
Abstract
Keywords
Introduction
Chronic suppurative otitis media (CSOM) is a kind of chronic inflammation of the middle ear (ME) mucosa and submucosa which is often accompanied by inflammation of the mastoid process. 1 The inflammation in the ME can affect the thickness of mucosa and the flow rate of blood, so it may alter transmucosal gas exchange and affect the ME total pressure. 2 One of the most important conditions for maintaining the ME function is the balance of the gas pressure. 3,4 For most CSOM, surgery is the main choice. The goals of CSMO surgery are to improve the ventilation of the ME and eradication of disease with a dry, safe ear. 5 Two techniques commonly used by ear surgeons are intact canal wall tympanoplasty (ICWT) and canal wall down tympanoplasty (CWDT). In 1984, Paparella first described the steps of intact bridge tympanomastoidectomy (IBM), 6 but the jury is still out on the long-term effects of IBM’s surgery. 7,8 In this study, we aimed to review the long-term hearing outcomes of IBM to discuss hearing preservation and possible theoretical basis.
Materials and Methods
Patients
We reviewed the records of subjects who had IBM for CSOM treatment. Our research included 102 patients who were able to follow-up with detailed data from nonselective, retrospective patients with CSOM who had experienced IBM. Our research group selected 102 patients from non-cholesteatoma otitis media patients who were operated on at the Eye & ENT Hospital of Fudan University from April 2007 to July 2017.
The mean age of the patients was 35.7±13.5 years (range from 8 to 64). This study was conducted in accordance with protocols approved by the Institutional Research Review Board at the Eye & ENT Hospital of Fudan University, Shanghai, China.
Surgical Technique
The lesions of these 102 patients located in attic and sinus tympani and damaged the balance of gas pressure in the ME. Postoperative pathology showed that the lesions were inflammatory granulation tissue or cholesterol granulomas. After intraoperative resection of the lesion, the water traffic between the entrance of the tympanum and the upper and middle tympanum would be detected. All subjects retained the lateral wall of the epitympanic and the ossicular chain.
Surgical Points
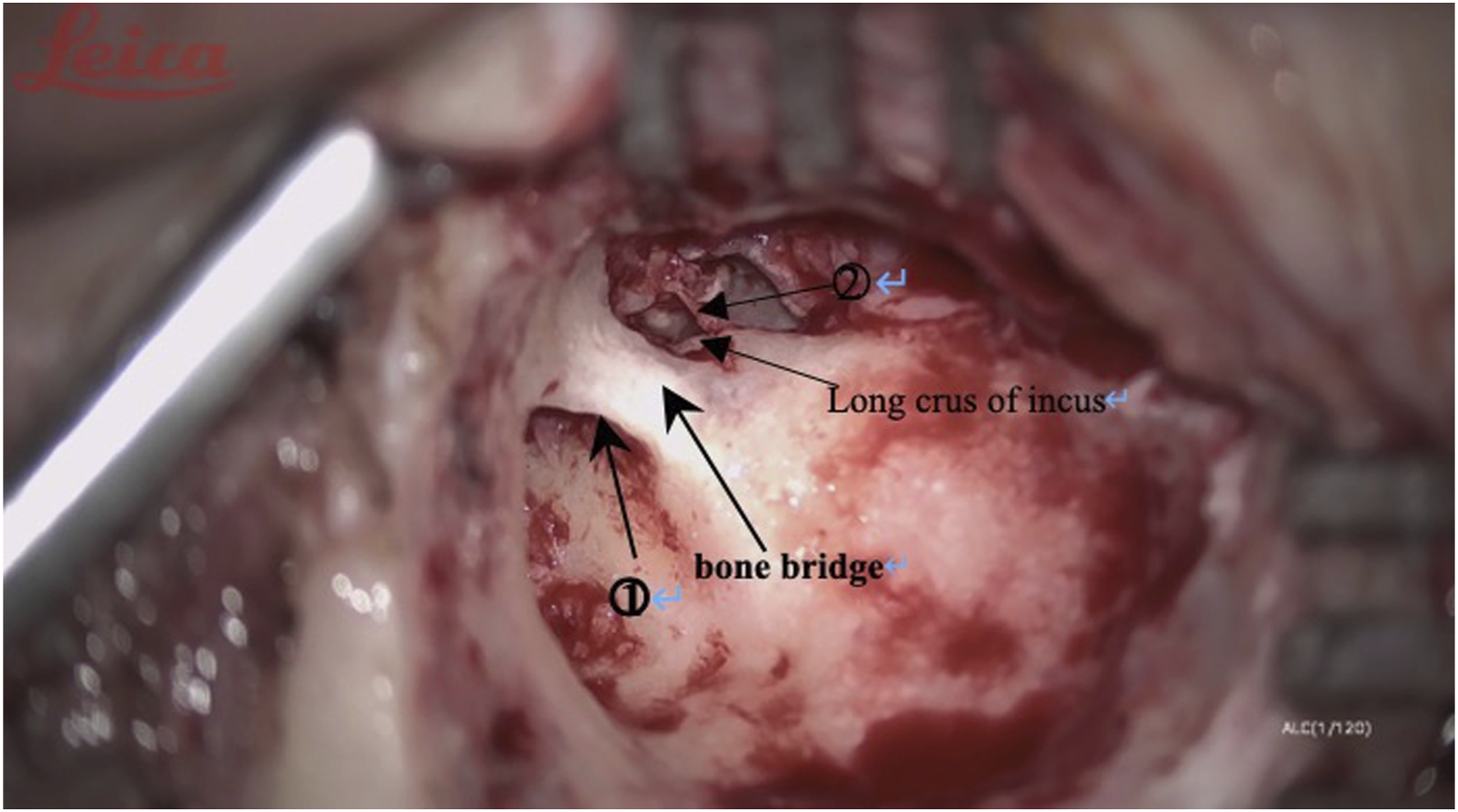
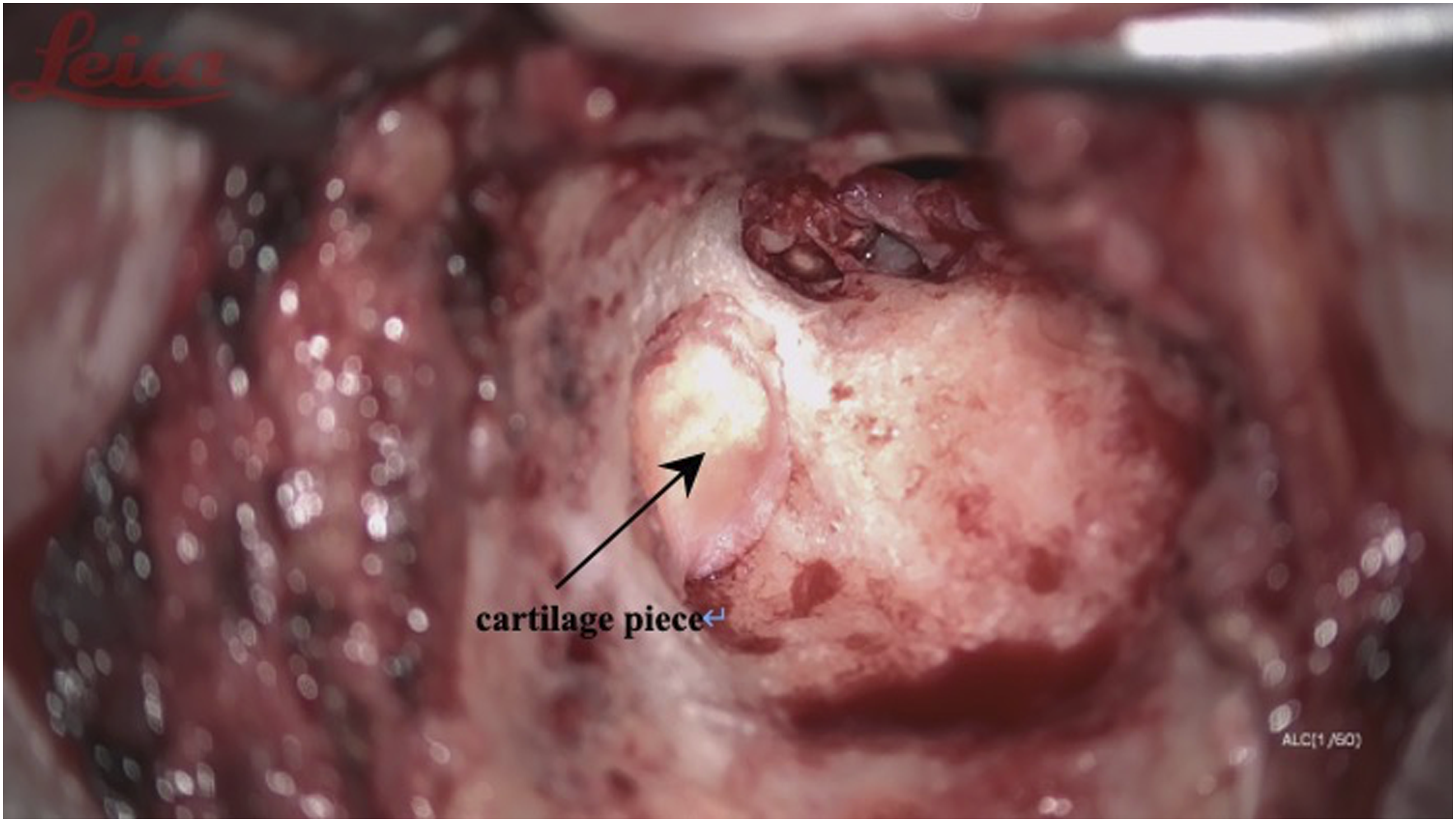
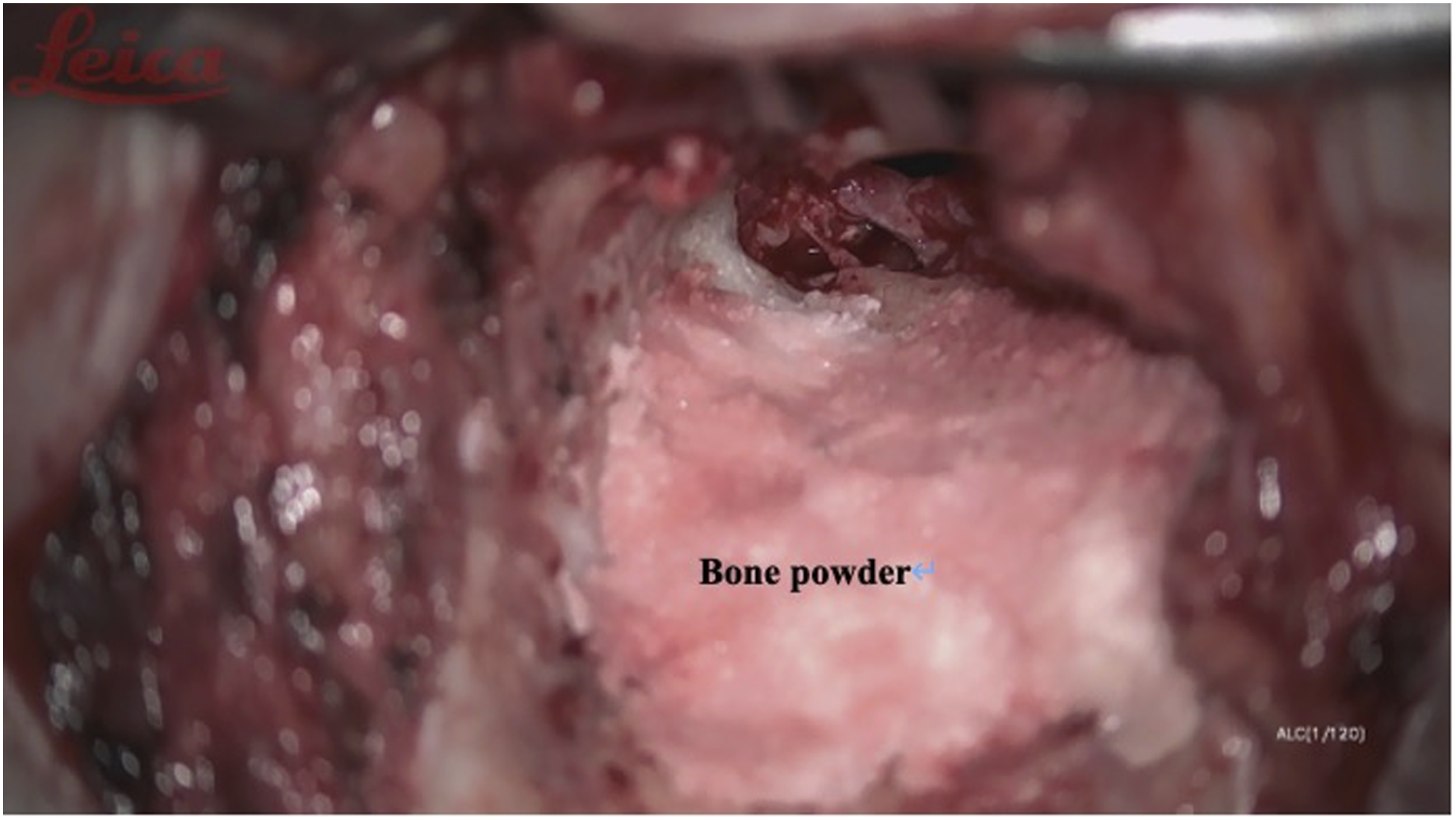
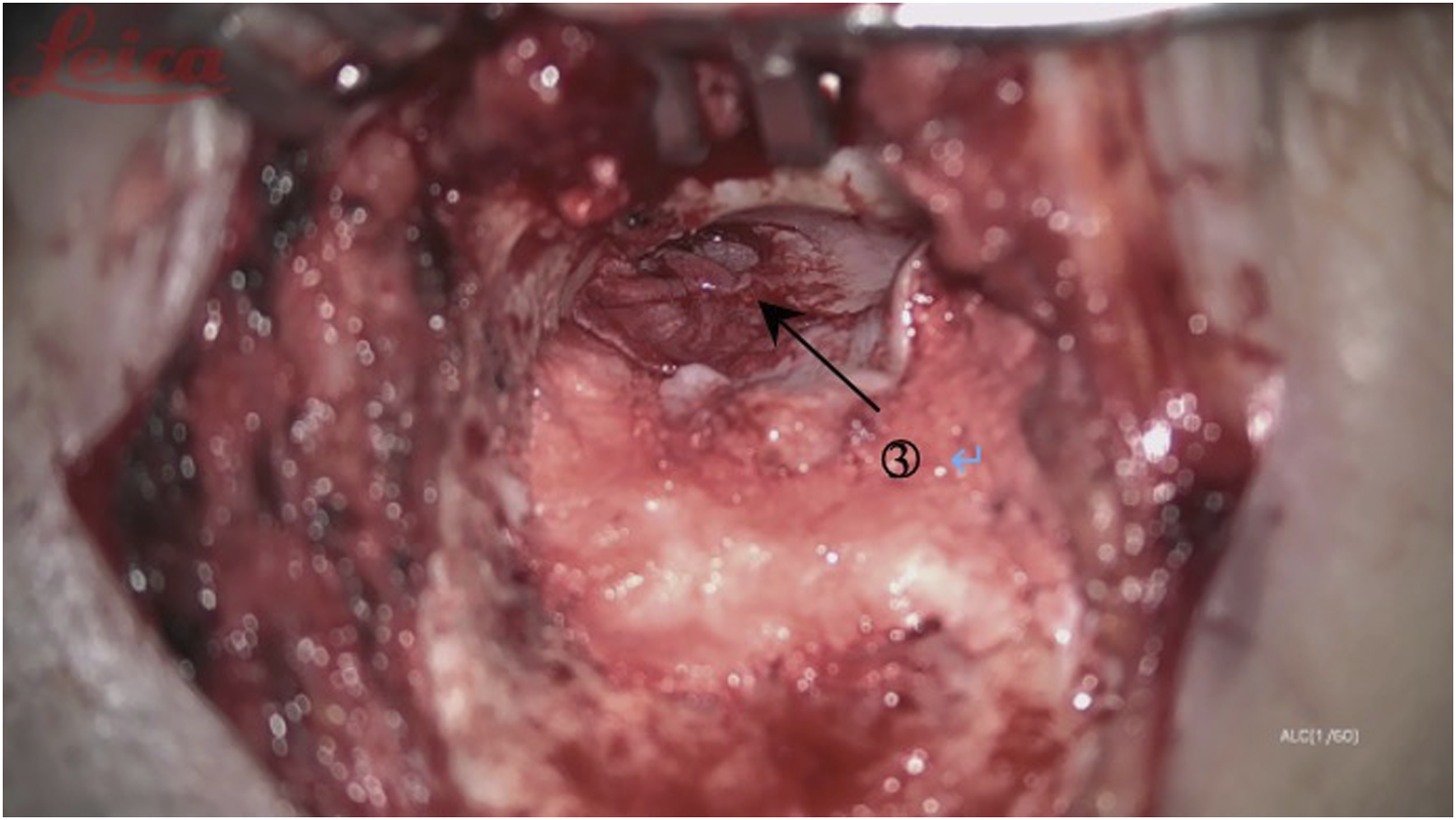
(1) Intact bridge tympanomastoidectomy surgical incision and mastoid contouring are the same as intact wall up tympanoplasty. Thoroughly contour the mastoid process and collect the bone powder of the mastoid cortical bone in preparation for filling the contoured mastoid cavity before the end of the operation; (2) Keep the bone bridge at the entrance of the tympanic sinus (Figure 1). It is important to avoid noise-induced hearing damage caused by the electric drill touching the ossicular chain; (3) Grind the lower facial nerve crest as much as possible to prevent the residual mastoid air cells from hiding the diseased tissue; (4) If necessary, the bone bridge at the entrance of the tympanic sinus can be narrowed to facilitate cleaning of the lesions obstructing the entrance of the tympanic sinus. The drainage of the tympanic sinus, epitympanum, and middle tympanum must be ensured during the operation (the water traffic test was unblocked); (5) Place the cartilage pieces removed during the formation of the ear concha cavity at the entrance of the tympanic sinus (Figure 2), and fill the outer mastoid cavity with bone powder to rebuild the external auditory canal (Figures 3 and 4); (6) When there are many air chambers inside the tympanic sinus, the tympanic sinus cavity can be reconstructed by covering it with a larger cartilage sheet and fasica to faciliatate the drainage of air from the medial air chamber. ①the entrance of tympanicantrum; ②chorda tympani; Place the cartilage pieces at the entrance of the tympanic sinus. Use the bone powder to fill the outer mastoid cavity. ③temporalis fascia (repair the tympanic membrane); Use the bone powder to fill the outer mastoid cavity. After that, Cover the repaired tympanic membrane and fascia on the bone powder.
Postoperative Management and Follow-Up
Postoperative intravenous uses antibiotic treatment. Fill the external auditory meatus with chlortetracycline gauze and orally take antibiotics for 10 days. The postoperative follow-up is about 7 to 10 days to take out the external auditory canal gauze. Next, wash ears with levofloxacin ear drops (6 drops each time for 10 min) and the absorbable gelatin sponge filled during the operation will flow out. Follow-up is required at 1 month, 3 months, and 1 year after surgery, which can be extended for 6 to 12 months. All patients were followed up for .5 to 3 years, with an average follow-up of 9.1 months and a median of 6 months. The mean follow-up period of less than 6 months was 4.5 months with a median of 5 months, and the follow-up period longer than 6 months was 15.9 months with a median of 9 months. Three months after the operation, use pure tone threshold to detect the hearing level of the affected ear and observe tympanum status, perforation, recurrence, mastoid epithelialization, and pure tone threshold at the same time.
Statistical Method
SPSS25 software was used to conduct paired T-test on the difference values of preoperative and postoperative pure tone average air-bone gap. The short-term and long-term effects were statistically analyzed by unpaired T-test. Gpower software was used to calculate the power value.
Result
Status of Ear Canal and Tympanic Membrane
After the operation, the external auditory canal of all patients was in normal shape and had a self-cleaning function. Of the 102 patients, 100 (98.0%) had intact tympanic membranes at follow-up. Among the 2 patients with incomplete tympanic membranes, 2 cases had preoperative tympanic membrane perforation greater than 2/3 and the duration of ME abscess was more than 30 years.
ABG Decreased Significantly After Surgery
Comparison of Pre- and Post-Operation Hearing Level.
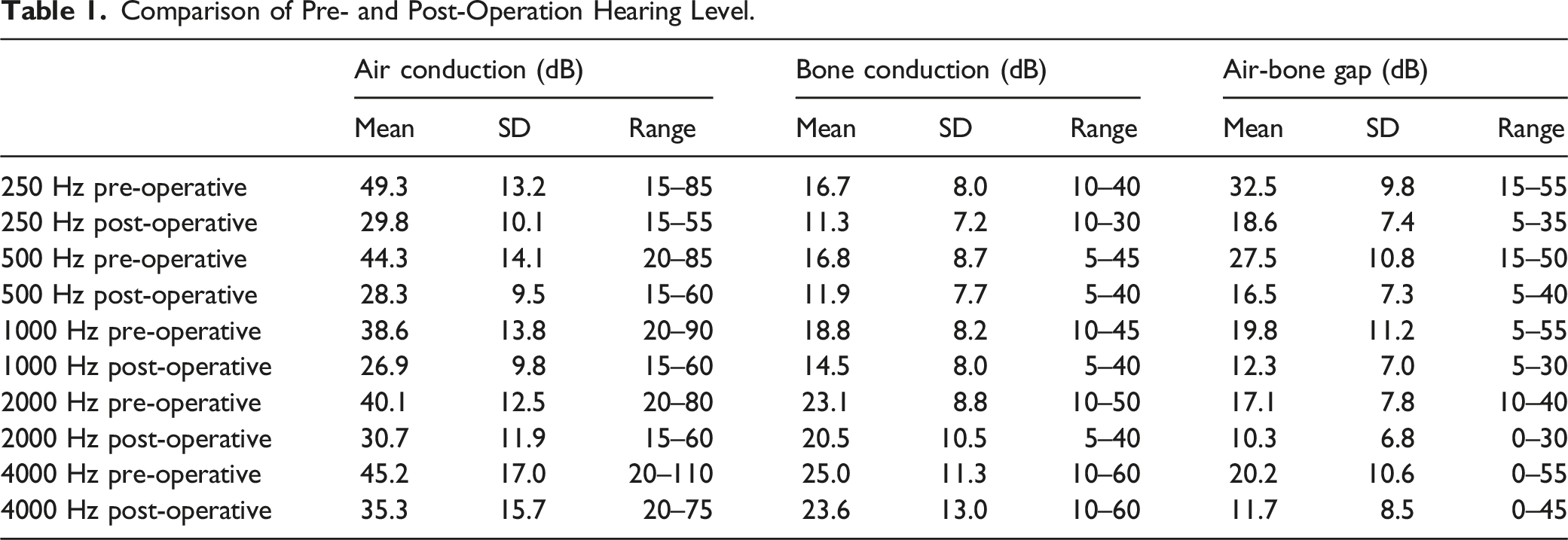
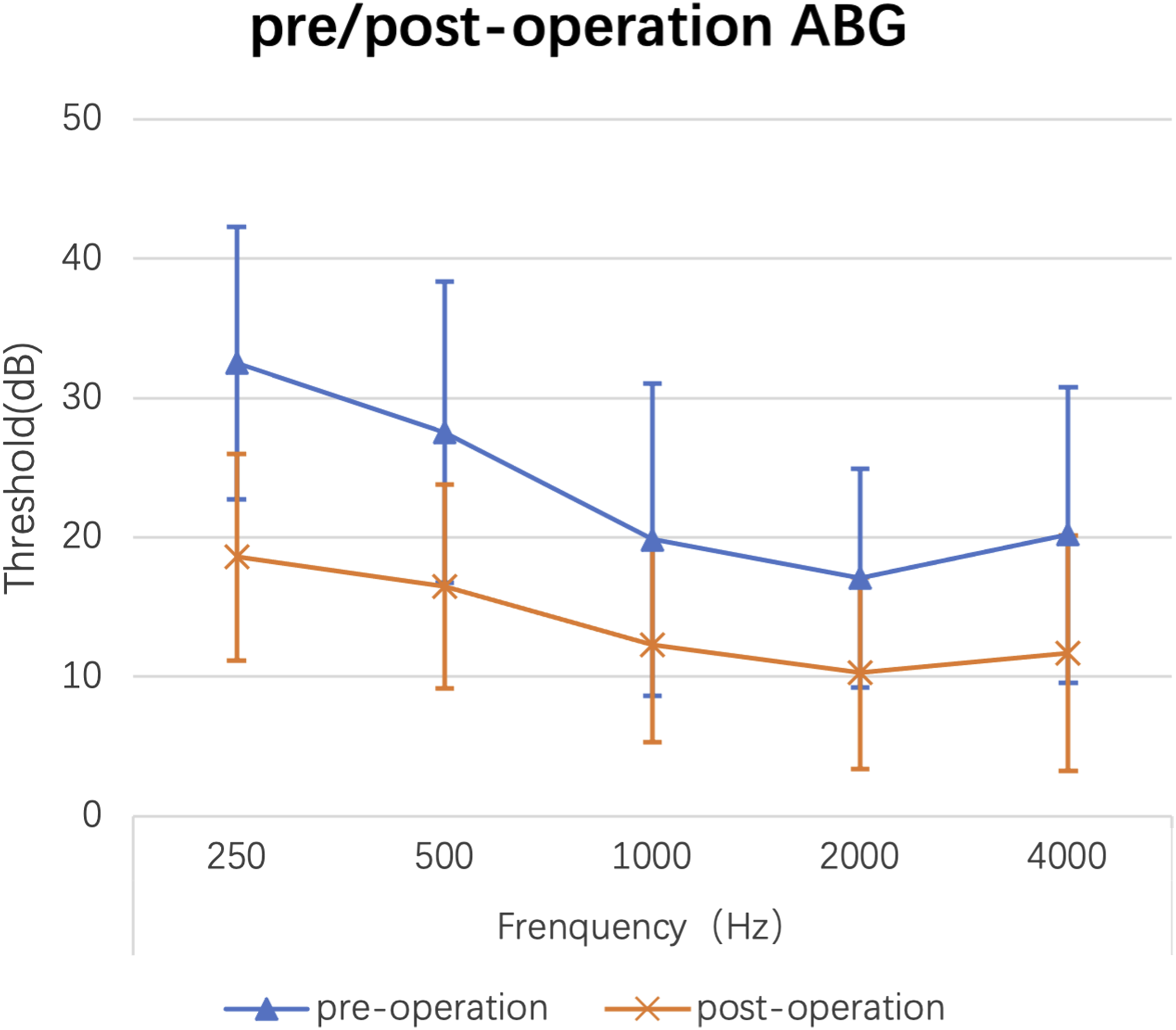
Comparison of pre- and post-operation hearing level.
Serviceable Hearing Post-operation (ABG < 20 dB)
Overall, 96/102 (94.1%) of patients obtained serviceable hearings in more than 3 frequencies with ABG <20 dB. The hearing level of 3 (2.9%) patients was lower than that before surgery. These patients had ME abscesses for more than 10 years (17, 30, and 40 years). We believe that the cause of postoperative hearing loss in these patients is related to the severe damage to the ME structure.
The Hearing Result Is Stable for a Long Term Follow-Up
Difference Between Long-Term and Short-Term ABG After Surgery.
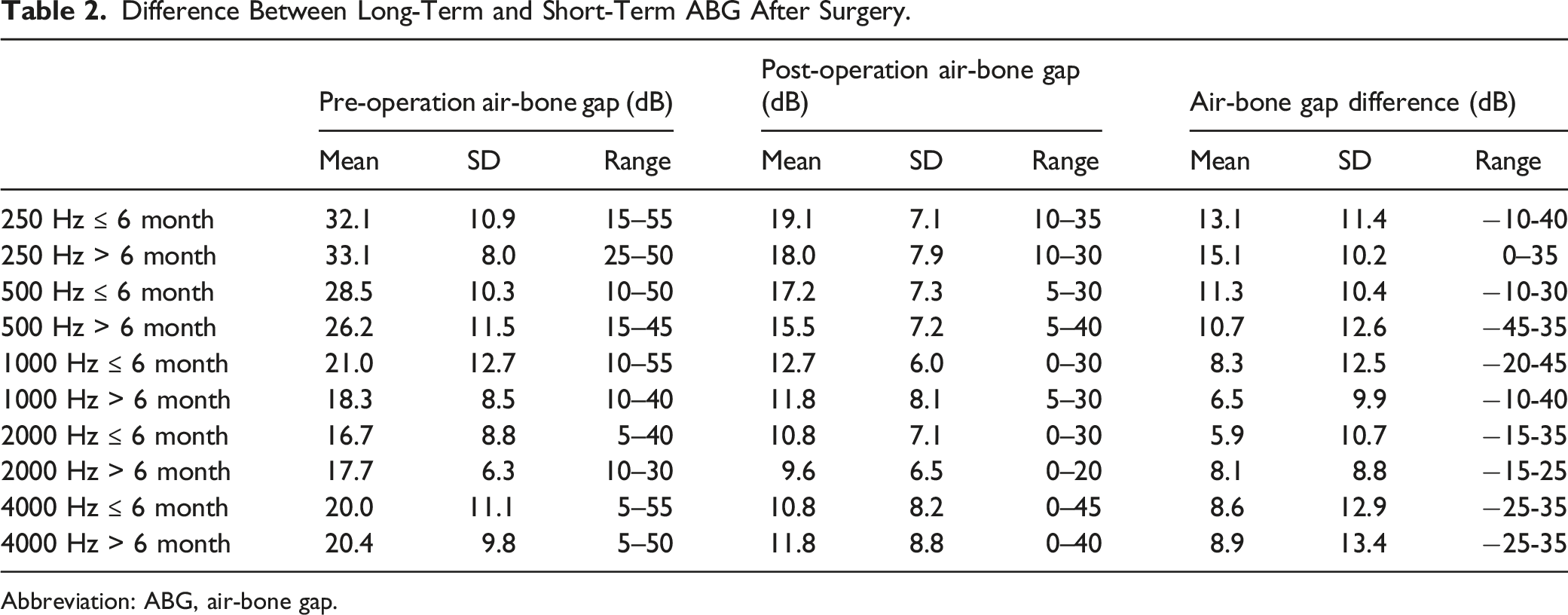
Abbreviation: ABG, air-bone gap.
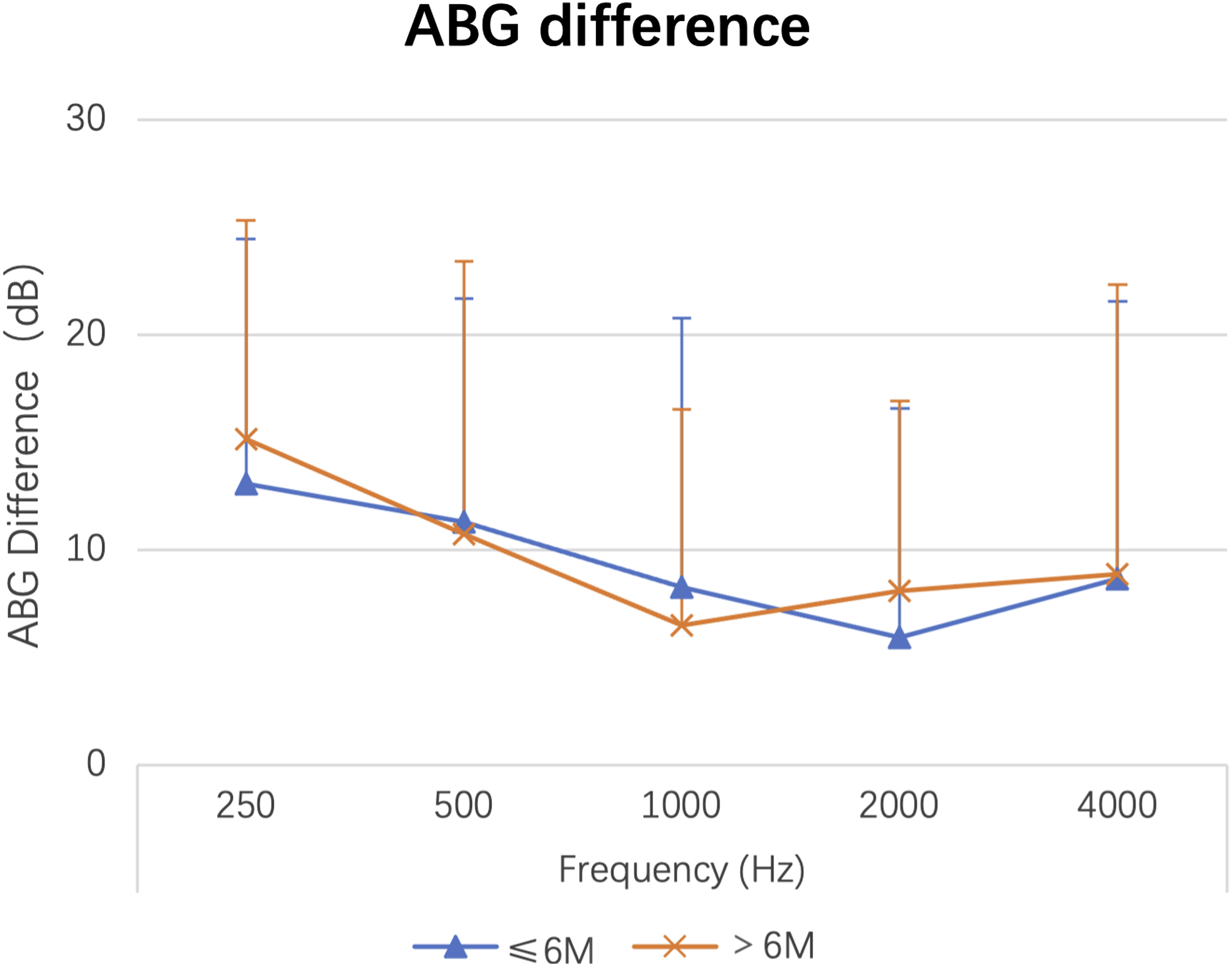
Short-term vs long-term hearing recovery.
Discussion
Intact bridge tympanomastoidectomy is an improvement of open tympanoplasty, which is suitable for patients with mild chronic otitis media with non-pneumatic mastoid lesions located in the tympanic antrum, epitympanic. 9 During the operation, at the entrance of the tympanic sinus, a water traffic test was performed and the result was unobstructed (i.e., water flow can be drawn into the midtympanic cavity after water from the mastoid cavity, and vice versa). It achieves the advantages of both closed and open cavity tympanomastoidectomy. 6 It can not only completely eradicate the disease but also preserve the bony structure which makes the ossicular chain stable. The operation does not require opening the epitympanum, but keeps the “bridge” to the external wall of the epitympanum and the entrance of the tympanum sinus. These operations we have done are to grind the “bridge” at the entrance of the tympanic sinus sufficiently low and narrow to facilitate cleaning of the lesions at the entrance of the tympanic sinus and adjacent epitympanum. The operation methods are similar to lower intact bridge tympanomastoidectomy.
99/102 (97.1%) of patients had hearing improvement in more than 3 frequencies after the procedure. Around 96/102 (94.1%) of patients obtained serviceable hearings in more than 3 frequencies with ABG <20 dB. 100/102 (98.0%) subjects had intact tympanic membranes at follow-up. Previous studies have reported that ABG less than 20 dB after ICWT can reach 80%-90%. 10 In previous study, the recurrence rate of patients with chronic otitis media treated with ICWT was about 7%. 11 Compared to ICWT, IBM has a lower frequency of relapse, but the long-term hearing effects achieved by IBM are comparable to other ICWT. 12 -14
One of the surgical goals of CSOM is to be able to reconstruct the tympanic airway path. Jacob Sadé first proposed the theory of “modified miniature lung” which means ME needs to breathe like a lung. 15 Therefore, the balance gas pressure plays one of the most important roles in maintaining ME function. The mastoid air cell system (MACS), the mucosal surfaces of ME, and the eustachian tube (ET) are also required to maintain the ME function. 3 In most patients, the only ventilation route to the epitympanum is through the tympanic isthmus. 16 A previous study found that even in patients with normally functioning ET, an isthmus blockage could cause dysventilation problems in the ME, leading to selective epitympanic dysventilation syndrome. 17,18
Intact bridge tympanomastoidectomy requires that after the lesions of the mastoid process and tympanum are removed intraoperatively, the water traffic between the entrance of the tympanum and the upper and middle tympanum is unobstructed, that is, no obstructive lesions are required in the epitympanum and the anterior tympanum. 9,19 Surgery ensures that there are no obstructive lesions in the tympanic isthmus, which provides conditions for long-term hearing maintenance.
Although the MACS acts as a pressure buffer, 20 it remains unclear what the contributions of the MACS and ET are. 21 James Belyea, Brandon Wickens, and Manohar Bance reviewed the subjects who underwent vestibular schwannoma resection with complete removal of the MACS. 22 They proposed a novel idea that perhaps the ET alone could maintain pressure in the ME without complete MACS. In our study, interoperative obliteration of the mastoid process and the cavity implants with bone powder could reduce the probability of recurrence. 23 This technique could reduce the volume and gas exchange of MACS. 24 Even if the volume of the mastoid air cell is small, it can buffer the pressure. The volume can even be as small as 0.6 mL at an appropriate mucosal surface of the mastoid. 3 Therefore, reducing the volume of the MACS during the operation can enable the ET to better maintain the pressure balance of the ME under the premise that its function is not abnormal. And the development of negative pressure due to gas exchange across the MACS may disappear. However, it can maintain a more stable pressure by breaking the balance between ME gas exchange and mastoid cushioning. 22 Perhaps this is one of the reasons for maintaining stable hearing over time.
All the patients were checked for the mobility of the ossicle chain during the operation, and 54/102 (52.9%) of patients released their ossicle chain. The operation does not require opening the epitympanum, but keeps the “bridge” to the external wall of the epitympanum and the entrance of the tympanum sinus. Hence, this technique not only retains the autologous auditory ossicle chains, but also the external wall of the epitympanum. The natural space of the epitympanum is preserved, which can greatly increase the stability of the ossicular chain. This would avoid the displacement of the implanted auditory ossicle due to various reasons (such as the scar contraction of the fascia during the repair of the tympanic membrane or the strenuous activities of the human body), which will affect the post-operative hearing outcome. 25 In the meanwhile, it would reduce the huge financial burden of titanium ossicle implantation for the patients.
There were 3 (2.9%) patients still had postoperative hearing loss. We believe that this may be due to severe damage to the ME structure of patients. If the ET does not function well, occlusion and adhesion may occur, which can lead to recurrence and hearing loss after the ME is formed. 25,26
This approach also has certain limitations: (1) For non-granulated epitympanum lesions or cholesteatomas that are not limited to the lateral side of the epitympanum, it is difficult to completely remove the lesion tissue. Especially for the cholesteatoma deep in the anterior superior tympanum, it is difficult to remove the entire cholesteatoma on the basis of completely retaining the ossicular chain. Residual cholesteatoma is prone to recurrence, so preoperative imaging evaluation can help us analyze whether IBM could be used. (2) This technique is not recommended for patients with severe horizontal nerve defects, so as not to damage the facial nerve. (3) In order to avoid the damage of the facial nerve in the process of removing the deep granulation deep in the auditory ossicle, the surgeon should have extensive experience in ear microsurgery.
Conclusion
Intact bridge tympanomastoidectomy with preservation of the auditory ossicular chain is an improvement on CWDT. It not only removes the tympanum sinus and epitympanum lesion but also retains the ossicular chain and the lateral wall of the epitympanum, which helps to retain sufficient mobility of the ossicular chain and the ventilation route to the ME. This surgical approach provides significant hearing recovery and long-term hearing stability.
Footnotes
Acknowledgments
We collected the clinical data from the Eye and Ear, Nose and Throat Hospital, Fudan University. We thank for this support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Contributions
Kaishi Wang, MD: data acquisition; Lu Xing: literature research, data interpretation, manuscript preparation, manuscript defnition of intellectual content, and manuscript editing; Gaogan Jia: statistical analysis, literature research, manuscript editing, and manuscript defnition of intellectual content; Hailiang Lin: literature research and manuscript editing; Yusu Ni, MD: guarantor of integrity of entire study, study concepts, study design, manuscript revision/review, and manuscript final version approval.