
Abstract
Objectives
To examine the difference in survival of obstructive sleep apnea (OSA) based on marital status and race.
Methods
A single academic institution with data collection from 2005 to 2015. Patients with a diagnosis of OSA based on polysomnogram were abstracted from electronic medical records. Patients were classified as “married” or “unmarried.” Race was self-reported as White, Black, Asian American, Hispanic/Latinx, Middle Eastern descent, or unrecorded and gathered from the electronic medical record.
Results
There were 6200 adults included. Of these, married patients composed 62.7% (n = 3890) of the patients. Patients were 51.3% White (n = 3182), 39.8% (n = 2467) were Black, and 8.9% (n = 551) were other/unrecorded. Married patients had better survival probabilities (p < .0001). Unmarried patients had 2.72 times the risk of death than those who were married (95% CI 1.78–4.20) when examining OSA survival. When examining survival of those on continuous positive airway pressure (CPAP) between married and unmarried patients, those who were unmarried had 2.00 (95% CI 1.58–2.54) times the risk of death than those who were married. Married Black patients demonstrated the best survival probabilities, followed by married White patients (p < .0001). Married patients had lower mean sleep efficiency than those that were unmarried (76.2% and 77.2%, respectively; p = .019).
Conclusion
Married patients with OSA had increased survival compared to their single counterparts. Married Black patients had the highest survival.
Introduction
Obstructive sleep apnea (OSA) occurs when there is inadequate tone or excess tissue of the upper airway resulting in collapse during sleep. It is defined as a disorder in which a patient repeatedly stops breathing during sleep due to upper airway obstruction. 1 -6 Treatment depends on severity, though most commonly consists of lifestyle modification, weight loss, continuous positive airway pressure (CPAP), oral appliances, or surgery. 7 CPAP is considered the gold standard; however, adherence to CPAP remains a challenge for many patients due to skin irritation, nasal congestion/dryness, and stomach bloating. 8 -10
It is known that OSA can impact intimate relationships, namely, that OSA negatively impacts partners’ sleep, mood, and daytime productivity and the quality of relationships improve with treatment of OSA. 11,12 It is also recognized that relationship status impacts OSA. Previous studies have found that marital status has been associated with higher rates of OSA diagnosis and increased CPAP adherence. 13 -16 Marital status has been found to play an important role not only in OSA, but in the management of other comorbidities, particularly when examining survival. This is the first study to our knowledge that evaluates the impact of race and marital status on survival. Marriage demonstrates survival benefits for other chronic conditions such as diabetes and hypertension, particularly for married versus unmarried males. 11,17 -20
This study population is unique in the high rate of diversity. Previous studies have indicated gender but not taken into consideration diversity in results reported. Race also plays a role in survival in OSA. The literature demonstrates that Black individuals with OSA have greater risk of atrial fibrillation, poorer CPAP adherence, increased daytime sleepiness, and higher OSA associated cardiovascular risk. 21 -25 According to Dudley et al., OSA in Black individuals is generally more severe on diagnosis, suggesting that that there could be a delay in diagnosis. 26 However, there exists no analysis for OSA survival comparing Black patients and White patients by marital status in the literature.
While relationship status is associated with overall survival and comorbidity management for other chronic conditions, there are certain gaps in OSA-related research. 17 -20 The goal of the current study was to investigate the associations of marital status, race and age on the diagnosis, treatment course, severity, CPAP adherence, and overall survival in those with OSA.
Methods
Adults who had completed a polysomnogram between 2005 and 2015 within a single academic medical center and a diagnosis of OSA were included in the analysis. CPAP adherence was defined as use for at least 4 hours for at least 5 nights per week. Patient self-reported demographics, date of OSA diagnosis, date of CPAP prescription, results of preliminary polysomnogram, and follow-up appointments were chart reviewed from the polysomnogram report and encounters with sleep medicine. Patients were defined as married if they self-reported this in the electronic medical record demographics, while unmarried patients were defined as not having the demographic status of “married” in the electronic medical record (e.g., single, divorced, widowed, and partnered).
All categorical data are reported as counts and column percentages; while all continuous data are described using means, standard deviations, medians, minimums, maximums, and quartiles. Univariate two group comparisons between married and unmarried patients were assessed using T-tests for normally distributed continuous variables, Wilcoxon rank sum test for continuous variables which are skewed, and using chi-square or Fisher’s exact tests if cell counts were < 5 for categorical variables. Univariate and multivariate survival analysis using Cox regression were performed. Hazard ratios and the corresponding 95% CIs are reported to examine survival since OSA diagnosis date, as well as survival since CPAP diagnosis date. Survival was calculated from the OSA diagnosis date and the last date the patient was known to be alive. CPAP survival was this same difference from first CPAP prescription. Kaplan–Meier survival estimates are computed and graphed. Statistical significance was set at P < .05. All analyses were performed using SAS 9.4 (SAS Institute Inc., Cary, NC). This study was reviewed and approved by an institutional review board at Henry Ford Health #11382-29. Data available upon request. There is no conflict of interest nor funding for this project.
Results
Demographics of Patients.

SD, standard deviation.
Married patients were 7.77 years older at the age of OSA diagnosis and an average of 6.69 years older at first prescription of CPAP. Additionally, married people had lower mean sleep efficiency compared to those who were unmarried (76.2 and 77.2, respectively; P = .019). There was no significant difference in apnea-hypopnea index (AHI) or oxygen saturation nadir between groups. On average, patients had a sleep efficiency score that decreases by 0.2% for every year older a patient is at OSA diagnosis (P < .0001).
OSA, Marital Status, and Survival
Overall, patients that were married had increased survival probability over the years (P < .0001) (Figures 1 and 2; Table 2 and 3). Mean years of follow-up was 5.82 and 5.87 years (standard deviation 4.01 and 3.93) for married and unmarried patients, respectively. When controlling for age at first CPAP prescription, gender, and sleep efficiency, those that were unmarried have 2.00 times higher risk of death since CPAP prescription than those that were married (95% CI 1.58–2.54). Every 1-year increase in age at first CPAP prescription was associated with a 1.02-fold increased risk of death (95% CI 1.01–1.03) since CPAP prescription when adjusting for marital status, gender, and sleep efficiency (Table 2). When controlling for age at OSA diagnosis, gender, and sleep efficiency, those that were unmarried have a 2.72 times higher risk of death since OSA diagnosis than those that were married (95% CI 1.76–4.20). Every 1-year increase in age at diagnosis of OSA was associated with a 1.04-fold increased risk of death (95% CI 1.02-1.06) when adjusting for marital status, gender, and sleep efficiency (Table 3). Kaplan–Meier curve of overall OSA survival by marital status. Abbreviations: OSA, obstructive sleep apnea. Kaplan–Meier curve of overall CPAP survival by marital status. Abbreviations: CPAP, continuous positive airway pressure. Multivariate Survival Models: Survival Since CPAP Prescription. CPAP, continuous positive airway pressure; HR, hazard ratio; OSA, obstructive sleep apnea. Multivariate Survival Models: Survival Since Obstructive Sleep Apnea Diagnosis. Note: * indicates statistical significance



OSA, Self-Identified Race, and Survival
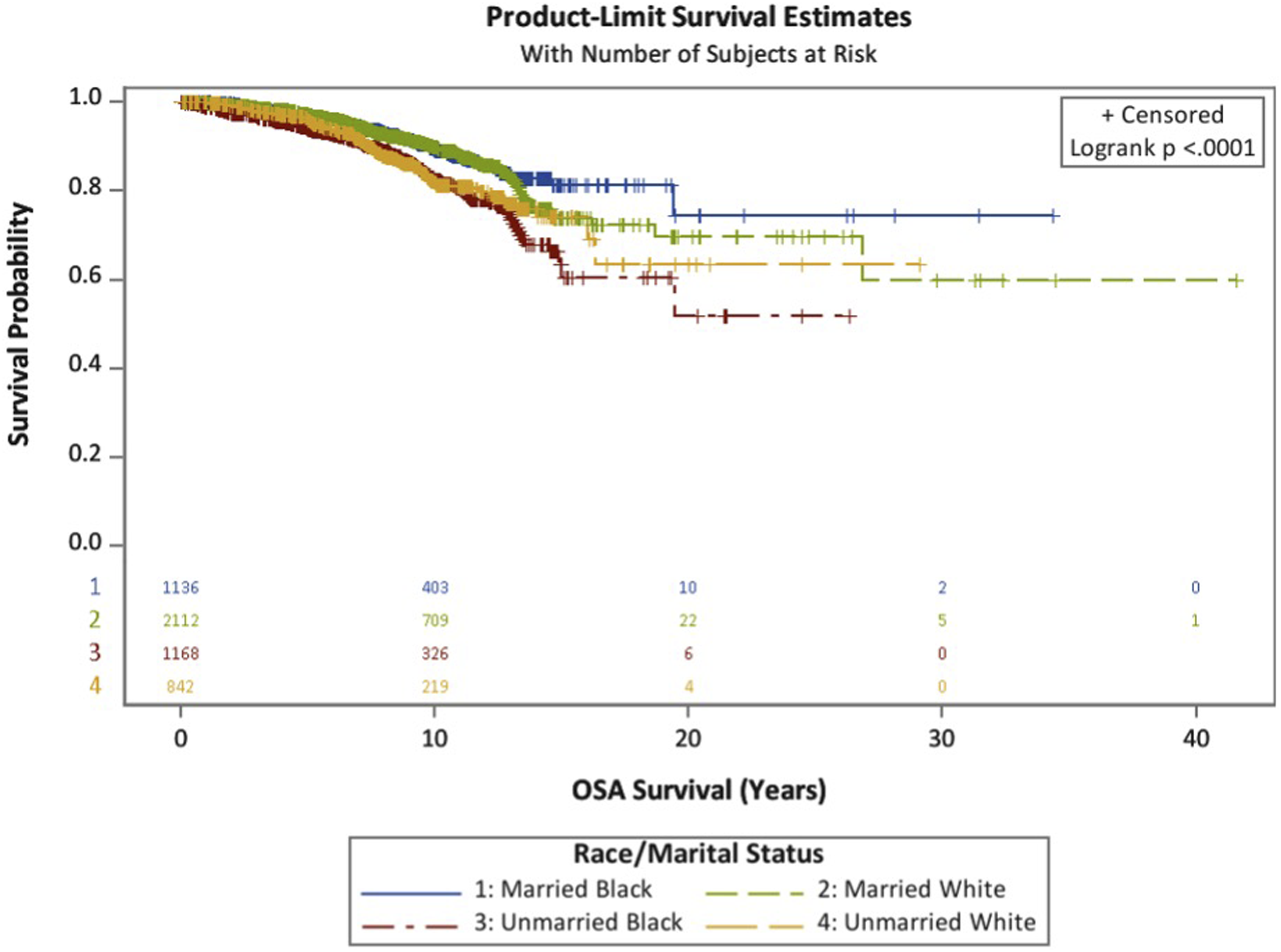
Only White and Black patients were included in analysis of race (n = 5649). No significant differences in survival since OSA diagnosis was observed between Black and White patients as a whole (P = .14) (Figure 3). However, when race and marital status together were studied, there were differences in survival between the groups. Married Black patients demonstrated the best survival probabilities, followed by married White patients (P < .0001) while unmarried White patients and unmarried Black patients did not display differences in survival (Figure 4, Table 4). When controlling for age at OSA, gender, and sleep efficiency, married Black patients had a 0.58 (95% CI 0.44–0.76) reduced risk of death since OSA diagnosis compared to unmarried White patients, while married White patients had a 0.54 (95% CI 0.43–0.70) reduced risk of death since OSA diagnosis compared to unmarried White patients (Table 4). Kaplan–Meier curve of overall OSA survival by race. Abbreviations: OSA, obstructive sleep apnea. OSA survival by race and marital status. Abbreviations: OSA, obstructive sleep apnea. Marital Status and Race: A Multivariate Table Below is Looking at Survival Since OSA Diagnosis When Adjusting for Race and Marital Status Combined. Note: * indicates statistical significance, HR, hazard ratio; OSA, obstructive sleep apnea.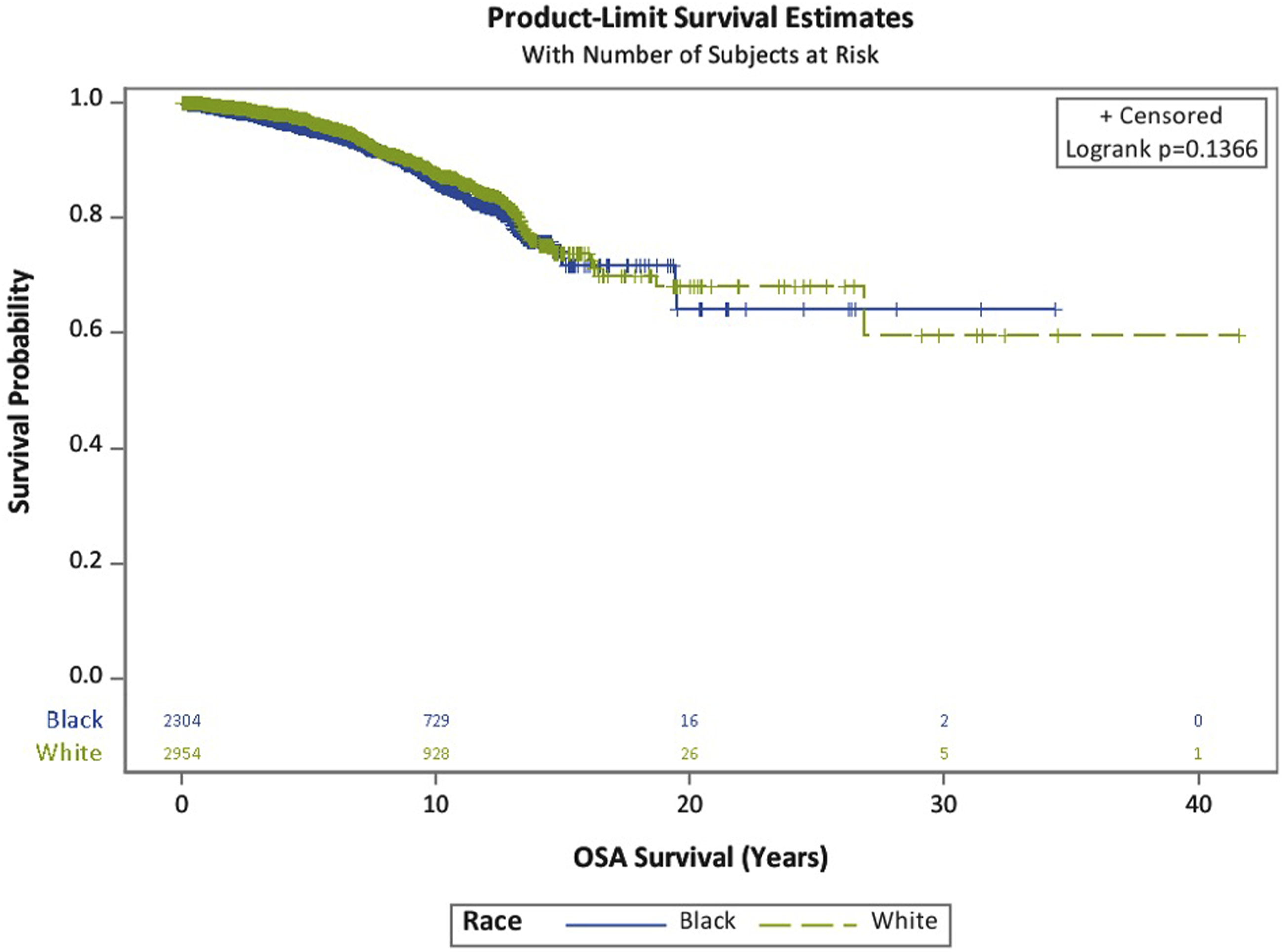

Discussion
The current study examined the associations between marital status, race and age and the diagnosis, treatment course, severity, CPAP adherence, and overall survival in those with OSA. In congruence with general health literature indicating survival benefits of marital or relationship status, the current study demonstrated that married patients diagnosed with OSA have better survival. Previous research in OSA, comorbidities, relationship status, and survival has found similar associations. These studies postulated that, while OSA can result in multiple comorbidities including cardiovascular disease, diabetes, and neurocognitive disorders, those that are married may have improved management of these conditions due to the partner’s involvement in assisting with medications and appointments. 18,19 This is important to note, as marital or relationship status is also considered a social determinant of health. 17 Those who are married tend to have better survival, especially males, compared to their unmarried counterparts. One hypothesis for this is that there is a selection bias for those who are already unhealthy at baseline to be unmarried. 17 -20 Interestingly, Lund et al. found that living arrangements, such as cohabitation had a larger impact on health than marital status, indicating that intimate partnership (i.e., the presence of an invested significant other) rather than legal marital status may be more significant to one’s health. 27 For some chronic diseases, such as Type II diabetes, there is increased risk of developing the disease for widowed compared to legally married or single males. 19 Similarly, hypertension was found to have increased mortality for unmarried compared to married males. 20 Survival in the married versus unmarried patients in OSA appears to align with these other chronic diseases.
Married individuals had better survival than their unmarried counterparts across race. It is known that Black patients experience higher overall mortality than their White counterparts, though this gap is narrowing. It has been found that in terms of OSA, Black patients have greater risk of associated comobidities. 21 -26 The current study found that married Black patients with OSA had the best survival, which has not been examined to this scale in the literature previously.
Limitations of this study include that, based on the conceptualization of “married” in this study, there may be unmarried people who still have a regular or frequent bed partner or an intimate relationship. Indeed, those patients who were divorced/separated or widowed were considered unmarried; thus, the prior contributions of a consistent partner to survival were not taken into account. Moreover, only Black and White races were examined as a sub-analysis in this study, other races were only included in totals, due to smaller sample size. Comorbid conditions were also not included in analysis, which could have an impact on survival and be a confounder in marital status. A strength of this study is the inclusion of a large population of Black patients and is the largest minority population in an OSA survival study to authors’ knowledge.
Conclusion
The current study demonstrated that in patients diagnosed with OSA being married was associated with improved survival compared to unmarried counterparts. Married Black patients had the best survival. Future research should examine changes in relationship status as it relates to changes in health status, in particular CPAP adherence, comorbidity, survival, and health care equity. Research should also examine the outcomes with an expanded definition of relationship status to include partnered but not legally married individuals.
Footnotes
Author contributions
Madeline Goosmann, MD: design, conduct, writing, presentation of research. Amy Williams, PhD: design, writing and editing, Kylie Springer, MS: statistical analysis of data. Kathleen Yaremchuk, MD, MSA: design, editing
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.