
Abstract
Patients who fail to commit suicide by hanging often end up with laryngotracheal injuries, which may lead to a compromised airway, swallowing dysfunction, and dysphonia. Previous studies have mainly focused on airway management after near-hanging attempts. Few have shed light on the treatment of swallowing dysfunction after laryngotracheal injuries. Here, we present a near-hanging patient who developed complete dysphagia shortly afterward. We used a Montgomery T-tube as an endolaryngeal stent, combined with swallowing rehabilitation. The patient’s swallowing ability was gradually restored one month after the surgery, and the stent was removed six months later. The present case report exemplifies the unique way of using the Montgomery T-tubes in clinical practice. Among the patients with airway stenosis affecting the larynx and extending to the vocal cords, Montgomery T-tube may be the only stent that can help manage strictures at the level of the vocal cords and in the supraglottic region, restoring swallowing function and maintaining the airway.
Introduction
Over the past decade, hanging has been the most used method of suicide in Taiwan. The mortality rate is approximately 70%. 1 Near-hanging patients are those who are rescued and sent to the hospital alive after a suicide attempt. Of these patients, 64%–90% survive. 2 We may underestimate laryngeal trauma in the initial assessment because of the non-specific presentation. The patient with compression injury by strangulation may initially present with deceptively mild symptoms and signs but develop acute airway obstruction several hours later. Laryngeal injuries can lead to unexpected, delayed death or permanent laryngotracheal sequelae if left untreated. To date, most studies on near-hanging cases have focused on airway management. Few have shed light on the treatment of dysphagia and documented it only as case reports.
Dysphagia caused by laryngotracheal stenosis in patients with post-laryngotracheal trauma can be managed with laryngotracheal repair and stenting, including the use of the Montgomery T-tube, 3 along with nonsurgical treatment, such as swallowing maneuvers, diet modification, and fluid thickening. 4
The Montgomery T-tube is a T-shaped silicon tube used to provide support in the stenotic trachea. Its use as the definitive management of patients with blunt laryngeal injury has been described in a case series in which over half of the patients showed satisfactory results in maintaining airway patency and enhancing voice clarity. 3 We described the management of a patient with dysphagia following an attempted suicide by hanging, and discussed restoring the patient’s swallowing function using the Montgomery T-tube for reconstruction along with swallowing rehabilitation.
Case Report
The patient is a 47-year-old woman without any underlying disease or psychiatric history. She also denied having suicidal ideation or depression. She was sent to the local emergency room by her family after a suicide attempt by hanging. On arrival, she was fully conscious. The airway was adequate, and her hemodynamics were stable. Hoarseness, sore throat, and dysphagia were present, with no symptoms or signs of respiratory distress. A neck examination revealed a transverse linear bruise over the anterior neck with swelling.
Nasopharyngofiberscopy revealed swelling and edema of both arytenoids. A laryngeal laceration was present at the posterior commissure, extending from the post-cricoid to the esophageal orifice. There was no acute airway obstruction, and the trachea was patent to the level of the carina. In considering the progression of soft tissue swelling and subcutaneous emphysema, tracheostomy for airway protection was suggested in the first place. However, the patient refused further management.
Urgent computed tomography (CT) of the neck and chest showed a cricoid cartilage fracture, extensive subcutaneous emphysema in the neck region, and pneumomediastinum. There was no spinal fracture noted. Brain CT showed no evidence of hypoxia and ischemic changes in the brain.
The patient developed respiratory distress due to progressive subcutaneous emphysema and laryngeal edema. Desaturation was evident 5 hours later (SpO2 89% under room air), and the anesthesiologist performed endotracheal intubation gently with glidescope. The patient was admitted to the intensive care unit for stabilization. Eight days later, the patient was successfully extubated. She was then referred to our laryngologist for further treatment.
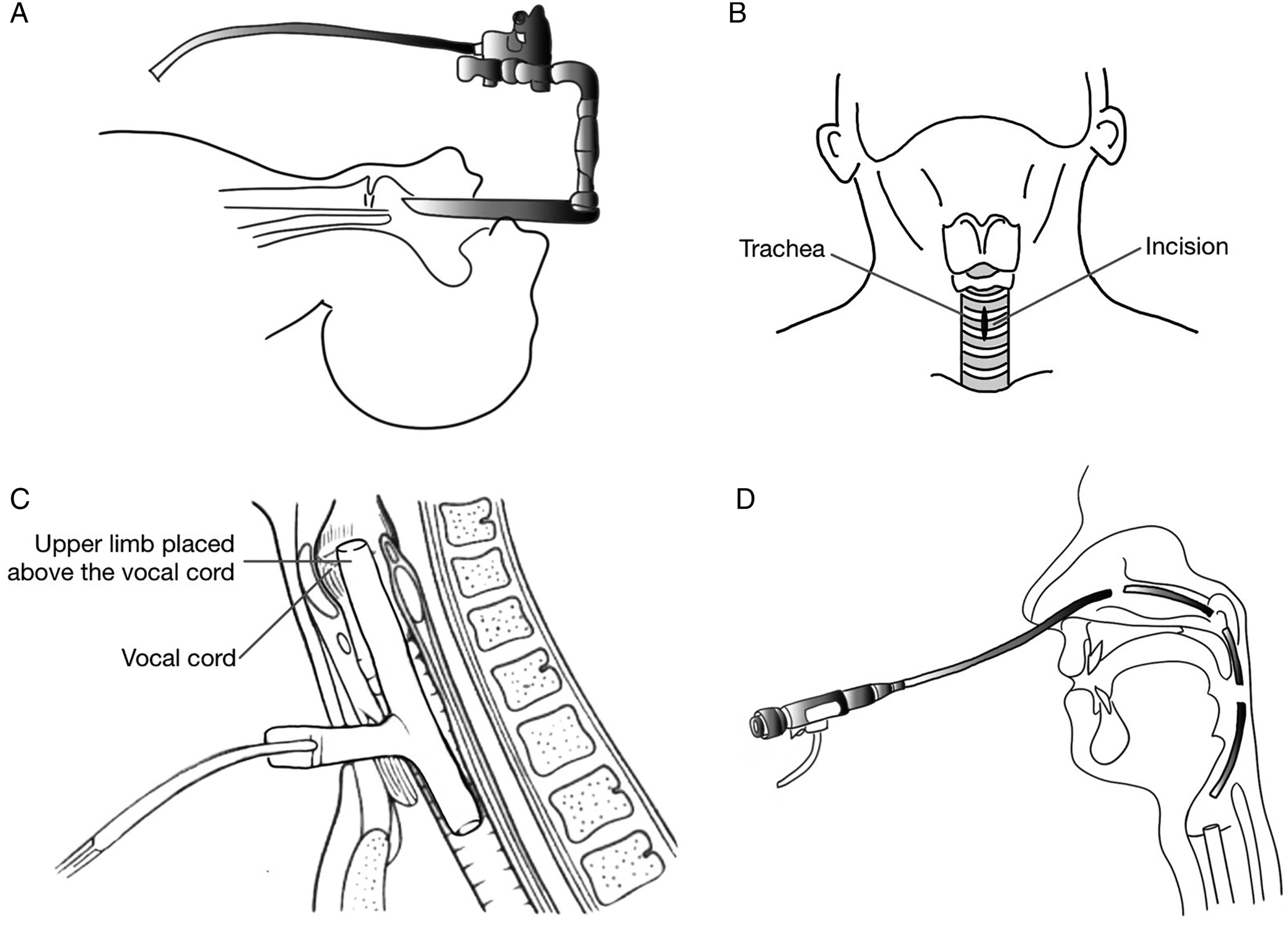
After admission, flexible fiberscope revealed bilateral vocal cord immobilization in the intermediate position, left arytenoid deformity with depression, mimicking type IV posterior glottic stenosis (Figure 1A and B). Preoperative computed tomography of the larynx and hypopharynx revealed dislocation of the left arytenoid and fracture of cricoid cartilages (Figure 1C and D). After careful evaluation, we performed surgical repair of the larynx using a Montgomery T-tube stent. The detailed surgical procedure is described in the diagrams below (Figure 2). Preoperative examination of CT scan and fiberscope showed (A) bilateral vocal cord immobilization in an intermediate position with a glottal gap, (B) left arytenoid deformity and depression with saliva pooling, (C) arytenoid fracture, and (D) cricoid fracture. A nasogastric tube was inserted due to dysphagia. Surgical procedures of Montgomery T-tube insertion. (A) Step 1. Under general anesthesia with spontaneous ventilation, microlaryngoscopy and bronchoscopy were applied to examine the degree and extension of laryngeal stenosis. (B) Step 2. Standard procedure of tracheostomy was performed with an incision made at 2nd to 3rd tracheal rings midline vertically. (C) Step 3. Define the length of the upper limb by measuring the distance from the tracheostomy site to ½ height of thyroid cartilage. The Montogomery T-tube was placed by inserting the upper arm first, then push the lower arm into the tracheal lumen by Kelly-Rankin Hemostatic forceps. (D) Step 4. Flexible nasopharyngoscope to check if the upper limb of the T-tube is above the vocal cord.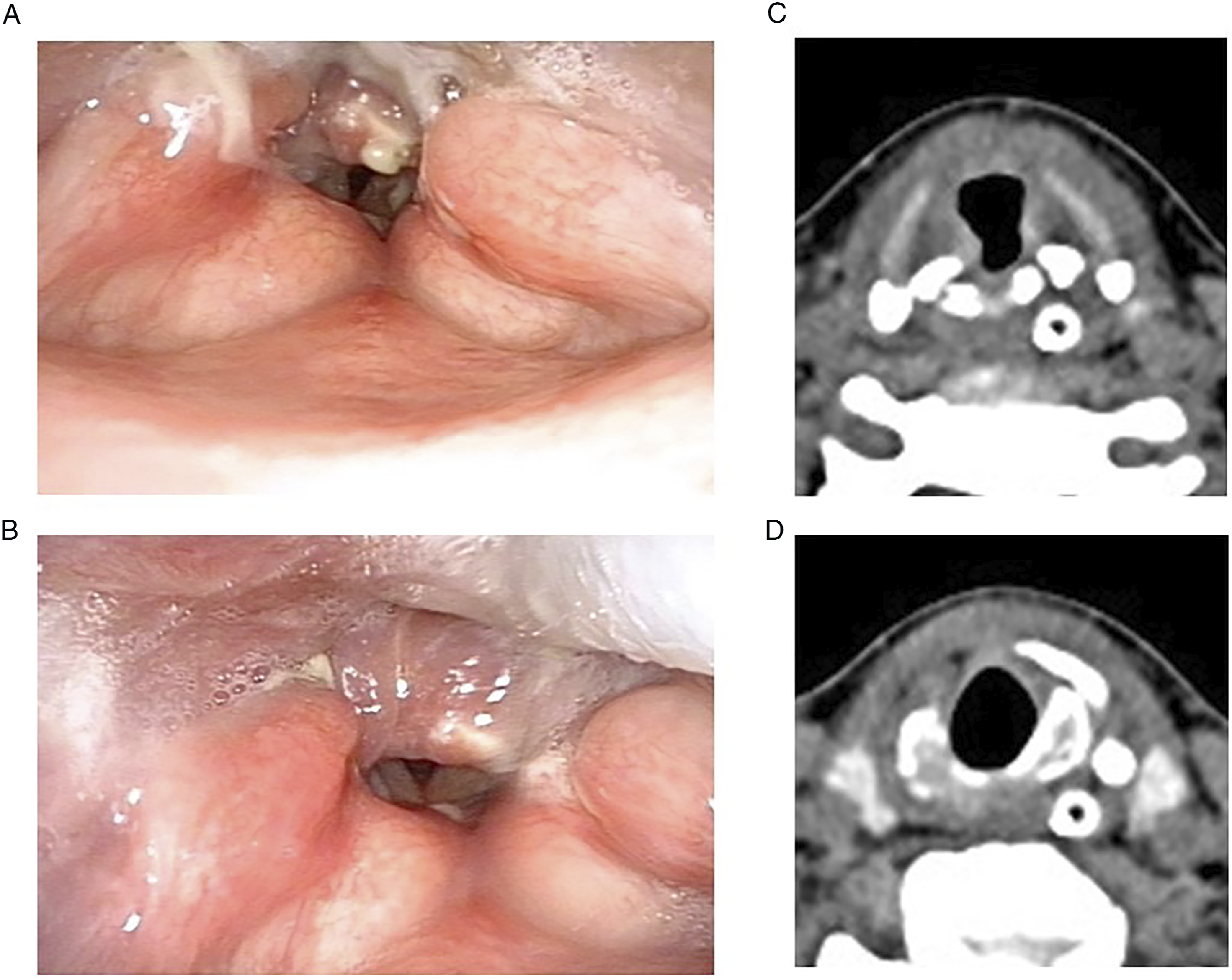
A Montgomery T-tube, Thoracic Safe T-tube (5200 series) (size 11) (Boston Medical; Boston, USA), was inserted under general anesthesia. The upper limb of the T-tube was placed in the transglottic position and across the bilateral arytenoid cartilage depression to maintain patency of the supraglottic pathway (Figure 3A). Postoperative fiberoptic findings revealed (A) a Montgomery T-tube in the transglottic position, and a nasogastric tube in place. (B) 3 ml of blue water during fiberoptic endoscopic evaluation of swallowing (FEES) test 1 week after the surgery and showed no residue over the pyriform sinus. (C) Montgomery T-tube was removed six months after insertion. (D) Arytenoids fused with the cricoid cartilage at the posterior cricoid area.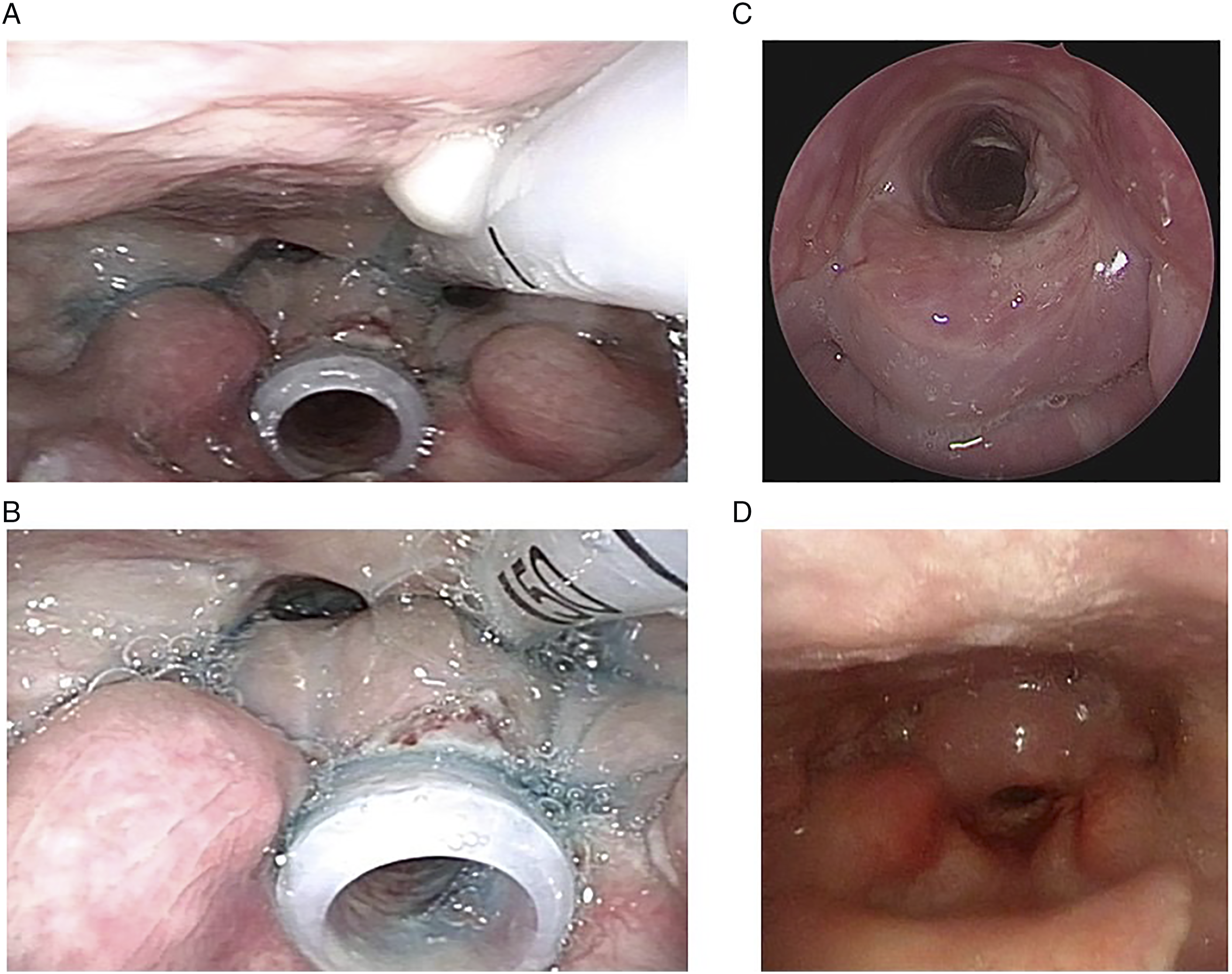
After laryngotracheal reconstruction with a Montgomery T-tube, the patient still demonstrated severe dysphagia symptoms with aspiration. The laryngologist and the speech-language pathologist assessed the fiberoptic endoscopic evaluation of swallowing (FEES) test with a small amount of pure blue water (Figure 3B). Swallowing rehabilitation was implemented, including swallowing exercises and compensatory swallowing strategies such as posture change, bolus consistency modification, and tongue-based strengthening exercises.
After 2 weeks of swallowing rehabilitation, the patient could swallow water without choking or gagging. She also started trying food with a thicker consistency, such as porridge, steamed eggs, and juice.
One month after the operation, the patient could swallow water, porridge, bread, and rice without aspiration. We then removed the nasogastric tube. Three months after the operation, the patient tolerated a regular diet. The Montgomery T-tube was kept there for 6 months to stabilize the laryngeal structures. After removing the T-tube, we inspected the airway using a ventilation bronchoscope (Figure 3C). The arytenoids were fused with the cricoid cartilage in the post-cricoid area, and there was minimal tracheal granulation tissue at the distal tip of the T-tube where it was previously placed.
Approximately 1 year after the operation, the patient tolerated normal fluid and solid food intake. The fiberscope showed type IV posterior glottic stenosis and limited movement of the bilateral vocal cords at the intermediate position (Figure 3D). Although she still had a breathy voice, we were able to preserve a functional airway. She was able to perform mild to moderate physical activities comfortably and complained of breathlessness only at an intense level of physical activity.
Discussion
Laryngotracheal trauma caused by hanging is often severe and life-threatening. Most victims die on-site due to hypoxia and cerebral ischemia caused by compression of the airways and major vessels, resulting in death. 5 However, they may not always be fatal, in which case, they are termed a "near-hanging." A near-hanging patient is at risk of blunt injury to the neck structures because of direct compression or cervical extension. Studies on the management of laryngotracheal injuries in near-hanging patients mainly stressed the importance of maintaining the integrity of the airway to support adequate ventilation but provided little information on the restoration of swallowing ability and phonation.6-9 Of the few studies that discussed the treatment of dysphagia after airway reconstruction,10-13 swallowing rehabilitation is essential for the recovery of swallowing function.
Following the attempted hanging, our patient sustained a cricoid cartilage fracture. Arytenoid dislocation and bilateral vocal cord immobility occurred later, with a functional oral intake scale level 1 dysphagia. A preoperative CT scan revealed multiple cricoid cartilage fractures and arytenoid dislocation. Flexible fiberscope found left arytenoid dislocation and bilateral vocal cord immobility. Therefore, cricoarytenoid joint dislocation or fixation was first impressed. In this case, we did not perform a laryngeal electromyogram (EMG). Although the laryngeal EMG can be performed to establish a differential diagnosis of vocal cord immobility between nerve injury and joint fixation, it is still difficult to determine the definite cause of bilateral vocal cord immobilization via strangulation or intubation.
Based on literature review, there are some controversies regarding managing acute blunt laryngeal trauma. First, the initial method of securing the airway with laryngotracheal trauma is undetermined. Intubation after laryngotracheal trauma may cause laryngeal injury and damage to the supporting structures, contributing to the deterioration of airway patency. 14 Tracheostomy should be the only procedure performed under this circumstance. However, advances in video-assisted intubation and glidescope are improving; intubation may be a feasible method and is worth exploring further. 15 Second, the ideal treatment option for acute laryngotracheal trauma is unavailable. The various approaches and the techniques described over the decades demonstrate the limitations of current therapies. 16 Injections of steroids into the cricoarytenoid joint may reduce inflammation, but there are no medical therapies currently approved to reverse fibrosis. Furthermore, surgical treatment to remove or release the scar, including incision of the interarytenoid scar and dilatation of the glottic stenosis, is restricted in its ability to restore laryngeal function and maintain the delicate balance between voice, airway, and swallowing. In most cases, surgical therapies disrupt that balance to preserve swallowing, maintain voice and create a functional airway. Posterior cricoid split, suture lateralization, and posterior cordotomy with partial arytedoidectomy are procedures to maintain the airway but endure the loss of voice.
Based on the flexible nasopharyngoscope and CT scan findings, acute laryngotracheal trauma and posterior cricoid cartilage multiple fractures mimicked type IV subglottic stenosis. Among patients with subglottic stenosis involving the larynx and extending to the vocal cord (type IV subglottic stenosis), Montgomery T-tube may be the only stent that can help manage strictures at the level of the vocal cord and supraglottic region. 3 Therefore, we decided to use the Montgomery T-tube rather than a simple tracheostomy for this patient. Moreover, the Montgomery T-tube provides a framework for the larynx to heal and stabilize. Edematous laryngotracheal obstructions can gradually be improved with Montgomery T-tube airway restoration, avoiding an invasive surgical procedure. In most situations, the Montgomery T-tube is placed with its proximal end distally to the conus elasticus of the subglottic larynx to minimize the risk of developing subglottic edema or granulomas. However, in this case, the upper limb of the T-tube was placed "above" the cord. There is a significant risk of a whispered voice and aspiration. 17 To minimize the risk of aspiration, the T-tube was placed above the cord but below the AE fold. Besides, we combined nonsurgical treatment options to manage dysphagia. The T-tube stent supports the forward movement and elevation of the hyoid-laryngeal box during the swallowing process, which is essential for the action to carry out smoothly. The remodeling phase of a wound starts at approximately three weeks and can last up to 1 year or more. During this stage, the wound may achieve maximum tensile strength in the attempt to recover normal tissue structures 18 and subsequently, the patient's swallowing function. Six months later, we removed the T-tube stent.
Dysphagia encompasses a wide range of etiologies. Most cases of dysphagia do not require surgical intervention to achieve safe swallowing and optimal nutrition and hydration. Videofluoroscopic swallowing study (VFSS) and fiberoptic endoscopic evaluation of swallowing (FEES) are common instrument modalities used to assess swallowing function. VFSS has been widely recognized as the gold standard for diagnosing dysphagia. Due to the total inability to swallow and aspiration in our patient, we did not perform VFSS. On the contrary, we chose FEES, which is easier to perform, widely accessible, repeatable, and has no risk of radiation exposure. With the aid of real-time FEES, the patient received swallow rehabilitation after the surgery.
When choosing a stent for benign subglottic or higher tracheal disease, the advantages of T-tubes include easy suctioning of respiratory secretions, easy removal in cases of acute obstruction, and seldom migration. As we have mentioned, when the proximal end of the T-tube is positioned above the vocal cords to stent the supraglottic area, complications, such as aspiration and voice weakening, may be encountered. 19 Our patient encountered a cricoid cartilage fracture, and we placed a T-tube stent to support the posterior wall of the cricoid. The upper limb was placed above the cord but below AE fold to reduce the risk of aspiration. Other complications associated with Montgomery T-tube insertion include infection, granulation at the distal or proximal end of the tube, may sometimes come into contact with the cords, and bacterial colonization or crust formation in the lumen. Tracheomalacia may also occur in areas adjacent to the tube edges. Furthermore, there is a possibility of obstruction of the tube or difficulty in removing the secretions from the T-tube. 3
Conclusion
Montgomery T-tube is a good choice and feasible method for endolaryngeal stenting in near-hanging patients with subsequent laryngotracheal trauma. It maintains the airway's patency and stabilizes the laryngeal framework, which is essential for hyoid-larynx elevation of the swallowing process. Combined with swallowing rehabilitation, our patient was able to preserve a functional airway and restore swallowing function.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.