
Abstract
Peutz-Jeghers syndrome is an unusual inherited intestinal polyposis syndrome associated with distinct mucocutaneous pigmentation. Peutz-Jeghers syndrome is known to show variable penetrance and clinical heterogeneity. It can involve various organs and lead to intestinal and extra-intestinal malignancies. Sinonasal inverted papilloma is a benign tumor originating from the nasal cavity and paranasal sinuses. It is characterized by high recurrence and malignant transformation; however, the exact pathogenesis and risk factors remain unclear. Recently, we encountered a case of sinonasal inverted papilloma in a patient with Peutz-Jeghers syndrome. Although we performed a molecular genetic study to evaluate the STK11/LKB1 mutation, we could not provide direct evidence of the association between sinonasal inverted papilloma and Peutz-Jeghers syndrome. Based on our experience, we here tried to introduce Peutz-Jeghers syndrome and the potential involvement of the upper airway tract based on previously reported cases.
Introduction
Peutz-Jeghers syndrome (PJS) is an autosomal dominant condition with variable penetrance characterized by gastrointestinal hamartomatous polyposis and mucosal pigmentation. As it is known to be associated with germline mutations of several candidate genes, such as the STK11/LKB1 tumor suppressor gene, extra-intestinal organs such as the breast, uterus, and endometrium could also be involved. 1 Patients with PJS have an increased risk of developing gastrointestinal and extra-intestinal cancer at a relatively young age. 2 Only a limited number of cases of nasal polyps affecting the upper airway in PJS have previously been reported. For example, three cases of sinonasal polyposis in a PJS family have been reported, and two of these developed sinonasal-type adenocarcinomas during follow-up. 3
Sinonasal inverted papilloma is a benign epithelial tumor that occurs in the nasal cavity or paranasal sinuses and is characterized by inverted squamous epithelial growth in the underlying connective tissue stroma with an intact basement membrane. 4 It accounts for 0.5-4.0% of all nasal tumors and can cause significant health concerns due to its high recurrence, focal aggressive growth, and the possibility to transform into malignancy. 4 Compared to nasal polyps, no case of sinonasal inverted papilloma in PJS has been reported until now. In other organs, a variety of papillomas have been reported in PJS. For example, intraductal breast papilloma with squamous metaplasia and oral papillomas combined with nasal polyposis have also been reported in PJS.5,6
Recently, we encountered a case of sinonasal inverted papilloma in a patient who was previously diagnosed with PJS. To the best of our knowledge, this is the first report of such a case. By sharing our experience, we are making an effort to introduce PJS and its implications for ear nose throat (ENT) and internal medicine clinicians.
Case presentation
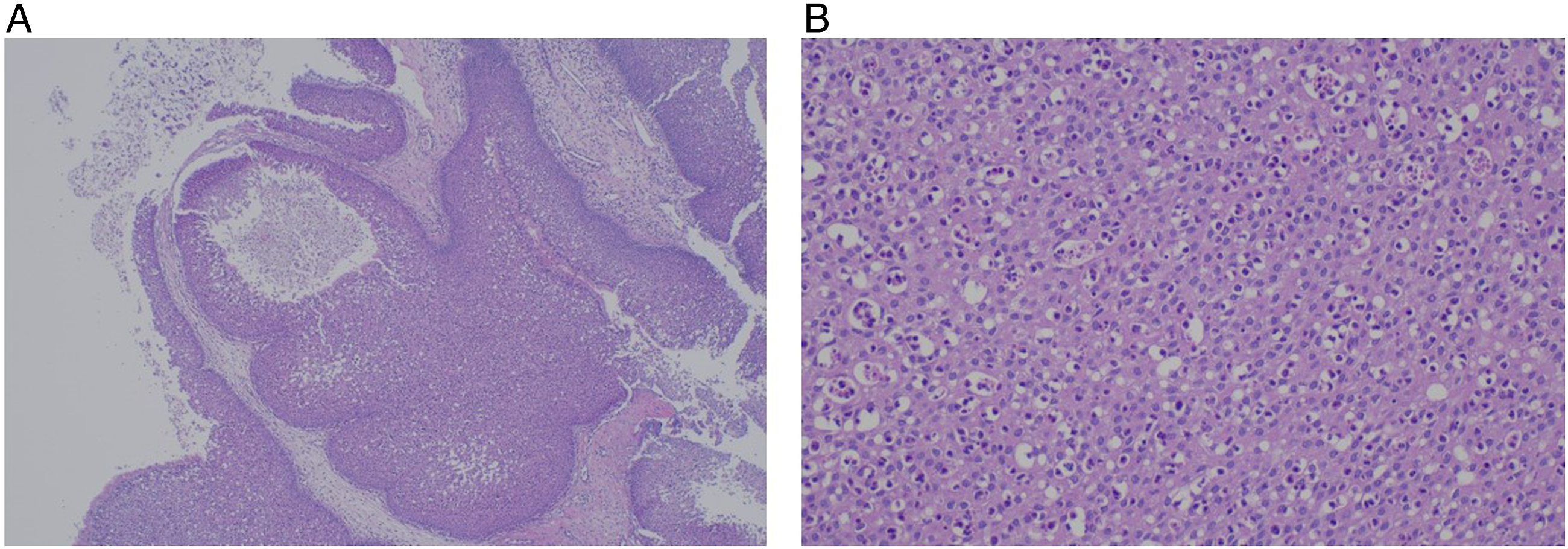
A 39-year-old man presented to the otorhinolaryngology department with a history of recurrent epistaxis. He had previously been diagnosed with PJS. He had a history of intermittent rectal bleeding, underwent colonoscopy by an internal medicine specialist, and was pathologically diagnosed with PJS several years before visiting our hospital. He also had a previous history of fingertip pigmentation. The rest of his medical history was unremarkable. Nasal endoscopic examination revealed a mass-like lesion protruding between the lateral nasal wall and middle turbinate, and a bleeding focus was observed in the inferior border of the mass-like lesion (Figure 1A). Paranasal sinus computed tomography (PNS CT) demonstrated a heterogeneous, subtle, enhancing mass in the right maxillary sinus, causing widening of the infundibulum (Figure 1B). Paranasal sinus magnetic resonance imaging (PNS MRI) showed a lobulated cribriform pattern mass that was isointense in T2 (Figure 1C). Based on the images, the mass was suspected to be a sinonasal inverted papilloma, and transnasal endoscopic sinus surgery was planned. During surgery, it was found that the tumor was attached to the posterolateral wall of the maxillary sinus. The mass, including the attached area, was removed and sent to the pathology department for analysis. Postoperative histopathological examination revealed an inverted papilloma (Figure 2). As he was previously diagnosed with PJS in another hospital, we performed a molecular study of the STK11 gene variant by sequencing the entire coding exon (a total of 9 exons) and near introns. However, no pathogenic variant of STK11 was found. Six months after surgery, the patient had no sign of recurrence. Endoscopic and imaging findings of sinonasal inverted papilloma in this case. (A) Nasal endoscopy showing a mass-like lesion that protruded between the lateral nasal wall and middle turbinate. (B) Coronal CT showing a heterogeneous subtle enhancing mass in the right maxillary sinus causing widening of the infundibulum. (C) Coronal MRI showing a lobulating cribriform-pattern mass. CT, computed tomography; MRI, magnetic resonance imagining. Histopathologic evaluation of sinonasal inverted papilloma in this case. Hematoxylin-eosin staining showing thickened squamous epithelium with an inverted growth pattern (A, magnification, X40). There was no significant cytologic atypia (B, magnification, X100).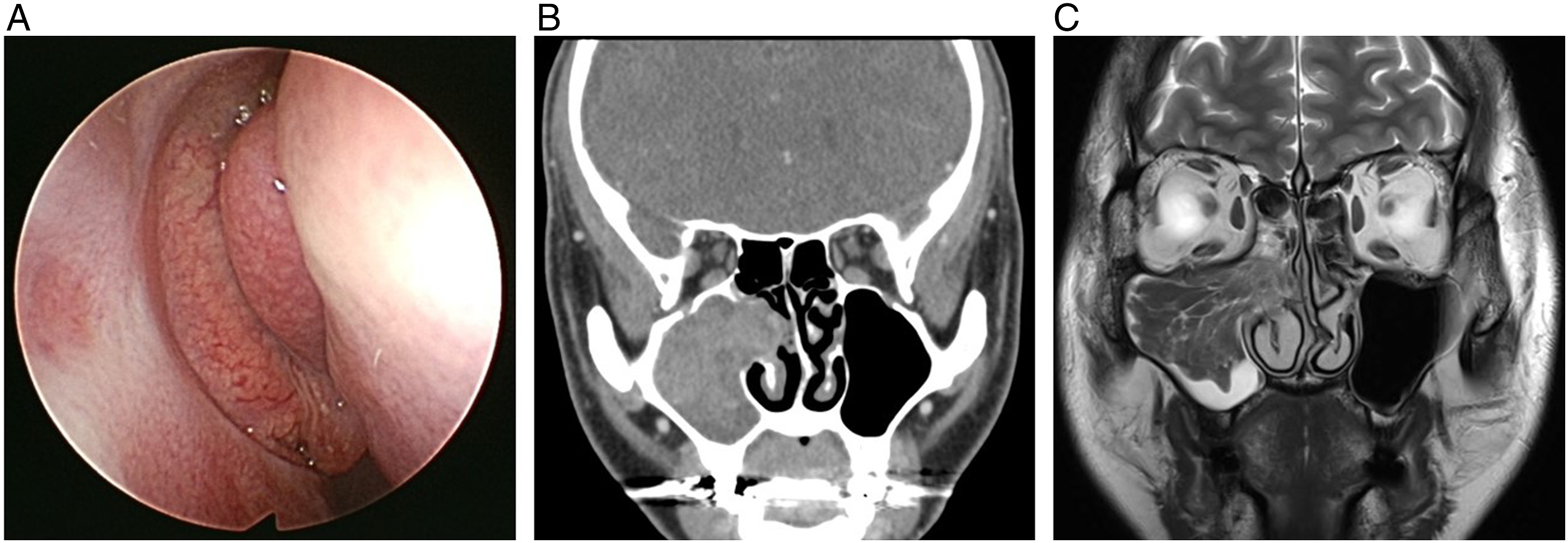
Discussion
PJS is a clinical diagnosis that may be supported by genetic testing. For individuals with a histopathologically confirmed hamartoma, a definite diagnosis of PJS requires at least two of the following three clinical findings: A family history consistent with autosomal dominant inheritance, mucocutaneous hyperpigmentation, or small-bowel polyposis. 7 Our patient was previously diagnosed with hamartoma in the gastrointestinal tract and had a history of hyperpigmentation of the fingertips that faded away after puberty. Based on these findings, the patient was clinically diagnosed with PJS.
Molecular testing also established a diagnosis of PJS. Molecular testing approaches include single-gene testing, the use of a multigene panel, and more comprehensive genomic testing. 8 Single-gene testing involves a sequence analysis of STK11/LKB1 (serine/threonine kinase 11), a tumor suppressor gene on chromosome 1p13.3. 9 A multigene panel includes STK11 and other genes of interest, and more comprehensive genomic testing includes exome sequencing and genome sequencing. 8
In our case, a single-gene test of STK11/LKB1 was performed; however, we could not demonstrate a direct association between sinonasal inverted papilloma and PJS. As this was the first case of a molecular genetic study of PJS in our institute, we could not extend our evaluation to further comprehensive molecular studies covering potential candidate genes.
The molecular genetic association between nasal inverted papilloma and PJS needs to be evaluated to show the clinical implications of inverted papilloma in PJS. In nasal polyps, a deleterious mutation of the STK11/LKB1 locus has been shown in sinonasal samples and blood samples at the same time in the same patient, suggesting a causal relationship between sinonasal polyp development and PJS. 3 Furthermore, it has been suggested that some parts of sinonasal polyps that are associated with PJS show malignant transformation. This is an important point because although the carcinogenesis in sinonasal polyposis remains unclear, it might be understood in the context of STK11/LKB1 mutation. 3 Furthermore, clinical differences between sporadic sinonasal polyps and PJS-related polyps have suggested that PJS-related polyps have fewer eosinophils than sporadic polyps. 2
However, a sinonasal inverted papilloma has never been reported in PJS so far, and no studies on PJS-associated sinonasal inverted papilloma have been published yet. It has been reported that 5-15% of sinonasal inverted papillomas could progress to malignancy throughout the course of the disease; however, the mechanism and etiology of malignant transformation in sinonasal inverted papilloma remains unclear. 4 Although we tried to evaluate the molecular genetic association of sinonasal inverted papilloma and PJS, we did not find any mutation in the STK11/LKB1 gene in our patient. However, studies on STK11/LKB1 gene mutations in PJS show heterogeneous results. 10 The STK11/LKB1 mutation was detected in all PJS patients in one study, while in other studies, STK11/LKB1 mutations were not found in 33-42% of patients with clinical characteristics of PJS 10 and germline mutations of the STK11 gene have been detected in only 70% of patients with familial PJS. 3 Therefore, our result does not rule out an association between sinonasal inverted papilloma and PJS, especially as our evaluation could not detect any massive deletion or duplication of the STK11/LKB1 gene, and other potential genes 10 were not evaluated. If the association of sinonasal inverted papilloma with PJS could be investigated through molecular genetic evaluation, it would be very helpful in understanding the pathogenesis of malignant transformation of inverted papillomas.
PJS itself is a very rare disease entity, and many ENT doctors might not be aware of it and may not recognize its systemic involvement. Based on this case, we suggest that ENT clinicians should perceive PJS as a systemic disease that could affect the upper airway tract and remember that sinonasal inverted papillomas could be a part of PJS and should perform thorough investigations whenever PJS is suspected.
Footnotes
Data availability statements
The datasets generated during and/or analyzed during the current study are not publicly available due to the patient’s privacy, but are available from the corresponding author on reasonable request.
Ethical/consent statement
Written informed consent was obtained from the patient.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.