
Abstract
Objectives
This study was conducted to identify the risk factors for free flap outcomes in head and neck reconstruction.
Methods
A retrospective review of 318 free flaps were used for head and neck reconstructions in 317 patients over seven years. The patient characteristics, surgical data, and flap outcomes were recorded. The impact of risk factors related on the outcomes of free flaps were analyzed using single and multivariate analysis.
Results
For single factor analysis, 295 free flaps for the first reconstruction were included. Hypertension and the type of recipient vein are associated with venous thrombosis (P = .018, P = .047). Hypertension, type of free flap, recipient artery, and recipient vein were associated with the incidence of re-exploration (P = .009, P = .011, P = .017, P = .021). Hypertension had an obvious effect on the flap survival (P = .005). For multivariate analysis, hypertension (odds ratio = .166, 95% confidence interval: .043 – .636; P = .009) was a statistically significant risk factor for flap survival. For types of recipient artery and vein, selecting two venous anastomosis (one of IJVS and one of EJVS) had the minimum incidence of venous thrombosis (2.2%), and selecting facial artery, single vein (one of IJVS), and two veins (one of IJVS and one of EJVS) for anastomosis had lower incidence of re-exploration, which were 4.4%, 2.9%, and 6.0%, respectively (P < .05).
Conclusions
Risk factors as hypertension, type of free flap, recipient artery and vein should be paid more attention in the free flaps for head and neck reconstructions. We believe proper measures will lead to better results in head and neck reconstruction.
Inroduction
Free flap transfer has become an integral part of the treatment for complex and large defects of head and neck, with a high success rate of over 95%.1-3 Despite the reliability of microvascular reconstruction, varieties of risk factors can cause complications and even failure of free flap. The risk factors can be simplified into three basic components that include the preoperative evaluation and selection of the patient, intraoperative technique and circumstances, and post-operative management.4,5 Preoperatively, patient comorbidities such as tobacco usage, past radiation, age, and prior head and neck surgery have all been debated as potential causes of flap failure. Intraoperative etiologies of flap failure typically involve surgical decisions including recipient vessels, pedicle geometry, and microsurgical technique. Postoperatively, it is important to maintain hemodynamic stability and control the external milieu, including monitoring of free flap, use of antithrombotic agents, and taking back to the operation room.5-7
It can be challenging reconstruction for the cases who are posed by previously treated necks with either surgery or radiation with or without chemotherapy. Due to the previous history of neck surgery and/or radiotherapy, patients with these prior interventions have cervical anatomy with distorted tissue planes, inflammation, and scarred vessels leaving a patient’s neck depleted of suitable recipient vessels.8,9 The lack of available blood vessels or severe fibrosis, anatomical difficulties of tissue, and long-term healing process are considered as obstacles of microsurgical repair and reconstruction. In recent years, with the improvement of microsurgical technology, senior authors adopt to the application of transverse cervical vessels, superficial temporal vessels, thoracoacromial artery, internal mammary artery, dorsal scapular artery, and cephalic vein as recipient vessels. However, there is no consensus on the choice of recipient vessels for the reconstruction for vessel-depleted neck.9-13 The scenario of the vessel-depleted neck thus requires careful surgical planning and consideration of alternative vessel sources or reconstructive techniques for successful surgical outcomes.14,15
We hereby present a retrospective study of collected data to evaluate our experience and compare the rates of complications and flap loss of different possible risk factors. The aim is to come up with a strategy for the reconstruction for head and neck.
Methods
Patients
A retrospective review of 318 free flaps used for head and neck reconstructions in 317 patients during the period of November 2012 to December 2019 was performed. 295 flaps were reconstructed for the first time, 22 for the second time, and 1 for the third time. In our center, all reconstruction cases underwent strict preoperative screening and preparation and were performed by experienced head and neck surgeons and are under careful surveillance postoperatively. Flap monitoring was consistently performed by observing the surface color, turgor, capillary refill, and pinprick test every hour for the first 72 hours, every 3 hours for the next 48 hours with gradual tapering to every 8 hours until day 7. When impaired circulation or other crisis was identified, the patient was immediately taken back to the operating room for re-exploration. All patients who underwent emergent re-exploration due to flap compromise within 7 days after the initial operation. The patient characteristics and surgical data, including patient age, sex, diabetes mellitus, hypertension, smoking, type of flap, and type of recipient vessels, were recorded. The primary outcome measurements were determined as follows: incidence of arterial and vein thrombosis, hemorrhage or hematoma, infection and rates of re-exploration, successful salvage, and total flap survival.
Data analysis
We compared these groups(categorical characteristics) by univariate analysis using X2 test or Fisher exact test to identify each possible risk factor for outcome. The outcomes include: arterial thrombosis, venous thrombosis, infection, hemorrhage & hematoma, infection, re-exploration, successful salvage, and flap survival. Multivariate logistic regression was performed to evaluate the association of the categorical characteristics with the total flap survival while controlling for possible confounders. Variables included: age, sex, hypertension, smoking, type of flap, type of recipient artery, and the type of recipient vein. Odds ratios (OR) with 95% confidence intervals were investigated. All measured data were analyzed using SPSS version 20.0 software (SPSS Inc., Chicago, IL, USA). P < .05 was considered statistically significant.
Results
Among the 295 cases of free flaps that were reconstructed for the first time in our center, 100(33.9%) cases were older than 60 years old and 195(66.1%) cases were younger than 60 years old. Among them, there were 205(69.5%) males and 90(30.5%) females. In statistics, there were 74(25.1%) cases of hypertension and 28(9.5%) cases of diabetes mellitus. The number of smoking cases was 148 (50.2%) which is similar to that of non-smoking cases (147, 49.8%). Free flaps utilized in this study included the radial forearm flap (RFF) (n = 123, 41.7%), the anterolateral thigh perforator (ALT) flap (n = 71, 24.1%), the fibular flap (n = 87, 29.5%), the superficial circumflex iliac artery perforator(SCIAP) flap (n = 8, 2.7%), the deep circumflex iliac artery perforator (DCIAP) flap (n = 2, 0.7%), and other various free flaps (n = 4, 1.3%). For recipient arteries, the superior thyroidal artery (STA
Single factor analysis
Impact of Patient Characteristics on Flap Survival.
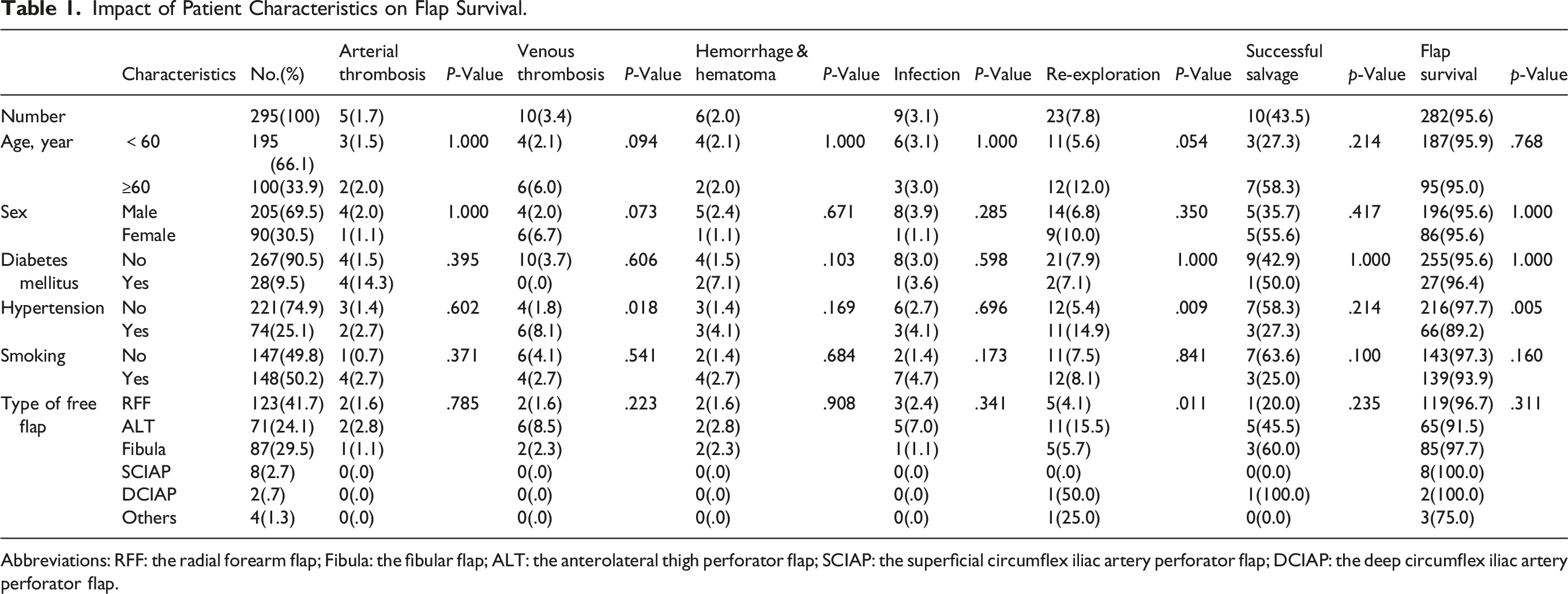
Abbreviations: RFF: the radial forearm flap; Fibula: the fibular flap; ALT: the anterolateral thigh perforator flap; SCIAP: the superficial circumflex iliac artery perforator flap; DCIAP: the deep circumflex iliac artery perforator flap.
Impact of Parameters Related with Recipient Artery and Vein Features on Flap.
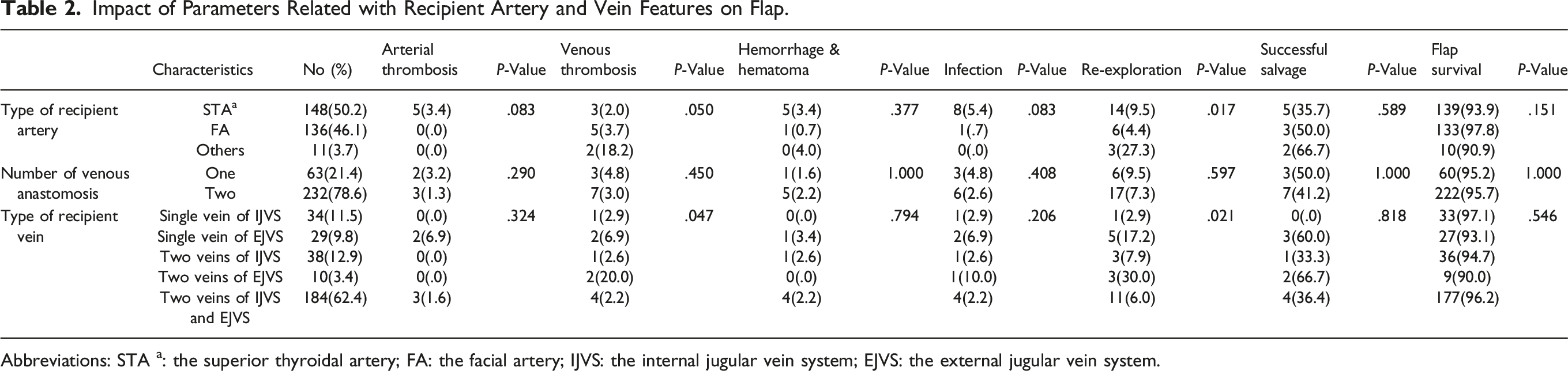
Abbreviations: STA a: the superior thyroidal artery; FA: the facial artery; IJVS: the internal jugular vein system; EJVS: the external jugular vein system.
Multivariate analysis
Binary Logistic Analysis for Total Flap Survival.
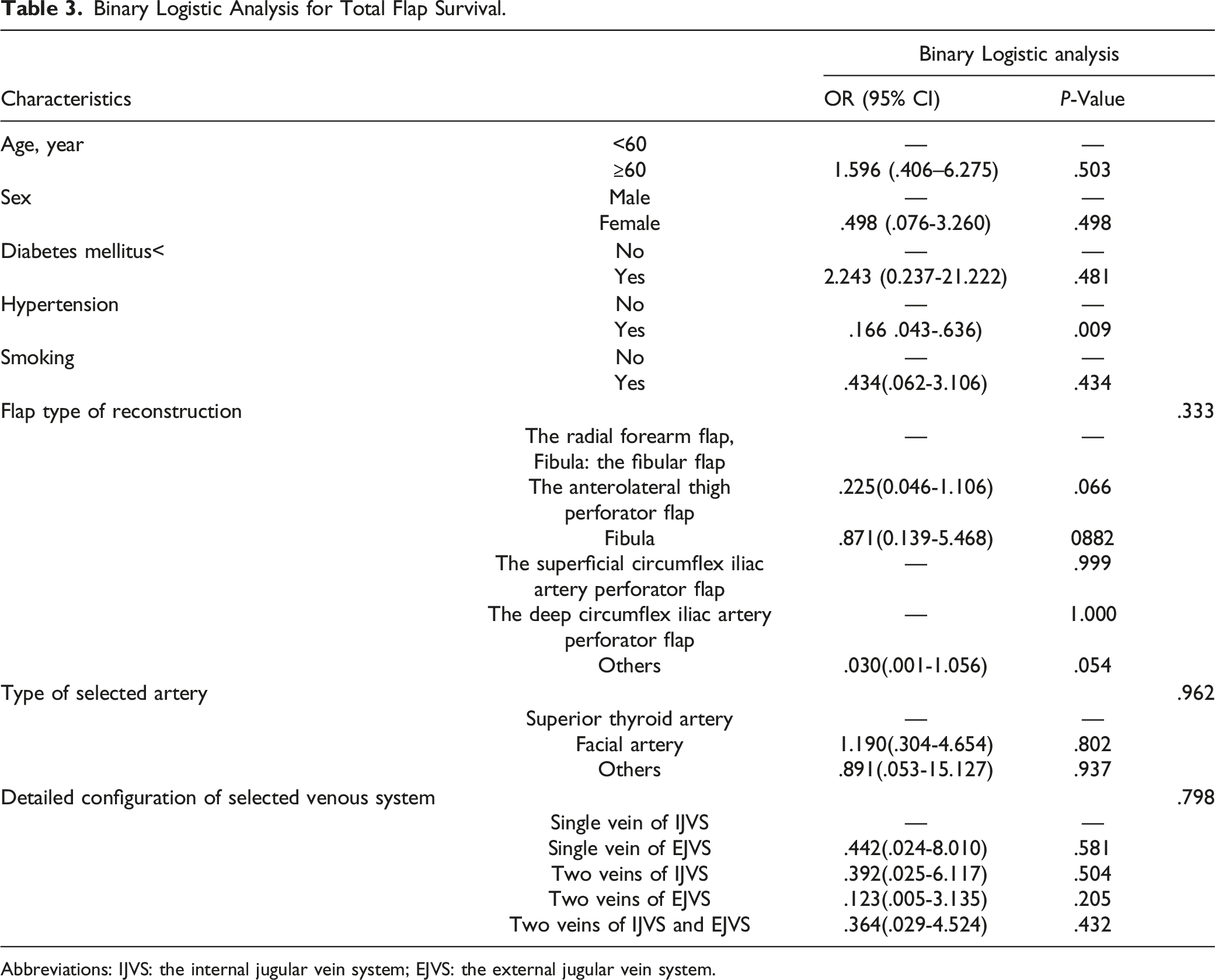
Abbreviations: IJVS: the internal jugular vein system; EJVS: the external jugular vein system.
For secondary reconstruction
Data of Secondary Reconstructive Surgery.
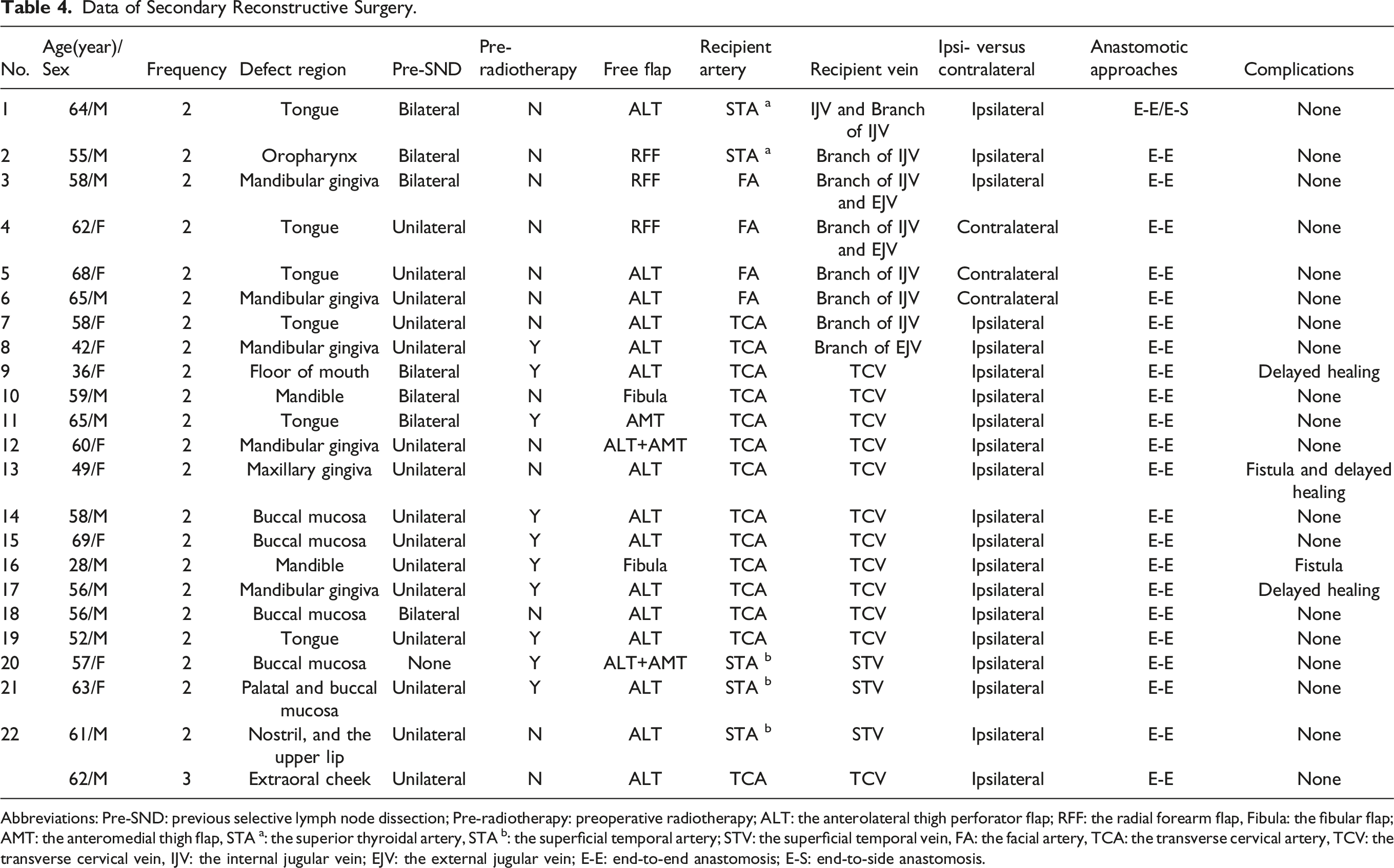
Abbreviations: Pre-SND: previous selective lymph node dissection; Pre-radiotherapy: preoperative radiotherapy; ALT: the anterolateral thigh perforator flap; RFF: the radial forearm flap, Fibula: the fibular flap; AMT: the anteromedial thigh flap, STA a: the superior thyroidal artery, STA b: the superficial temporal artery; STV: the superficial temporal vein, FA: the facial artery, TCA: the transverse cervical artery, TCV: the transverse cervical vein, IJV: the internal jugular vein; EJV: the external jugular vein; E-E: end-to-end anastomosis; E-S: end-to-side anastomosis.
Discussion
The defects of head and neck often have a great impact on the patient's language, eating, swallowing and appearance, which are closely related to the patient's quality of life. Since the introduction of microvascular free tissue transplantation was firstly proposed in the 1970s, the reconstruction of head and neck defects had become possible and greatly improved the patient’s quality of life.1,16,17 Despite the great success of free flap transplantation, failure still exists.
There are many risk factors for the flap failure. In this study, we studied the risk factors of age, sex, smoking, the type of flap, the type of recipient artery, the number venous anastomosis, and the type of recipient vein on the outcomes of free flap.
In terms of age, most studies had proved that age is not a contraindication for head and neck free flap transplantation unless combined with multiple complications.7,18 According to the definition for the elderly of WHO and in China, we divided the patients into 2 groups: ≥60 years old and < 60 years old in this study.19,20 The results are the same as the previous studies that age has no effect on the success and adverse outcomes of free flap.3,7
The adverse effects of diabetes mellitus are related to the microangiopathic changes that occur within the skin and muscle. Experimental studies using rats have demonstrated that the degree of intimal repair and endothelialization is lower in poorly controlled patients with diabetes that can lead to anastomotic failure. 21 Also in one clinical study and one meta-analysis, Valentini et al.22,23 concluded that diabetes mellitus was significantly associated with adverse post-operative outcomes. They also argued to use local flaps as much as possible than free flaps for the reconstruction of head and neck defects in diabetic patients. However, flap failure only occurred in 1(3.6%) of 28(9.5%) diabetic patients and 12(4.5%) of 267(90.5%) non-diabetic patients, in our study. Diabetes has no obvious relationship with the poor prognosis and failure of free flap.
As for hypertension, there was still no relevant study to prove that hypertension is associated with the adverse outcomes between patients with and without hypertension. Since we found that the hypertension history was related to thrombosis and re-exploration in this study, we then collected blood pressure data of 30 patients (including 12 patients with hypertension history) with post-operative complications or re-exploration for 8 post-operative days. We screened the daily blood pressure of each patient, selected the 3 blood pressures with the highest systolic blood pressure (SBP) to calculate their average value and then analyzed them, which was shown in Supplemental Material Table 1. According to the definition of hypertension of International Society of Hypertension Global Hypertension Practice Guidelines, 24 the mean SBP of 30 patients were higher than 140 mm Hg in 7 days within 8 days post-operation, but it could not be proved to be related to post-operative complications or re-exploration. Wang et al. found that elevated systolic blood pressure increased the risk of hematoma formation, and they recommended keeping systolic blood pressure below 150 mm Hg to prevent hematoma. 25 Therefore, we suggested that blood pressure should be paid attention during the perioperative period.
In terms of smoking, our study did not find that smoking patients had a higher frequency of adverse outcomes. However, there was study suggested that current smokers and those who quitted less than 3 weeks before surgery had a significantly higher risk of impaired wound healing and encouraged the patients to abstain from using tobacco products for at least 3 weeks before surgery. 26
When talking about the type of free flaps in the head and neck defects, it is well-known that fibula flap is associated with higher complication rate compared to soft tissue flaps. 27 However, the re-exploration occurred in 5(4.1%) of 123 the RFF flaps, 11(15.5) of 71 the ALT flaps, 5(5.7%) of 87 the fibular flaps, 1(50%) of 2 the DCIAP flaps, 1(25%) of 4 the other flaps, and none of the SCIAP flap in our study, and the difference was statistically significant (P = .011). We considered that the high rate of re-exploration in the ALT flap and the DCIAP flap might be related with the unsteadiness of the perforator. With the development of medical imaging technology, in order to optimize the operation, we usually used Doppler and CTA technology to detect and locate the perforator on the donor site for the free flap before operation and chose the most reliable perforator during operation.
In our study, the superior thyroidal artery (STA
At present, the choice of recipient vein was still a hot topic. There have been studies proving that dual venous anastomosis had a higher success rate of free flap because dual venous anastomosis could provide better blood drainage.28,29 In this study, there was no significant difference between single venous anastomosis and dual venous anastomosis in the outcomes of the free flap. Our previous studies have shown that the IJVS was the priority for head and neck reconstruction when single venous anastomosis would be performed. 30 But the EJVS was still a reliable choice when the IJVS is not available. 5 In terms of detailed configuration of selected venous system, two veins of IJVS (2.6%) and two veins (one of IJVS and one of EJVS) (2.2%) showed a lower incidence on venous thrombosis, and single vein of the IJVS (2.9%) and two veins(one of the IJVS and one of EJVS) (6.0%) showed a lower incidence on re-exploration. Therefore, we had the reason to think that the IJVS was preferred in single venous anastomosis, and two veins(one of IJVS and one of EJVS) was preferred in dual venous anastomosis. Clinically, we chose end-to-end anastomosis as long as the size of donor vein and recipient vein matched. However, end-to-side anastomosis overcomed the problem of vascular mismatch and achieved a similar success rate.31,32 With the introduction of coupler device into head and neck reconstruction, it has been widely welcomed, which can shorten the operative time and improve the success rate of free flap.33,34 We would use it in patients who can afford it economically since the coupler device was introduced in our center.
Prior surgery and radiation make the second reconstruction a highly challenging aspect, which often result in significant scarring and damage to the neck vasculature. Therefore, the choice of recipient vessels is the key of secondary reconstruction.15,35 Because the transverse cervical vessels are located deep in the neck and rarely affected by radiation therapy, they are favored by head and neck surgeons. Urken et al. 36 once documented their use of the TCA as their primary and utmost preferred recipient artery for head and neck free flap reconstruction. Tessler et al. also believed the transverse cervical vessels are reliable and accessible recipient vessels based on 19 patients.13,15 The superficial temporal vessels, located in the preauricular region, were usually unaffected by previous surgery or former irradiation and are constant in anatomy and are used by many surgeons.12,37 It has been reported that thoracoacromial artery, internal mammary artery, cephalic vein transposition, and vein graft can also be used in vessel-depleted neck.38-40 But these techniques are unfamiliar to head and neck surgeons, which makes the procedure more difficult. The superficial temporal vessels were used in the upper third of the head and the transverse cervical vessels for the lower third of the face as the priority in our center. Therefore, for 22 patients in secondary reconstruction, the transverse cervical vessels were used in 12 patients and the superficial temporal vessels were used in 3 patients. Clinically, we used CTA technology to evaluate the vascular condition of the patient's neck carefully. When the superficial cervical and transverse temporal vessels were not available due to variation or deletion, we would we dissected the ipsilateral and contralateral vessels that were relatively well conditioned or not affected by Pre-SLND or pre-radiotherapy for anastomosis. In our study, secondary reconstruction was successful in 22 patients.
This study has the following defects. First, this was a retrospective review performed at a single institution that was entirely dependent on medical records; in addition, patients were not randomized. Second, a total of 491 free flaps were performed in this center from November 2012 to December 2019. Due to incomplete case data, 173 cases were excluded and only 318 cases with complete case data were included. Therefore, there may be some deviation in the results. Third, risk factors such as the use of coupler device and anticoagulants were not analyzed in this study, and the study results were not comprehensive enough. Therefore, more quality research to extract more accurate is needed in the future data to validate the results of this experiment.
Conclusion
In conclusion, risk factors as hypertension, type of free flap, type of recipient artery, and type of recipient vein should be paid more attention in the free flaps for head and neck reconstructions. It is vital that the patients with hypertension controlling their blood pressure during the perioperative period.
Footnotes
Acknowledgments
Thanks to all who have contributed and all the patients in our research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the ethics committee for human experiments at the China Medical University, School and Hospital of Stomatology. (201815)
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.