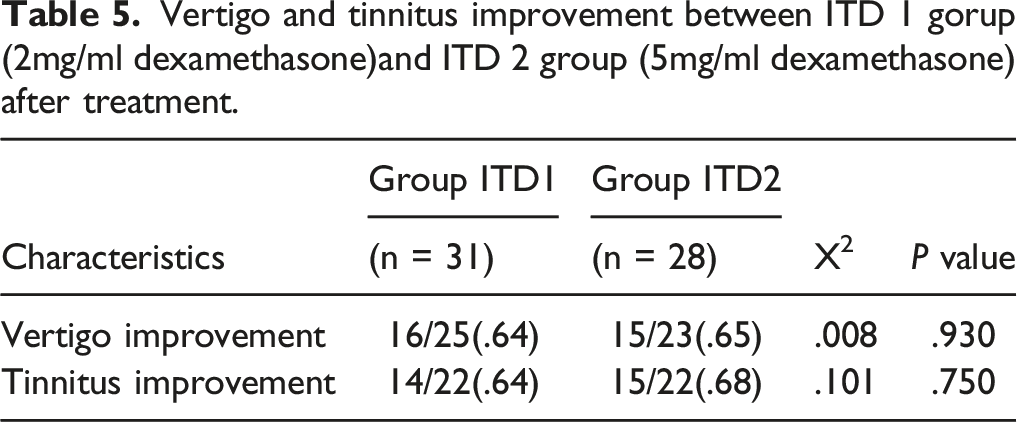
Vertigo and tinnitus improvement between ITD 1 gorup (2mg/ml dexamethasone)and ITD 2 group (5mg/ml dexamethasone) after treatment.
DHI and THI subscale for ITD and ITL group.
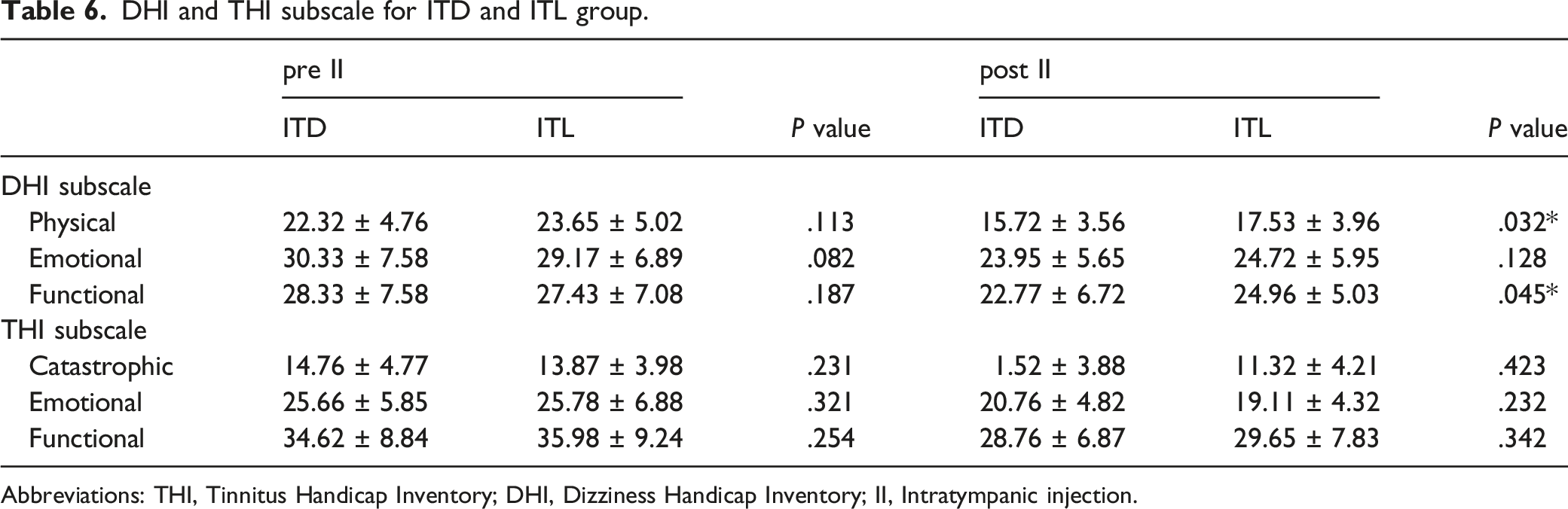
Abbreviations: THI, Tinnitus Handicap Inventory; DHI, Dizziness Handicap Inventory; II, Intratympanic injection.
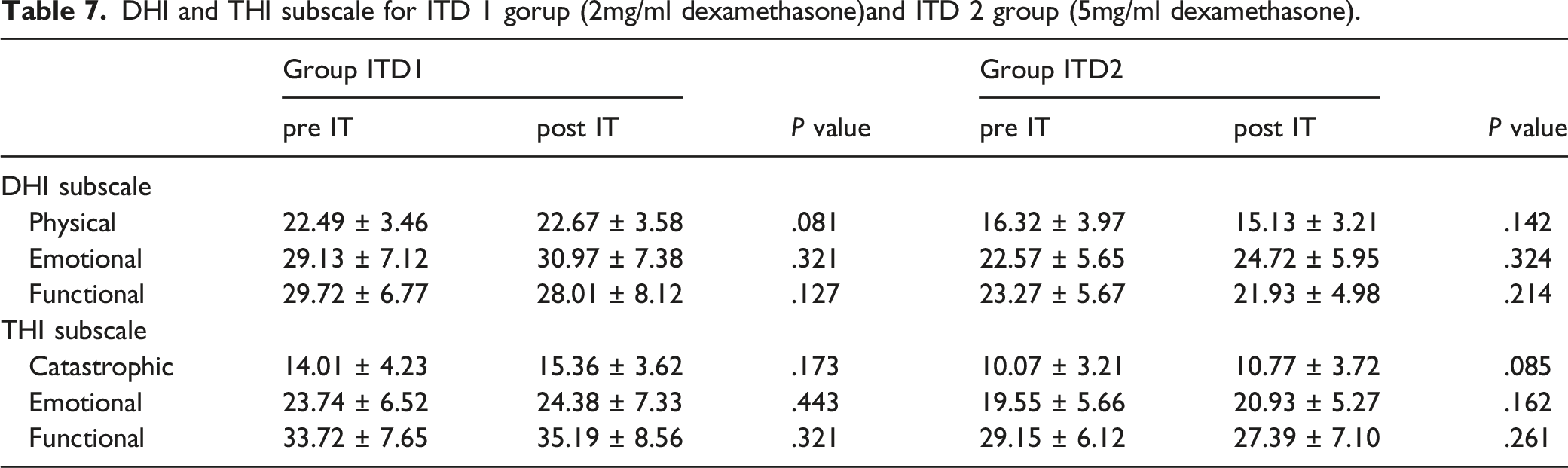
DHI and THI subscale for ITD 1 gorup (2mg/ml dexamethasone)and ITD 2 group (5mg/ml dexamethasone).
Discussion
The intratympanic injection technique was first reported by Schuknecht in 1956 when he used intratympanic streptomycin to treat Ménière’s disease. 10 In 1985, Fradis used IT lidocaine to treat Méniere’s disease, and 67.8% of patients had an improvement of tinnitus. 4 In 1987, Sakata used IT dexamethasone to treat the Méniere’s disease in 61 patients, and 74% had an improvement of tinnitus. Currently, ITD and ITL are commonly used to treat Méniere’s disease. 11 Neither of the 2 reports from the 1980s mention complications of IT, and both concluded that ITD or ITL were safe and effective. However, current research has suggested that there may be some adverse effects with this method.
Complications
Intratympanic steroid injection has become a regular treatment for Méniere’s disease, sudden hearing loss, autoimmune inner ear diseases, and SNHL. In our study, we observed some minor complications of intratympanic injections such as transient dizziness and vertigo, pain, tongue numbness, and tinnitus. Other researchers have also reported side effects of the intratympanic steroid injections. Guan-min et al 12 studied 39 patients who received intratympanic steroid injections, and reported one patient developed acne and another patient developed vertigo immediately after the injection, and recovered after 2 hours of rest. Plontke et al 13 followed 23 patients who received intratympanic steroid injections for 2 weeks, and found 2 patients developed otalgia, 1 patient a headache, 1 patient an ear canal skin defect, and 1 patient developed vertigo. Park et al 14 followed 88 patients who received intratympanic steroid injections for 3 months, and found 25 patients (28.4%) had complications including otalgia (11/88), transient dizziness (9/88), ear fullness (8/88), and headache (5/88). Wu et al 15 followed 55 patients who received intratympanic steroid injections for a month and found that 18 patients had transient dizziness and 1 patient had a temporary tympanic membrane perforation. In our study, despite nearly one-fifth of the overall study population developing complications, the majority of them were technique-related, very transient, and self-resolving. They included transient dizziness/vertigo post-injection, and ear fullness and slight otalgia during injection, which can be all caused by the injection technique. Given that patients recovered after only a few minutes, we believe the transient vertigo attacks are due to the introduction of warm or cold liquids into the external ear canal.
Otomycosis
In our study, some patients developed external auditory meatus mycosis. In our literature search, we did not find any reports of mycosis of the external auditory canal after intratympanic injections. While we did not find any report of mycosis of the external auditory canal, we noted that some patients developed mycosis after ITD. The possible reason is that our vertigo center admits a large number of patients from southern China, including more than 250 Méniere’s disease patients every year. Due to the large number of patients, it is not unusual that some rare complications are observed. We speculate that otomycosis after intratympanic injection may be related to the following 3 factors.
Dexamethasone
In our study, only patients that received ITD developed mycosis of the external auditory canal. As such, dexamethasone injection into the tympanic cavity may increase the risk for immunosuppression and opportunistic infection. Leav et al 16 reported a case of invasive pulmonary aspergillosis in a patient with asthma who was treated with high-dose inhaled fluticasone (1,760 mg daily), which is significantly higher than the standard dosage (440 mg twice daily). This suggests that steroids can lead to immunosuppression, and the higher the concentration, the greater the chance of an opportunistic infection. This is consistent with what we observed in our study. All the patients who developed a fungal infection were treated with 5 mg/ml of dexamethasone; no patients treated with 2 mg/ml developed a fungal infection. This suggests that the lowest effective concentration of dexamethasone should be used. We also noted that the rate of tinnitus improvement was similar between the ITD1 and ITD2 groups. Therefore, our results indicate that 2 mg/ml dexamethasone reduces the chance of otomycosis without reducing treatment effectiveness. Nonetheless, previous studies using higher concentrations of dexamethasone ranging from 10 mg/ml to 24 mg/ml for the treatment of Ménière’s disease have not reported an increase of external auditory meatus mycosis.17-19 A possible reason is that most patients in the studies received injections only 1–5 times per month; not as frequent as in our study.
Climate: Warm and Humid
The warm and humid environment in southern China favors the development of fungal infection of the external auditory meatus. Fungi can easily reproduce in a warm environment. Our hospital is located in a subtropical region, with an average temperature of over 22.5°C, and the appropriate growth temperature of fungi is between 20-35°C. Second, Guangzhou is close to the ocean and there are barriers (e.g., big mountains) to prevent the warm and humid air flow coming from the ocean from reaching Guangzhou. This warm and humid environment is very favorable for the growth of fungi. 20 It is because of this geography that fungal external auditory meatus infection is not common in northern China, and doctors in areas where the infection is not common may lack understanding of the disease, resulting in some missed diagnosis of otomycosis.
The clinical characteristics of otomycosis include obvious ear itching accompanied by a sense of ear blockage. Endotoscopy may show a thick white fungal silk on the tympanic membrane, or a white, brown, yellow, or black mycosis mass blocking the external auditory canal. Microscopic examination of the mass will reveal fungal spores. 21
Iatrogenic Infections
The third factor may be iatrogenic infections, which may be because the whole treatment process is not standardized, nor is the use of antifungal drugs. If the syringe is not properly sterilized during drug extraction, a small number of fungal spores may be iatrogenic into the eardrum or external auditory canal, which may cause local propagation and spread of the fungus. Thus, more attention needs to be given to standardizing procedures to reduce the possibility of iatrogenic infection. Treatment with fungus-contaminated steroids is one of the most common causes of fungal infection. Kauffman et al 22 reported that in 2012, 751 patients developed fungal meningitis, stroke, spinal or paraspinal infection, or peripheral osteoarticular infection and 64 died. In the end, they found that most patients had undergone epidural injection or osteoarticular injections with fungus-contaminated methylprednisolone acetate, resulting in a significant number of intracranial and intra-articular infections. Fungal infections can also be caused by contaminated drugs injected into the ear, so aseptic procedures should be followed and the government must carry out the most stringent quality control requirements for the production of drugs.
Curative Effect Analysis
Our results showed that with the same number of injections there was no significant difference in rate of tinnitus improvement between the ITD group and the ITL group, but there was a significant advantage in the improvement of vertigo in the ITD group. There was no significant difference in the rate of tinnitus or vertigo improvement between ITD1 and ITD2 groups. Patients in the ITD2 group were more likely to have complications such as otomycosis and tympanic membrane perforation. These findings suggested that dexamethasone has a better therapeutic effect than lidocaine, and a lower concentration of dexamethasone can reduce the occurrence of complications. Therefore, we recommend that a concentration of 2 mg dexamethasone/ml be used.
Conclusions
In this study, we found that otomycosis, though rare, is a complication of ITD, and this has not been previously reported. Notably, a concentration of 2 mg dexamethasone/ml can reduce the occurrence of fungal external auditory meatus infection while also improving tinnitus. Mycosis of the external auditory canal can be cured by active treatment. ITD is still the recommended treatment for Ménière’s disease, but the concentration should be reduced to 2 mg/ml. Because the number of patients in this study was relatively low, study with a larger number is needed to support our conclusions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Science and Technology Program of Guangzhou, China (Grant No. 201704030081).
Ethical Standards
All procedures/treatment in this study and the treatment of patients comply with the ethical standards of the relevant national and institutional committees on human experimentation, and with the Helsinki Declaration of 1975, as revised in 2008.