
Abstract
Ulcerative necrotic supraglottitis is a rare entity of laryngeal infection leading rapidly in laryngeal necrosis, systematic complications and potentially fatal outcomes. We present a case of a 50-year-old gentleman with ulcerative necrotising supraglottitis and no co-morbidities who presented in Ear Nose and Throat Service in the Accident and Emergency department due to dysphagia and weakness. He was treated with an emergency tracheostomy with neck exploration and washout and received appropriate supporting antibiotic regime. He improved and was eventually decannulated, able to breathe phonate and swallow appropriately. After a thorough review of the literature regarding necrotising infections of the laryngeal cavity, only 7 cases have been reported, all in immunocompromised patients with severe complications. Our case report is the first ulcerative necrotic supraglottitis in a healthy individual who was treated early and aggressively with impressive results.
Keywords
Introduction
Necrotising infectious diseases such as necrotizing fascititis are life threatening conditions that affect multiple parts of the human body and are attributed to a combination of different aerobic and anaerobic microorganisms. The condition starts as a common infection of the mucosa or skin and continues to spread in an uncontrolled and extremely rapid way which results in late diagnosis and treatment as well as discouraging outcomes. Predisposing factors are immunosuppression, diabetes mellitus, chronic liver conditions, renal insufficiency and malignancy. Early diagnosis and treatment with appropriate antibiotics as well as in some cases surgical management is vital to achieve healing.
Necrotising supraglottitis is a rare and rapidly progressive infectious disease of the laryngeal cavity that primarily involves the supraglottis. Most commonly, it begins from the mucosa, fascia and subcutaneous tissue and continues spreading to the cartilage and muscles.1-3 It is a result of several microorganisms that cause infection and tissue necrosis with subsequent tissue break down, with formation of cavities and accumulation of purulent discharge. The wide variety of bacteria as well as concurrent co-morbidities of the patients allow a rapid progress of the disease in the laryngeal cavity, surrounding muscles, trachea and even distant organs that can be affected and evidently, skin.
Case presentation
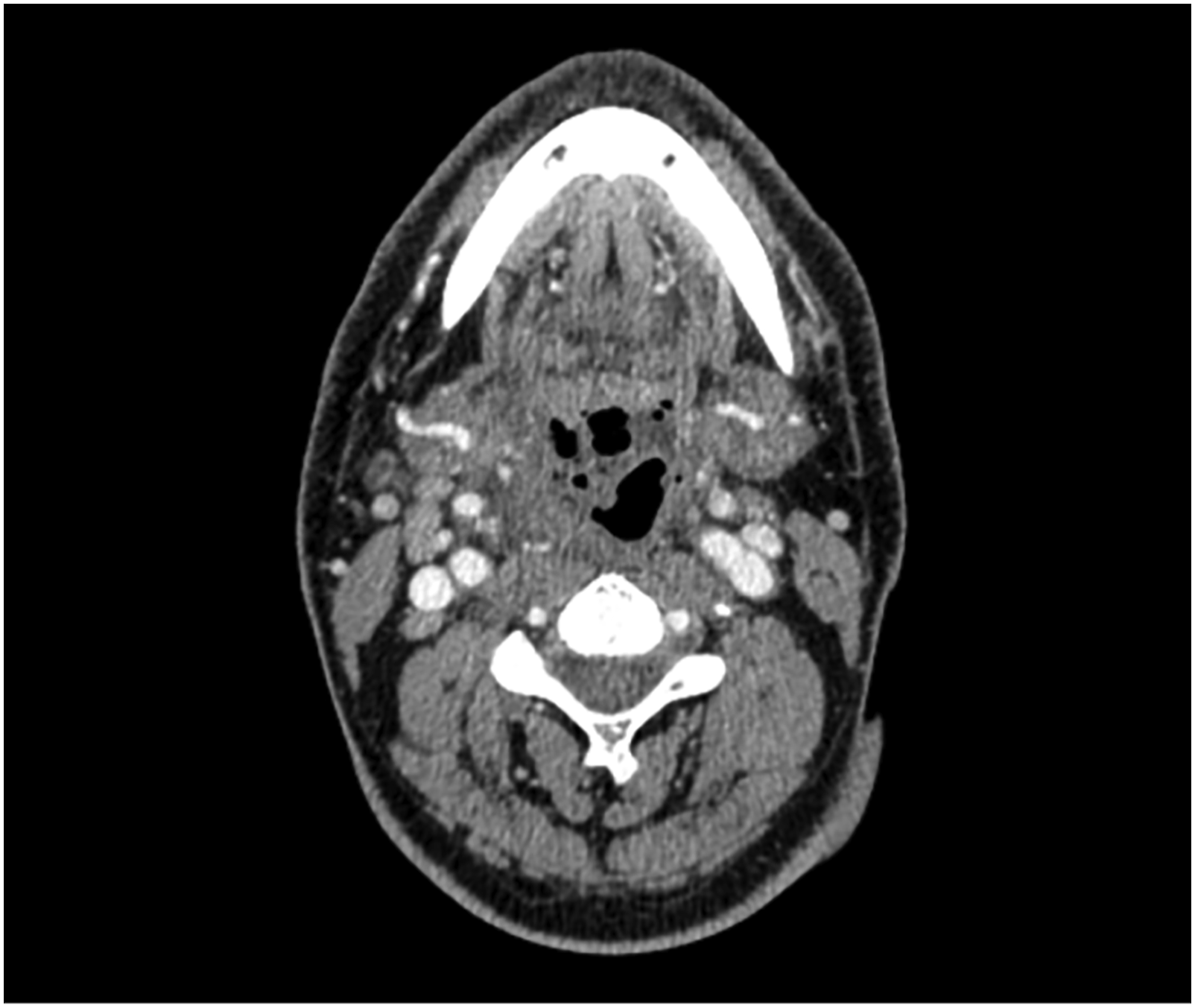
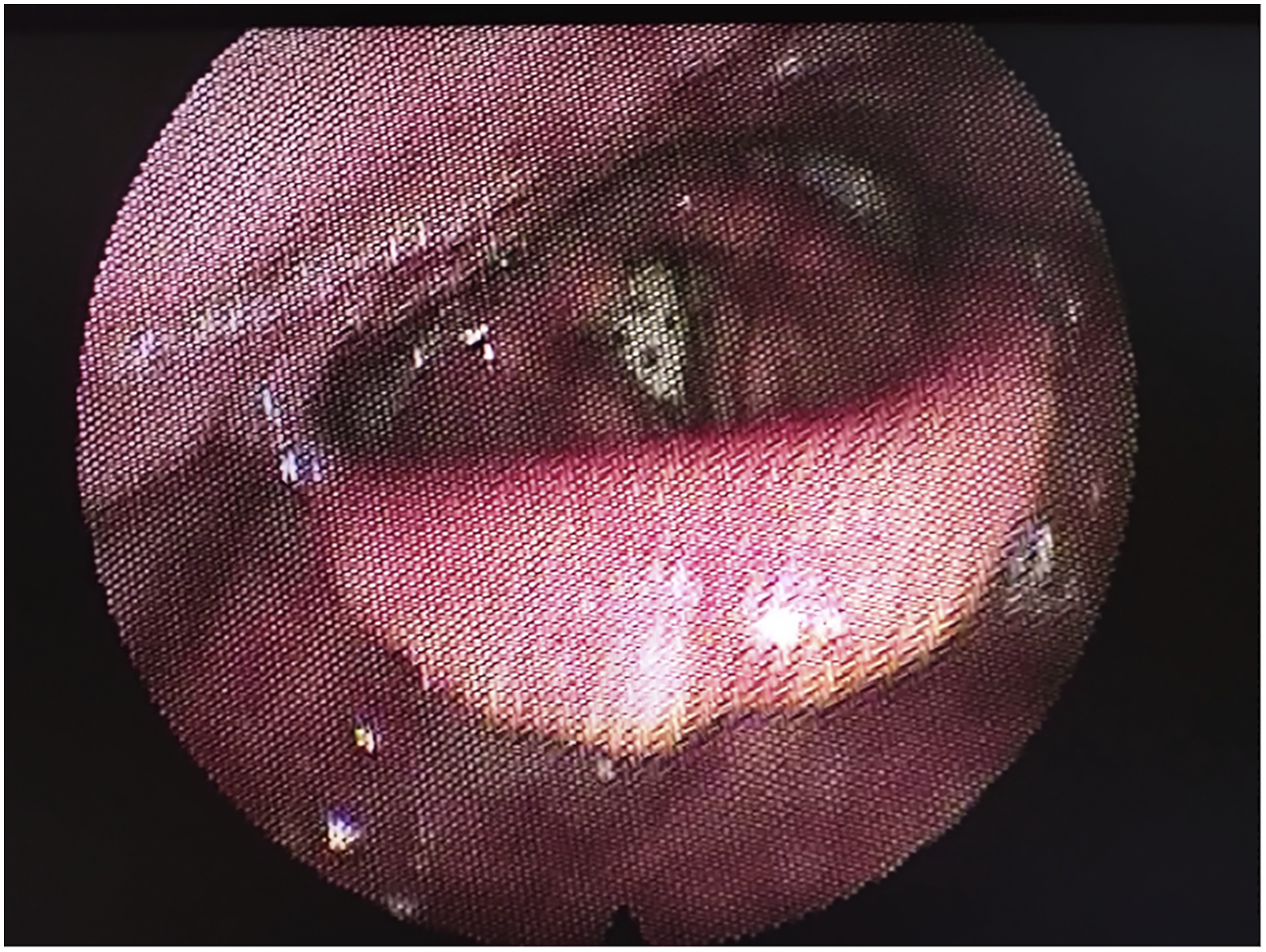
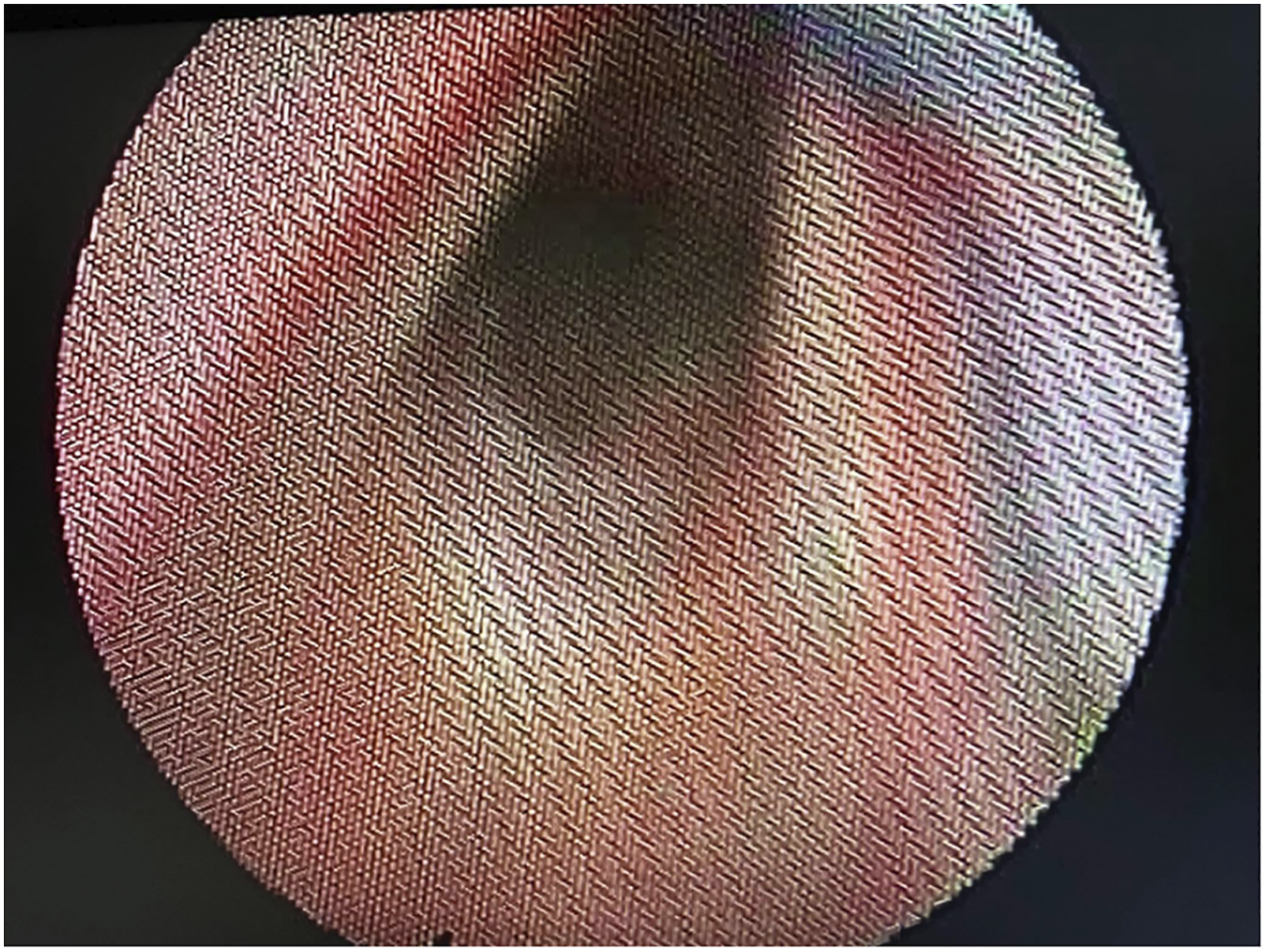
We present a case of a 54-year-old gentleman with ulcerative necrotising supraglottitis who presented in Ear Nose and Throat Service in the Accident and Emergency department due to dysphagia and weakness. He had symptoms for less than 24 hours and had progressive difficulty in swallowing solid and fluid material as well as temperature at 39°C and concurrent muscle aches. He denied any cough or cold and any other symptom when asked. He had no co-morbidities apart from high blood pressure and no previous similar episodes. He underwent a full Ear Nose and Throat examination including flexible nasoendoscopy that revealed an ulcerated necrotic supraglottis, mainly involving the right arytenoid cartilage and an extremely swollen epiglottis with no evident necrotic area but obstructing the airway (Figure 1). Amazingly, he was experiencing no difficulty in breathing and the dysphagia he described was disproportionate to the necrotic area that was observed during flexible nasoendoscopy. He was immediately discussed with microbiology department and was started on broad spectrum antibiotic treatment and appropriate resuscitation. He had a CT scan of his neck and chest that showed local necrosis, subcutaneous air and multiple abscess formation (Figures 2 and 3) and his blood was analysed, blood cultures were sent and was reviewed by internal medicine as well as infectious disease teams while being prepared for theatre. He underwent an emergency tracheostomy with a combined external and endoscopic approach to drain the abscesses and remove the necrotic tissue remnants. He required multiple washouts and double drain placement. His blood tests showed severe infection and inflammation with high white cell count and neutrophilia, raised inflammatory markers and prolonged clotting time. Histology results showed necrosis with neutrophil and reactive cells infiltration of the laryngeal tissue specimen. During his hospitalisation, he was initially kept nil by mouth while after multiple flexible endoscopic examinations and a formal swallowing test, started tolerating oral intake. Also, when his airway was established and the necrotic area was healed, he was decannulated. Thankfully, our patient improved on antibiotic treatment, required two more re-look operations under local anaesthetic to address local infection and was subsequently discharged (Figures 4 and 5). Flexible nasoendoscopy on admission. Flexible nasoendoscopy before decannulation (The tracheostomy tube is also visible). Healthy laryngeal cavity post treatment. CT scan of the neck on admission (vocal cord level). CT scan of the neck on admission (hyoid level).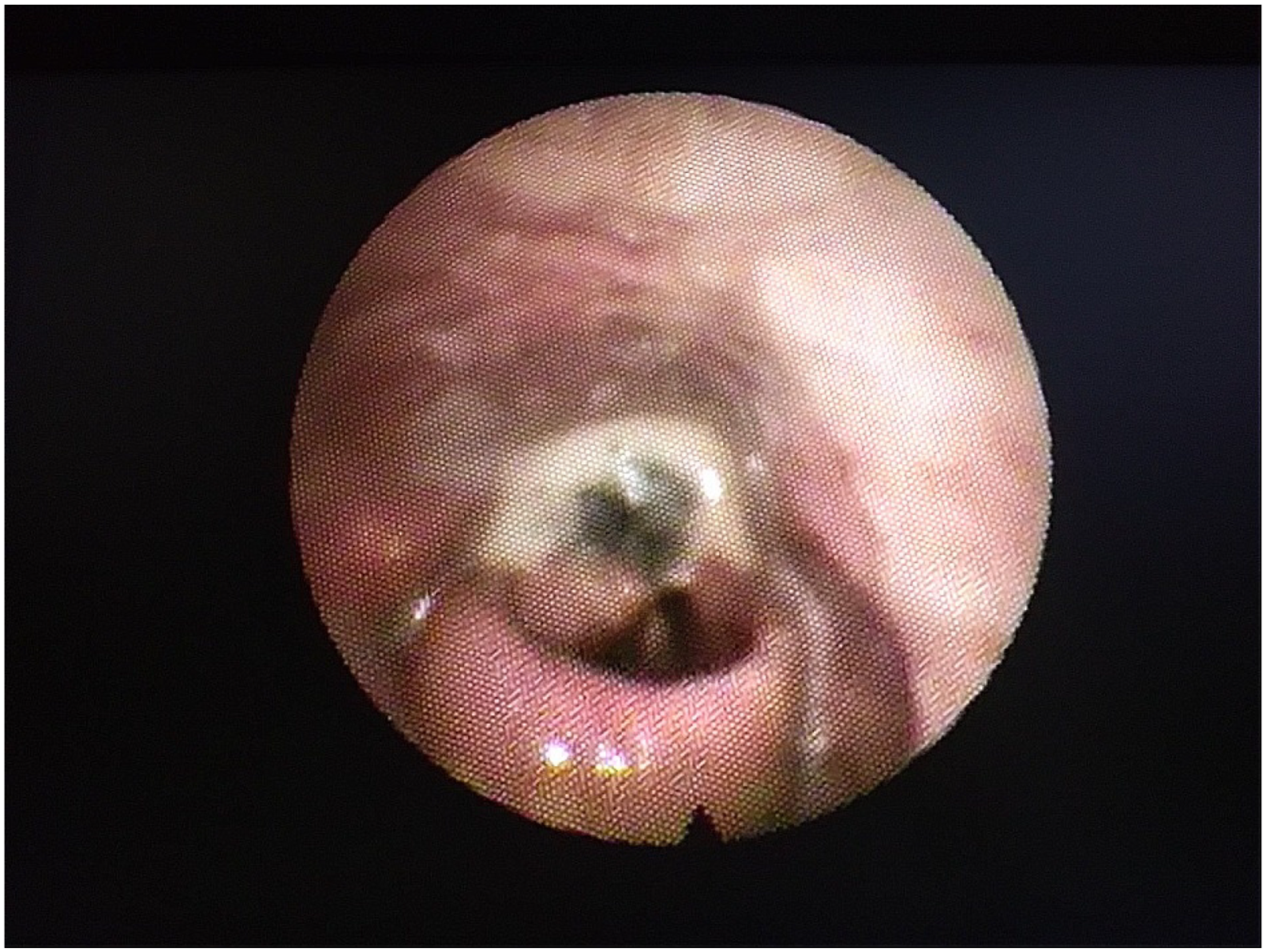

Discussion
In 1952, Wilson et al. introduced the term necrotizing fasciitis that described a rapid and progressive inflammation mainly involving the subcutaneous tissue, superficial and deep fascia with concurrent presence of cutaneous gangrene. Since then, there is a lot of research on the pathogenesis and pathophysiology of the condition in an attempt to prevent rapid expansion and late diagnosis.
In most cases, patients present with pain, temperature and erythematous swollen affected areas that in the beginning may not seem necrotic. 4 They deny symptoms earlier and describe a rapid and severe spread of the disease. In our case, our patient had no previous symptoms and his absolute dysphagia developed in about four hours after the onset of the condition. Next step, if left untreated, his airway would be compromised due to severe inflammation and necrosis of the larynx leaving them with a permanent tracheostomy and swallowing problems at the best scenario. Our patient had no other severe co-morbidities – he is a smoker with hypertension – or any history related to alcohol consumption that is correlated with compromisation of the natural barriers in the oral cavity, decrease of saliva production that results in increased concentration of microorganisms.
In terms of the pathogens, Streptococcus group A and Staphylococcus aureus seem predominant while other gram negative aerobic micoroorganisms are involved, too. 5 In our case, no such pathogen was isolated apart from Acinetobacter that was treated with a combination of meropenem, tigecycline and colistimethate sodium for three weeks according to microbiology advice. It is questionable, the choice as well as the course of antibiotic treatment in such complex cases but we advocate early and aggressive treatment to prevent severe disability and fatal outcomes. 6 Surgical treatment with an emergency tracheostomy and subsequent debridement proved to achieve an effective and safe airway with removal of all necrotic tissue to enhance recovery and healing. Again, this could be considered as overtreatment since surgical exploration was performed on admission without having 48 hours of antibiotic treatment first, however, removal of necrotic parts and leaving drains in the cavities promoted cleaning and healing of the area to ensure quicker recovery.
Blood testing normally reveals elevated white cell count, raised inflammatory markers, altered coagulation profile and decreased protein concentration. 5 These results can be associated with multiple infectious diseases or inflammatory conditions so clinical examination and imaging is key. 7 Imaging with a normal xray or with CT of the affected area, reveals local swelling, with debris and free air in small cavities that have been forming for the past few hours. Repeating CT in a short period of time before treatment starts might show significant difference to the worse.
Conclusion
Necrotising supraglottitis is a rapidly spreading cervical infection that is normally seen in immunocompromised patients. 8 The infection is due to multiple aerobic and anaerobic pathogens and requires numerous surgical operations and strong antibiotic regimes with sometimes significant morbidity or even fatal outcomes. We present a necrotizing supraglottitis in an immunocompromised patient that was addressed with an emergency tracheostomy, incision, drainage and washout with supportive antibiotic therapy. Since his treatment was aggressive from the beginning, no further surgical operations were required and the patient was subsequently decannulated, able to breathe, swallow and phonate with impressive results. We therefore advocate early and aggressive approach to necrotizing supraglottitis to ensure effective treatment and complete recovery.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.