
Abstract
Background
Congenital pyriform sinus fistula (CPSF) is a rare congenital disease derived from the remnants of the third or fourth branchial cleft.
Objectives
To investigate the imaging characteristics, clinical manifestations, surgical methods, complications, and personalized treatment of CPSF.
Material and Methods
The clinical data of 12 CPSF patients admitted to the Department of Otorhinolaryngology Head and Neck Surgery of the First Affiliated Hospital of Wenzhou Medical University from March 2016 to May 2021 were retrospectively analyzed. Cryogenic plasma radiofrequency ablation, carbon dioxide laser resection, and external cervical excision were selected based on the individual condition, and postoperative complications and efficacy were evaluated.
Results
There were 6 men and 6 women. Neck abscess or thyroiditis was considered at the initial diagnosis. In 11 of the cases, the CPSF was on the left side, whereas in the rest one case, it was on the right. A pyriform fossa fistula was observed during hypopharyngeal iodine angiography. Eight patients were treated with endoscopic piriform fossa fistula laser resection, two with cryogenic plasma radiofrequency ablation, and the rest with external cervical fistula resection. There was no evidence of postoperative hoarseness, pharyngeal fistula, dysphagia, and other complications.
Conclusion and Significance
CPSF is less common in adults than in children. For patients with recurrent neck abscesses, CPSF should be highly suspected, timely angiography should be performed as soon as possible, and care should be taken to avoid missed diagnoses. The primary method for piriform fossa fistula removal is surgical treatment. Finally, tailoring treatment regimens to the patient’s condition can significantly improve curative efficacy.
Introduction
Congenital pyriform sinus fistula (CPSF) is a rare gill-derived disease associated with incomplete obliteration of the third or fourth pharyngeal pouch during early embryonic development. It accounts for approximately 1%–4% of all cervical gill-derived malformations. 1,2 Surgery remains the most effective treatment for the inflammatory lesion. Due to its rarity, misdiagnosis and mistreatment are frequently occurred during clinical scenarios. And consequent abscess incision and drainage can cause scar tissue hyperplasia and damage of normal anatomy of the cervical region.
Patients and Methods
Clinical data of 12 patients diagnosed with CPSF admitted to the Department of Otorhinolaryngology Head and Neck Surgery of the First Affiliated Hospital of Wenzhou Medical University from March 2016 to May 2021 were retrospectively collected. The gold standard for definite diagnosis is the detection of a piriform fossa fistula under a general anesthesia-supported laryngoscope. 3
All patients underwent cervical enhanced CT, B-ultrasonography of the neck, and iodine angiography of the hypopharyngeal esophagus before surgery. We selected the surgical method (cryogenic plasma radiofrequency ablation, carbon dioxide laser resection, external cervical resection) according to clinical manifestations and auxiliary examination characteristics. In addition, we tracked postoperative complications and curative effect. Samples of pus or lesions were collected during surgery for subsequent bacterial measurement. For intraoperative cauterization, we used a CO2 laser system and a laryngeal plasma knife (EIC7070-01 from ArthroCare) with coagulation set to level 5. The depth of burning into the fistula is approximately 1 cm, and the diameter around the fistula opening is approximately 1.0 cm based on the size, shape, and surrounding anatomical structure of the fistula. The fistula and Betz fold structure should be fully exposed in CPSF cases. In addition, cauterization of the Betz fold structure should destroy the fold walls to prevent fluid accumulation intraoperatively. For open surgery, we first performed a laryngoscopic examination, and injected methylene blue into the fistula to provide a positioning reference. We made a standard neck incision along the previous scar, and then separated the mass until exposing its adhesion with the pyriform sinus. We removed and sutured the distal part of the fistula. At the same time, the upper pole of thyroid was separated from the lesion and retained for preventing damages to recurrent laryngeal nerves. Routine antibiotics and nasal feeding were applied for 10 days after operation. To confirm fistula closure, electronic laryngoscopy was performed.
Results
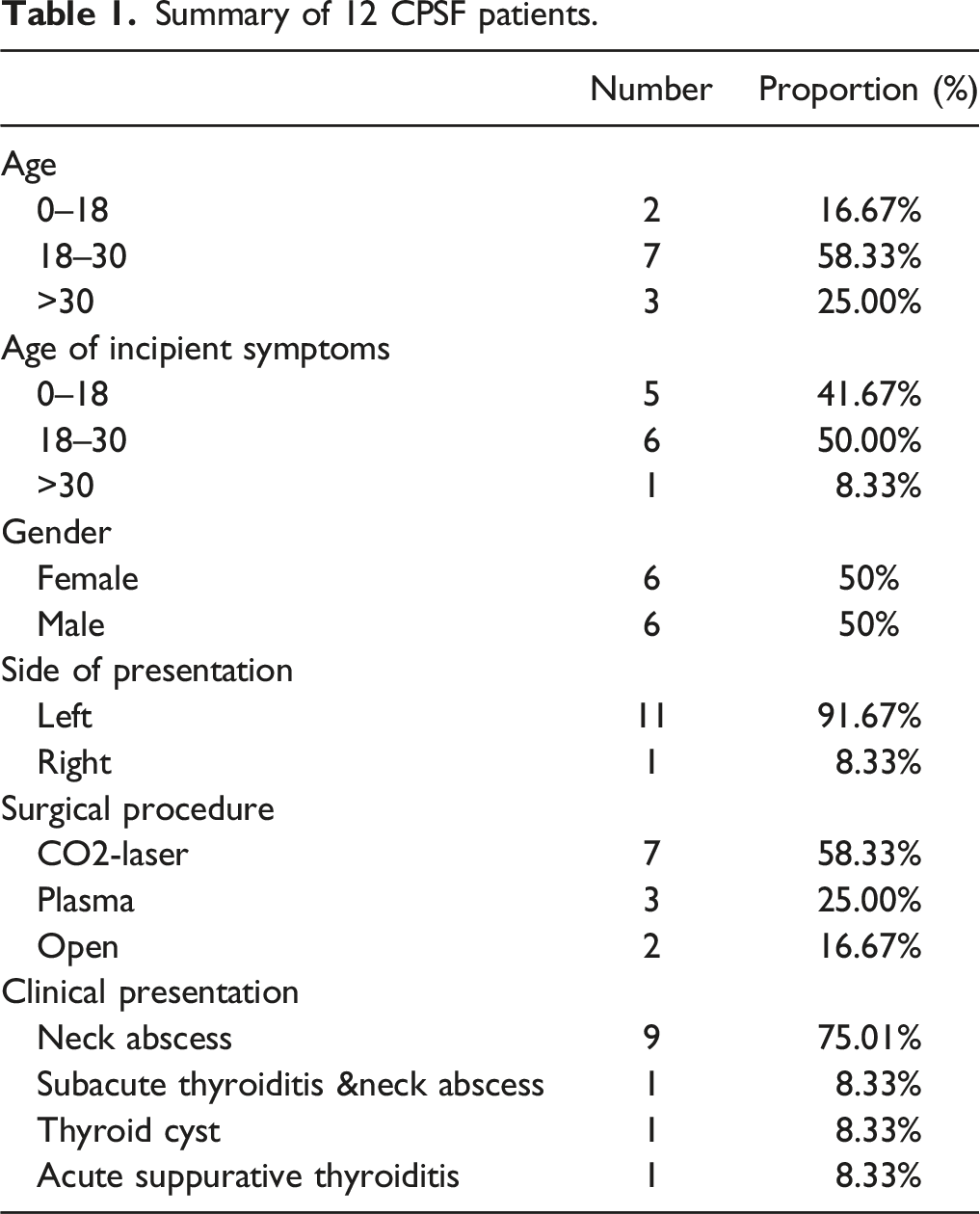
Summary of 12 CPSF patients.
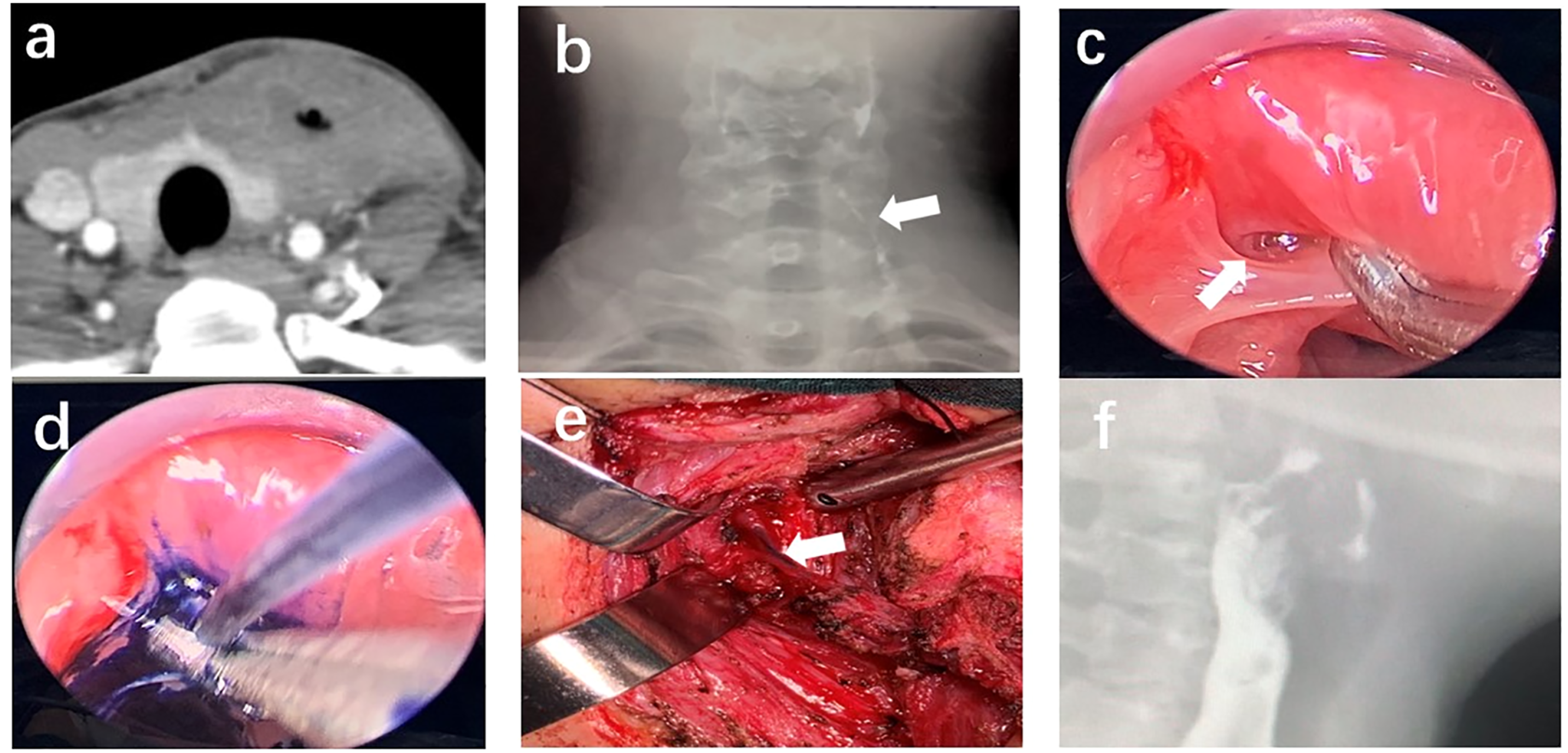
Figures 1 and 2 present two typical examples. (a) November 2017, this improved CT image reveals an abscess in the left neck; (b) the patient was scarred after repeated incision and pus drainage; (c) March 2018, hypopharyngeal iodine angiography (the arrow indicates left piriform fossa fistula); (d) December 2018, endoscopic exploration and CO2 laser fistula resection were performed under general anesthesia (the arrow indicates the fistula at the tip of the piriform fossa, and the five-pointed star indicates the esophageal inlet); and e, (f) 1 month after surgery, hypopharyngeal iodine angiography revealed that the fistula had vanished. (a) CT revealed an abscess in the left neck with air shadow; (b) hypopharyngeal iodine angiography (the arrow indicates left piriform fossa fistula); (c) the arrow indicates a piriform fossa fistula; (d) methylene blue was injected into the internal fistula to reveal the fistula; (e) on surgical exploration (the arrow indicates fistula); and (f) reexamination 1 month later indicated that the fistula had vanished.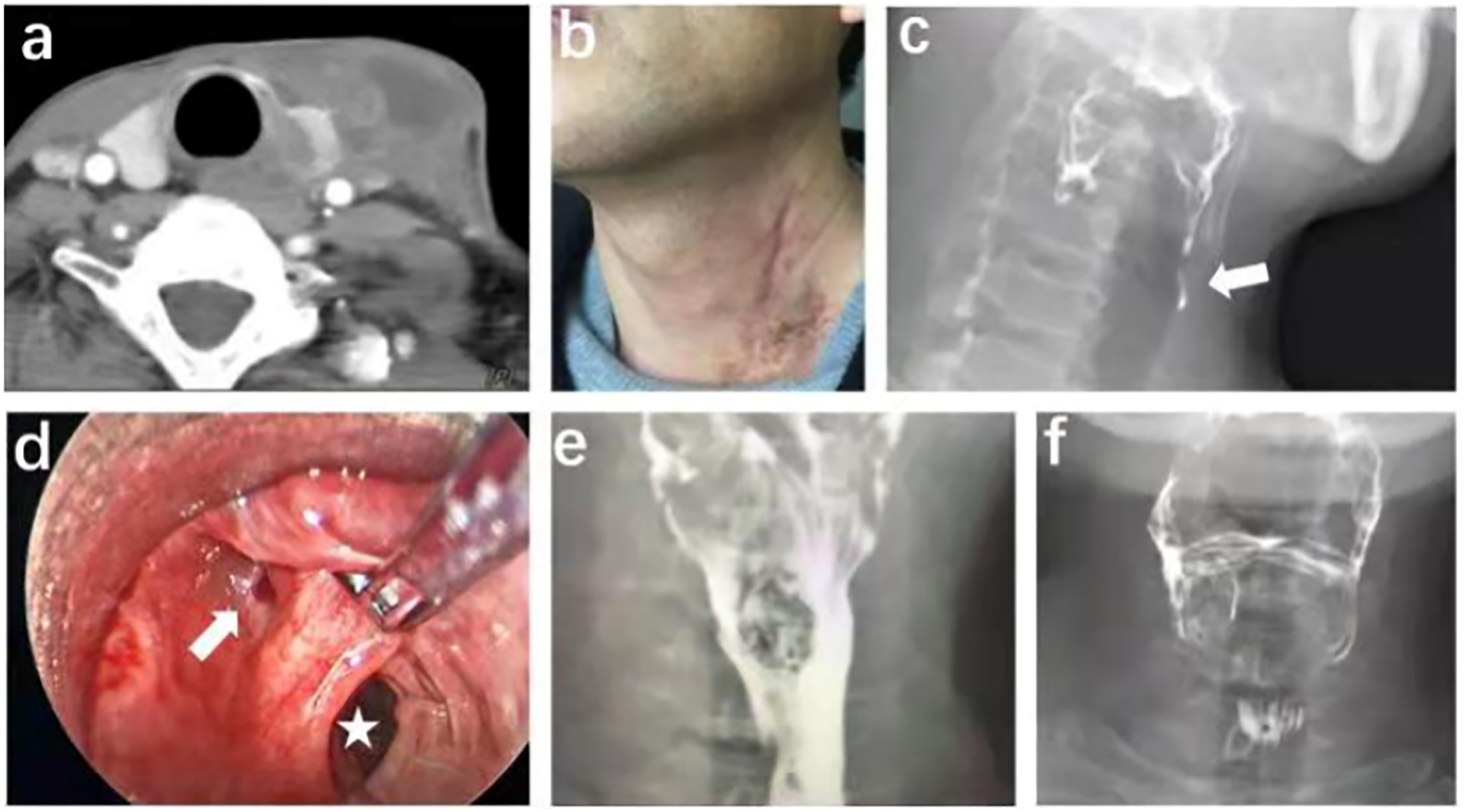
In April 2021, a female patient presented to our hospital with “repeated infection of the left neck for 24 years and recurrence for 4 days.” She had more than 10 times of neck incision and drainage as well as 2 “radical” surgeries in other hospital. After admitting to our hospital, the patient underwent abscess incision and drainage and was given antibiotics after surgery. The contrast agent ran outward and downward from the left piriform fossa apex, with a length of 6 cm, indicating left piriform fossa fistula, according to the hypopharyngeal iodine angiography. Considering the long-distance fistula and the history of multiple operations, open fistulectomy was selected. 2 months after abscess incision, the patient underwent resection of the left piriform fossa fistula under general anesthesia. During the operation, we detected the fistula endoscopically, and injected methylene blue into the fistula to provide a positioning reference for open surgery. Then we perform fistula resection through cervical anterior approach with the assistance of a neural monitor to avoid recurrent laryngeal nerve injury. The fistula was confirmed to be eliminated by hypopharyngeal iodine angiography 1 month after the operation, and neither neck swelling nor pain was reappeared. The follow-up is still ongoing.
Discussion
Congenital piriform sinus fistula (CPSF) was first reported by Raven in 1932. 5 It begins in the piriform fossa and travels through the cricothyroid muscle and the hypopharyngeal constrictor before arriving at the thyroid. Left fistulas are more common than right ones, which could be due to embryogenesis inhibition of the right superbranchial cleft and asymmetric transition of the fourth branchial arch, 6,7 and the data in our study were consistent with this view. Colonization of bacteria and food debris in the mouth and throat are main source of infection for CPSF infection and even abscess-formation, which migrate along the fistula to the deep tissue through the piriform fossa fistula. In majority of the patients, CPSF occurred in their infancy or childhood, and the majority of neonates sought medical attention due to the discovery of a mass in the anterior cervical region. There are many empirical studies or large-scale reports on CPSF in infants and young children; however, CPSF in adult is relatively uncommon, making it prone to be misdiagnosed in adult patients presenting with neck abscess onset.
The clinical symptoms and imaging manifestations of CPSF in adults differ from those in children or neonates. Piriform sinus fistulas in children are usually manifested as neck abscess or acute thyroiditis. The subjects in the current study were mostly hospitalized due to recurrent neck mass with or without abscess, rupture, tenderness, fever, or thyroiditis, and 66.67% of the patients had a history of neck incision and drainage prior to admission, including one patient with up to 10 times of neck incision drainage. CPSF should be considered when recurrent neck abscess or acute suppurative thyroiditis occurs, particularly in the left neck. CPSF can be classified into 3 types based on clinical manifestations, intraoperative findings, and presence of internal and external fistulas: the sinus type (with internal or external fistulas), the fistula type (with internal and external fistulas), and the cyst type (without internal or external fistulas). The sinus tract type is the most common.
To confirm the diagnosis, all patients underwent preoperative neck ultrasound, electronic laryngoscopy, enhanced CT, and hypopharyngeal iodine angiography. Iodine angiography of the hypopharyngeal esophagus reveals the morphological changes of piriform fossa, such as sinus and fistula formation, which can be used as an ideal method for diagnosing CPSF in static inflammatory phase. 8 In this study, the positive rate was 83.33% in the 12 cases. However, when the mucosa of the piriform fossa fistula swells and obstructs the fistula during the acute inflammation stage, the contrast agent is unable to enter the fistula; thus, negative results can be obtained. 9 In our study, the B-ultrasonic results indicated an inflammatory mass in the neck tissue and hypoechoic thyroid nodules. According to Li’s study, patients of different ages have different cyst boundaries. More specifically, the cyst walls become thicker and the cyst boundary become more blurred with age. 10 Repeated inflammation will cause adhesion with the surrounding tissue structure, and the opening of the piriform sinus to the fistula will gradually lead to inflammatory stenosis; the stenosis and closure of the adult sinus may be undetectable by B-scan ultrasonography. Enhanced CT of the neck revealed local soft tissue on the surface or uneven low-density area inside the sternocleidomastoid muscle; there is also usually no airway compression. Goiter can be shown, or uneven local or large range of mass, visible round, punctured, strip, and other multiple gas shadows, the piriform fossa narrows down or disappears. CT also reveals the approximate location of the lesion and its relationship with the surrounding anatomical structure. The most representative characteristic is the presence of an air bubble within the mass or fistula. 11 In this study, MR examinations were not conducted; some researchers claimed that MR examinations do not detect the presence of microscopic bubbles in the cyst. 4
Traditional open-neck surgery and minimally invasive surgery via supported laryngoscopy, to seal the inner orifice, are the only effective methods for radical treatment. The two surgical methods have both advantages and disadvantages. Compared with traditional open surgery, endoscopic surgery shows simple operated, fewer complications, shorter hospital stay, repeatable operation, and easy to be accepted by patients. Minimally invasive surgery included mucosa cauterization and cryogenic plasma radiofrequency ablation. Compared with CO2 laser, low-temperature plasma has less thermal damage to tissue and can reduce nerve damage to a greater extent. The basic idea is to cauterize or excise the piriform fossa internal fistula, as well as its periphery and fistula mucosa, thus the mucosa can be closed by scar adhesion after edema, avoiding subsequent infection. Nevertheless, these endoscopic methods are imperfect so far, as the recurrent rates are higher than that of the complete resection approach. 12
It is important to note that during the acute or subacute stages of CPSF, cryogenic plasma cauterization with a support laryngoscope is not recommended. Endoscopy is ineffective at this stage for determining the internal opening of the CPSF. It has been reported that the one-time closure rate of endoscopic cautery is 55.9%–98.1%. 13,14 On the contrary, studies have reported that the one-time closure rate of endoscopic cautery is 82.5%. Re-cauterization is performed for the patient who has not closed. The cumulative closure rate of secondary cautery was 95.0%, whereas that of tertiary cautery was 100.0%. In total, the average number of cauterizations was 1.2 times. 14
Complications following endoscopic cauterization may include secondary deep neck infection, oropharyngeal mucosal abrasion, obvious dysphagia, hoarseness and cough, and arytenoid joint dislocation. 15 Complications from open surgery may include vocal cord paralysis, wound infection, neck scar, and nerve damage. This group of patients in the current study showed no postoperative complications.
Based on the advantages and disadvantages of different surgical methods, we summarize the following points on how to make selections between the two surgical methods: For patients who are with the first-episode, and with no prior incision and drainage history, the minimally invasive surgical method should be preferred. Open surgery is a viable option for those patients who have previously failed minimally invasive fistula resection and a long fistula distance. Attention should be paid to fistula location and details such as avoiding recurrent laryngeal nerve injury. When there is a high risk of injury to the recurrent laryngeal nerve due to structural changes in the neck caused by scar hyperplasia, patients who have had multiple open surgeries can try endoscopic surgery. Herein, individualized treatment according to the patient’s condition can significantly improve the efficacy and safety.
This study has some limitations. First, the sample size was relatively small due to the low morbidity. Second, the differences between plasma and CO2 lasers in minimally invasive surgical modalities were not elucidated. Last, long-term outcome of the two surgical methods have not been studied.
Conclusion
Piriform fossa fistula is easily misdiagnosed in adults, and it usually presents as neck abscess or neck mass during the patients’ initial visit. It should be considered in patients with recurring episodes of neck abscess. To date, antibiotic and anti-infection plus surgical treatment is the universally accepted treatment principle of piriform fossa fistula. Endoscopic laser ablation and cryogenic plasma radiofrequency ablation have the advantages of minimally invasive, effective, and high safety, providing a new surgical method for piriform fossa fistula. However, traditional open surgery may be a rational choice for patients who experience recurrence of residual sinus tract infection.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All procedures performed in studies involving human participants were in accordance with the ethical standards of the ethics committee of The First Affiliated Hospital of Wenzhou Medical University.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We received financial support from the Natural Science Foundation of Zhejiang Province, China (No. LY19H130001).