
Abstract
Objective
This study aimed to examine the olfactory and gustatory dysfunctions (OGDs) among hospitalized patients with a novel strain of severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2), lineage B.1.617.2, also known as the delta variant, in Xi’an, China through verbal interviews.
Methods
Clinical information of 370 hospitalized patients infected with the delta variant in the Aerospace City Branch of Xi'an People's Hospital in Xi’an, China from December 27, 2021 to January 10, 2022 were collected. The prevalence and characteristics of OGDs were collected using a simple questionnaire submitted to all infected patients, including questions about the presence and absence of OGDs.
Results
Among the 370 patients infected with the delta variant, 28 (7.6%) reported OGDs. A significant proportion of patients with self-reported OGDs were younger than those without (28.9 ± 10.5 vs. 35.3 ± 13.9, P = 0.005) and had significantly higher rates of sore throat and rhinitis (28.6% vs. 12.3%, P = 0.033; 42.9% vs. 9.9%, P = 0.000). Women were significantly more affected by OGDs than men (67.9% vs. 32.1%, P = 0.012). Vaccinated and unvaccinated delta variant-infected patients showed statistically significant differences in terms of disease severity (P = 0.002).
Conclusions
The prevalence of OGDs in the delta variant infection was lower than that in wild-type SARS-CoV-2 infection. Meanwhile, young age, female sex, and upper respiratory tract symptoms could be closely related to the occurrence of OGDs in the delta variant infection. In addition, a satisfactory level of efficacy was obtained with coronavirus disease 2019 vaccines against moderate and severe delta variant infections.
Introduction
Coronavirus disease 2019 (COVID-19) is caused by severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) and is highly contagious and widespread. 1 After the wild-type strain, the SARS-CoV-2 virus circulates in several variant strains worldwide that have also seriously affected the socioeconomic development globally. The delta variant is a highly adaptable strain that has gradually become the dominant epidemic strain worldwide since it was first reported in India in June 2020. With the further development of related research, the mystery of the delta variant has gradually been unveiled. To date, many studies have shown that the delta variant strain replicates faster, is more contagious, has shorter incubation periods, and nucleic acid testing takes a longer time to turn negative.2-4
Most studies5,6 in the United States and Europe have shown that the loss of taste or smell tends to be a common symptom for those infected with the wild-type strain of SARS-CoV-2, and the symptoms were reported more frequently in mild cases. Furthermore, the olfactory and gustatory dysfunctions (OGDs), the ‘classic’ symptoms, could trigger community nucleic acid testing in many European countries. However, few studies in China have focused on OGDs in patients with COVID-19. 7 To our knowledge, only two researches8,9 have described the prevalence of OGDs in hospitalized patients with COVID-19, and the prevalence is lower than those conducted in Europe and the United States. Although the delta variant has long been the dominant strain in many countries, there is very little research on OGDs in patients with the delta variant. Moreover, there has been little research on the delta variant in China. At present, studies show that OGDs in patients infected by the delta variant might be due to the following reasons. First, the delta variant appeared late in mainland China, was mostly distributed in individual cases, and was quickly controlled. Second, smell or taste disorders have not been a very concerning symptom for the general public and even for some medical staff, resulting in the omission of OGDs on medical records.
According to clinical studies, post-viral olfactory dysfunction is a common cause of smell disorders in adults The exact mechanisms of OGDs in patients with COVID-19 remain unclear. However, several studies10-12 have shown that angiotensin converting enzyme 2 (ACE2) receptors that bind to SARS-CoV-2 are highly expressed in nasal and oral mucosal epithelial cells and in the nervous system, which can be regarded as a potential mechanism for olfactory disorders. Exploring the clinical characteristics of different VOC strains will help understand the underlying mechanisms.
This study aimed to investigate olfactory and gustatory dysfunction in hospitalized patients infected with the delta variant in China.
Patients and methods
Data collection
This retrospective observational study enrolled 370 patients infected with the delta variant at the Aerospace City Branch of Xi'an People's Hospital in Xi’an City, Shaanxi Province, from December 27, 2021 to January 10, 2022. Medical staff who were well trained in this hospital collected nasopharyngeal swabs according to standardized procedures. Following the manufacturer’s instructions, we extracted viral RNA using the nucleic acid isolation kit (Sansure Biotech Inc. Lot No.2020007, China) for 2 h. RT-PCR was performed using a SARS-CoV-2 RNA detection kit (Sansure Biotech Inc. Lot No.2020007, China).13,14 A positive reference gene and the N and ORF1a/b genes were targeted by primers and probes during RT-PCR. A strict set of biosafety protocols and standard operating procedures was followed during all tests. The following patients were excluded from the study: those with a history of cognitive impairment, and those with other causes of OGDs, such as traumatic brain injury and chronic rhinosinusitis, before the epidemic.
Demographic data, including sex, age, general symptoms (fever, cough, dyspnea, fatigue, sore throat, rhinitis, abdominal symptoms, headache, and myalgia), computed tomography (CT) scans, and information about OGDs and vaccination were collected. Due to the need to avoid cross-infection during the outbreak, most records were subjective symptoms and the examinations that were available. The diagnosis, severity, and classification of the disease were based on guidelines published by the Chinese National Health Commission 15 and WHO. 16 This study was approved by the Ethics Committee of the First Affiliated Hospital of the Air Force Medical University (XJLL-KY20212083). All patients signed an informed consent form.
Statistical analysis
All statistical analyses were conducted using the IBM SPSS Statistics software (version 26.0; IBM Corporation, Armonk, NY, USA). The baseline data were calculated as arithmetic means with standard deviations (SDs) based on a normally distributed distribution. Proportions of categorical variables, which were expressed as counts and percentages, were compared using the Chi-squared test. An independent samples t-test was used to determine whether the differences between the data were statistically significant. Statistical significance was set at P < 0.05.
Results
Demographic and clinical features
Demographic and clinical features of patients with Delta COVID-19.
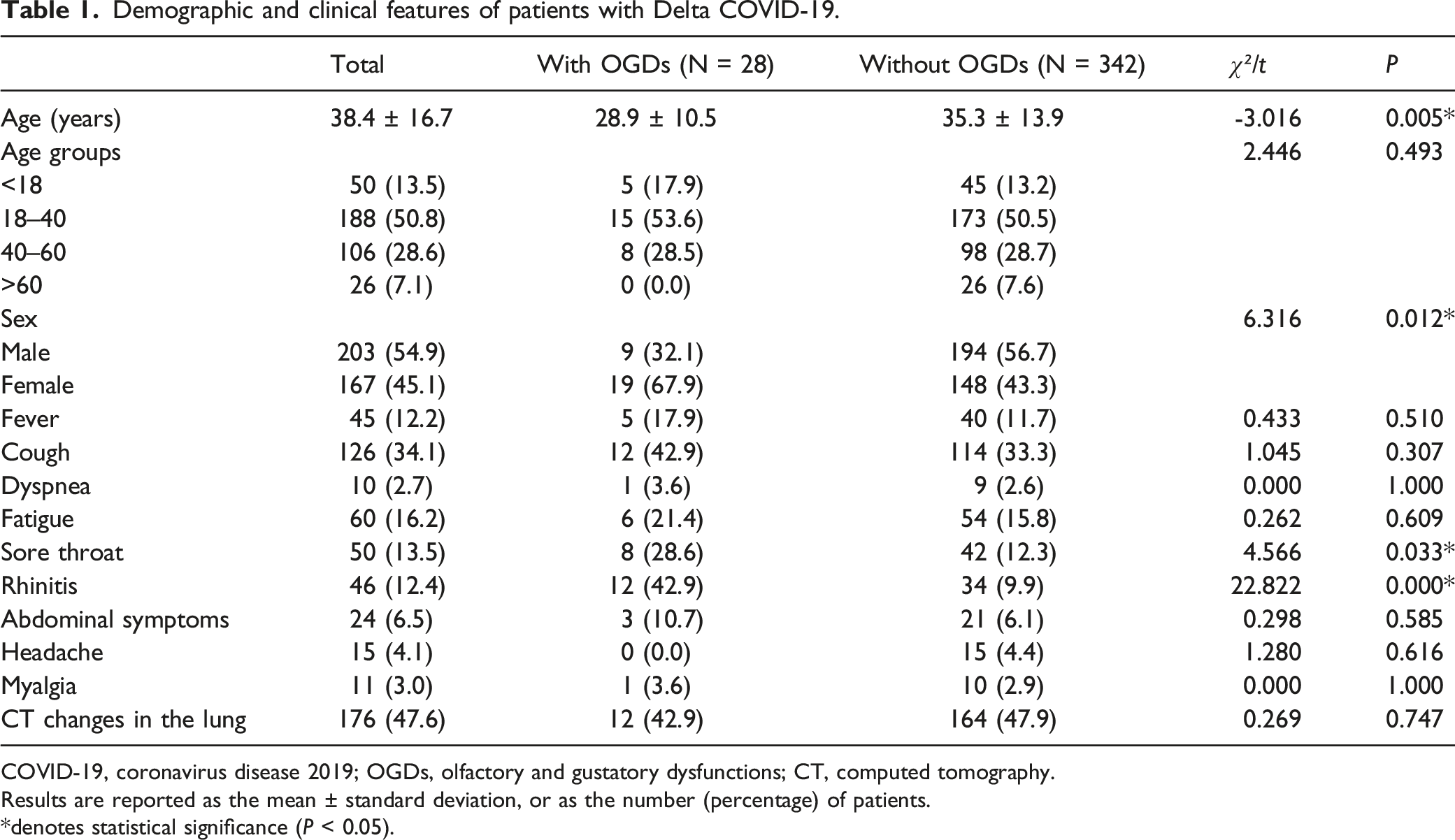
COVID-19, coronavirus disease 2019; OGDs, olfactory and gustatory dysfunctions; CT, computed tomography.
Results are reported as the mean ± standard deviation, or as the number (percentage) of patients.
*denotes statistical significance (P < 0.05).
Prevalence of Olfactory and Gustatory Dysfunctions in Hospitalized Patients Infected with the Delta Variant
Of the 370 patients, 28 (7.6%) reported at least one OGD. Among them, nine (32.1%) reported only smell disorders, seven (25.0%) reported only taste disorders, and 12 (42.9%) reported both smell and taste problems (Figure 1). An altered sense of smell or taste was reported as the only symptom in six (1.6%) patients. All patients with OGDs received at least one dose of the COVID-19 vaccine. Proportion of olfactory dysfunction (OD) and gustatory dysfunction (GD) in patients with Delta COVID-19.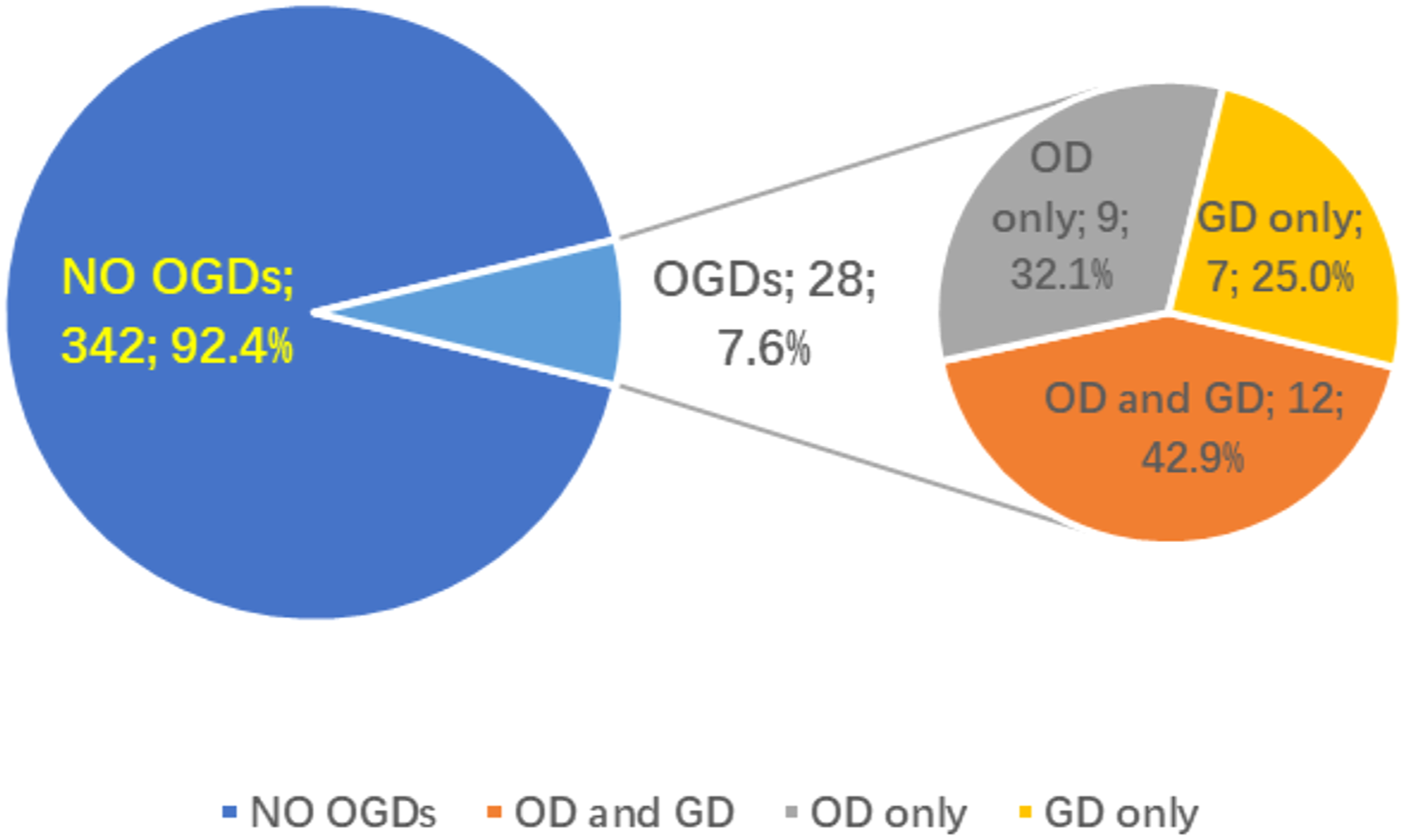
The most common symptoms in patients who reported OGDs were cough (42.9%) and rhinitis (42.9%), whereas the rarest symptoms were headache (0.0%), dyspnea (3.6%), and myalgia (3.6%). Moreover, the most common age group among these patients was the young age group (18-40 years) (53.6%) (Table 1).
Severity of SARS-CoV-2 Delta Variant Infection among Infected Patients Who Have Been Vaccinated and Unvaccinated
Severity of vaccinated or unvaccinated patients.

Results are reported as the number (percentage) of patients.
Discussion
Main results of this study
To the best of our knowledge, this is the first study in China to describe the prevalence and characteristics of olfactory and gustatory dysfunctions (OGDs) in hospitalized patients infected with the delta variant. Previous global studies have shown that patients with COVID-19 may have a loss of taste or smell as a common symptom. 17 The COVID-19 protocols in many countries have considered OGD as a typical symptom and key point of differential diagnoses. Viruses are constantly changing, and new variants appear over time; these new variants can even reinfect humans. Researchers have been working on the study of the COVID-19 variant strains. However, it is still unclear what the epidemiological characteristics and mechanisms of OGDs are. A relatively small number of relevant reports have been published, particularly in China. This study utilized a self-reported questionnaire to assess subjective olfactory and gustatory perception among hospitalized patients infected with the delta variant. Furthermore, electronic medical records were used to analyze the relationship between other manifestations of delta variant and OGDs.
In this study, 7.6% of patients infected with the delta variant complained of the smell or taste disturbances, and 5.7% reported olfactory disorders. The self-reported prevalence of OGDs in this study was significantly lower than the 18.4% reported by a Korean study on the delta variant 18 and was also significantly lower than the 53% pooled prevalence found in a large sample size meta-analysis of the wild-type strain of COVID-19 using a random-effects model. 19
The World Health Organization (WHO) identified five variants of concern as Alpha, Beta, Gamma, and Delta, with the latest being the Omicron variant. A survey that summarized several reports in Europe and the United States showed that the rates of self-reported OGDs in patients infected with the wild-type strain of SARS-CoV-2 ranged from 34% to 68%, 6 while a multicenter European study 20 reported that the rate was as high as 79.7%. Two studies8,9 on hospitalized patients with COVID-19 in China showed that the incidence rates of self-reported smell impairment were 15.3% and 5.1%, respectively. The discrepancies in the incidence of OGDs may be due to the different emphasis placed on the ears, nose, and throat symptoms by healthcare providers and researchers across countries. On the one hand, previous studies showed that the frequency of OGDs in COVID-19 differed between detection via validated smell tests and questionnaire reports, and when objective measurements were compared to self-reports, olfactory dysfunction was more prevalent.21,22 Therefore, self-reported studies may have underestimated the prevalence of olfactory disorders associated with COVID-19. Our study used a questionnaire to assess the sense of taste and smell, and the different assessments resulted in some of the variations between this study and other prevalence studies of OGDs in COVID-19. On the other hand, a study from Germany showed that the rate of OGDs in children infected with the Alpha VOC, which was also one of the main spreading variant strains, was 1.7%. 23 Moreover, the rate in adults was also very low, which was reported by the Coronavirus (COVID-19) Infection Survey of the UK Office for National Statistics. A South Korean study 24 of 40 patients with the Omicron VOC found that only one (2.5%) patient had a loss of smell or taste, and a recent study published in The Lancet showed that the loss of smell was less common in participants infected during the Omicron prevalence than that during the Delta prevalence. 25 Bartheld et al further found that mutations of SARS-CoV-2 might be a major contributor to the prevalence of chemosensory deficits. 26 Similar to previous studies, our study's low incidence of olfactory disorders may be due to the fact that all patients were infected with the delta variant strain.
This study also explored the variations in clinical characteristics between patients with and without self-reported symptoms of smell or taste disorders. The younger the patient, the more susceptible a person was to olfactory and gustatory dysfunction. However, previous studies showed the age difference was not statistically significant. 27 The present study showed that 67.9% of patients suffering from chemosensory disorders were females, and the difference in gender between the two groups was statistically significant. A study from Italy 28 pointed out that men were more susceptible to developing chemosensory disorders than women. This discrepancy may be due to the different strains; therefore, age and sex differences among the delta variant-infected patients with OGDs require further study.
We also found that patients infected with the delta variant with OGDs were more likely to have symptoms of sore throat and rhinitis, which was statistically significant. Unlike the present study, a retrospective telephone survey found that only a few patients with smell or taste impairment infected with the original strain reported rhinitis, 29 and Lechien et al demonstrated that there was no significant connection between olfactory dysfunction and rhinitis symptoms in a statistical analysis of 417 patients with COVID-19. In addition, widely expressed ACE2 receptors on oral and nasal mucosal epithelial cells and even the nervous system may be the underlying mechanisms that lead to OGDs,10-12 while OGDs may also be the result of nasal inflammation or obstruction. Although the results of the study are preliminary, we can conclude that the cause of chemosensory impairment in patients infected with the delta variant was more frequent in patients with upper respiratory tract symptoms.
This study compared the severity of infection between vaccinated and unvaccinated patients, and the results indicated that moderate infection rates were lower in the vaccinated group than in the unvaccinated group, which is similar to some previous studies, which showed that moderate and severe infections caused by the delta variant could be prevented by the vaccine.30,31 Even if the sample size was small, it is still possible to conclude that, despite the fact that vaccination does not completely protect against infection by the delta variant, protection against moderate and severe infections remains effective.
Limitations
This study has some limitation. First, the sample size was small, which could have caused bias in clinical observations. It would be better to include more patients infected with the delta variant from Xi’an and other cities worldwide. Second, all data were collected from electronic medical records, and taking into consideration the risk of cross-infection, it was decided to use a very simple questionnaire to assess the sense of smell and taste, and some accurate information, such as the severity and development course of chemosensory disorders, may be missed, Objective assessments should be included in future studies. Finally, the detailed vaccination status of the patients was incomplete, which could also have caused bias.
Conclusions
The prevalence of OGDs with the delta variant infection was lower than that of the wild-type strain. In addition, young age, the female sex, and upper respiratory tract symptoms might be closely related to the occurrence of OGDs in delta variant infections. Vaccine efficacy against moderate and severe delta variant infections was satisfactory in patients with COVID-19. However, further studies are needed to validate these results.
Footnotes
Acknowledgements
We would like to thank the Nursing Department of Xi’an People’s Hospital for their help with data collection.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Shaanxi Provincial Department of Science and Technology Key Industry Innovation Chain (Group) Social Development Field (2021ZDLSF02-12).