
Abstract
Background:
Under the background that cervical plexus block (CPB) is often adopted for type I thyroid cartilage laryngoplasty (TCL) and vocal cord medialization (VCM), the present study sought to investigate whether ultrasound-guided CPB (USCPB) could improve the efficiency of type I TCL and VCM.
Methods:
Patients with TCL were enrolled and subjected to deep and superficial USCPBs. Intravenous dexmedetomidine pumping was used to assist the painless sedation and ensure the patients to be awake for phonation during surgery. Blood pressure, electrocardiogram, heart rate (HR), and blood oxygen saturation (SpO2) of patients were recorded. The complications, like local anesthetic toxicity and total spinal anesthesia, were monitored.
Results:
All patients underwent CPB without infiltration anesthesia and complication. The use of Sufentanil at the dose of 5–10 μg was reported in 2 of 15 patients. No Horner syndrome was discovered in patients after anesthesia, and total intravenous anesthesia with intravenous pumping of dexmedetomidine was effective. During surgery, HR, diastolic blood pressure and mean blood pressure were barely changed, but systolic blood pressure was decreased.
Conclusion:
Ultrasound-guided CPB with the intravenous dexmedetomidine pumping is a safe anesthesia method for patients during TCL.
Keywords
Introduction
Vocal cord paralysis (VCP) is the partial impairment of vocal cord motor, caused by the nerve or neuromuscular abnormality, which affects glottic closure and further leads to voice impairment. Hence, some serious and life-threatening complications emerge in the form of voice, swallowing, and respiratory difficulties. 1 VCP may be unilateral or bilateral. In terms of unilateral VCP (UVCP), the paralyzed site tends to be shortened accompanied with the anterior rotation of arytenoid, and the left vocal cord is affected more often than the right. 2 Currently, laryngeal electromyography (LEMG) and video laryngostroboscopy (VLS) are primary techniques responsible for assessing the condition of patients with VCP. Of them, LEMG, as an effective means to evaluate the neuromotor function, can identify the impairment in neural transmission and muscle activity. VLS is a method of vocal cord visualization applied to evaluate the disorders on the vocal cord. 3
Previous studies have additionally evidenced the roles and efficacy of both type I thyroid cartilage laryngoplasty and vocal cord medialization when treating VCP in clinical practice.4,5 Type I thyroid cartilage laryngoplasty is usually adopted for improving dysphonia caused by VCP, during which a rectangular thyroid cartilage is firstly removed on the involved side, followed by implant placement to shift the vocal cord to the midline. Vocal cord medialization, whose efficiency is proved in treating abductor spasmodic dysphonia (SD), mainly focuses on modifying the structure of vocal cord to restore the normal phonation. 6 However, a precise surgery is difficult to conduct on the larynx of the patients who are awake, due to the reflex responses caused by the manipulation on the larynx. 7 Therefore, further viable and better anesthesia strategies are required during the treatment of VCP.
The past decades have witnessed the increasingly wider application of ultrasound-guided regional anesthesia (UGRA) by virtue of its ability to safely and effectively relieve the pain suffered by patients. 8 Compared with other traditional nerve localization techniques, ultrasound reduces the dosage of local anesthetic and avoids the needle-induced hazardous mechanical trauma to the nerve. More specifically, ultrasound increases the probability of success, hastens the onset of nerve block, and reduces the serious adverse effects of the complications (like vascular puncture) and the toxicity caused by local anesthesia. 9 The cervical plexus block (CPB) is a method providing effective anesthesia and analgesia for the head and neck regions. Under the guidance of ultrasound with increasing impacts on the head and neck regions, CPB can be conducted in a more safe and accurate manner. Also, CPB is used to identify some important hallmarks, such as muscles, cervical vertebrae, large vessels, nerves, and cervical fascia. 10 The current study, hereby, aims to evaluate the efficacy of ultrasound-guided CPB in type I thyroid cartilage laryngoplasty and vocal cord medialization surgery, looking forward to authenticating its potential application in the treatment of VCP in clinical practice.
Methods
Ethics Statement
The Ethics Committee of Fujian Provincial Hospital has reviewed and approved the conduction of this study (endorse number: K2020-09-078). Meanwhile, all recruited patients or their legitimate guardians have signed the written informed consent before participating in this study.
Patients and Treatment Regimen
A total of 15 patients, including 11 males and 4 females treated in Fujian Provincial Hospital from Jan. 2017 to Dec. 2019, were enrolled in thyroid cartilage laryngoplasty. The recruited patients were in physical status grade I to III according to American Society of Anesthesiologist (ASA) and aged 36 to 75 years old.
Patients were subjected to surgery on the premise of routine fasting, and their upper limb venous access was opened after entering the operation room. The transfusion of lactated Ringer’s solution (BMGL7501, Medline Industries, Mundelein, IL) was maintained, and the blood pressure (BP), electrocardiogram (ECG), and blood oxygen saturation (SpO2) of patients were monitored. Oxygen was administered via nasal cannula.
All patients were placed in an occiput posterior position with head turned to the opposite site. 25% Ropivacaine (PHR2571, Sigma-Aldrich, St Louis, MO) and 1% Lidocaine (PHR1034, Sigma-Aldrich) were selected as the local anesthetic. Sonosite S-Nerve portable ultrasound system (Soma Technology, Bloomfield, CT) was used as the ultrasonic apparatus, with the linear probe set at a high frequency of 6–13 MHz. The probe was placed horizontally in the middle of the sternocleidomastoid, and the sternocleidomastoid muscle could be seen in the center of the screen. Then, the posterior margin of the sternocleidomastoid muscle and the prevertebral fascia were searched and identified. After the point and angle of puncture were determined, the tip of the needle underwent in-plane adjustment to enter between the sternocleidomastoid muscle and the prevertebral fascia, close to the posterior edge of the sternocleidomastoid muscle. The superficial CPB was completed via injecting 5–6 mL of local anesthetic to separate the prevertebral fascia from the sternocleidomastoid muscle. By the rotation of the probe to the sagittal position and the connection of the outer edge of sternocleidomastoid muscle, the transverse processes on the 3rd, 4th, and 5th cervical vertebrae were observed, presenting a mark that resembles a hump. After the 4th cervical vertebrae was determined at the middle of the posterior edge on the sternocleidomastoid muscle, the probe was rotated by 90° horizontally, and the tip of the puncture needle was guided in the same plane between anterior and posterior nodules of the transverse process of the 4th cervical vertebrae. 4 mL of local anesthetic was injected to complete the deep CPB on the cervical plexus, after the confirmation that no blood and cerebrospinal fluid (CSF) were withdrawn by the puncture needle. The transverse process could be observed via the ultrasound localization, and the tip of the puncture needle was located above the transverse process and between the anterior and posterior nodules. The image of anesthetic diffusion was visible following the injection of local anesthetic, as depicted in Figure 1. Representative image of anesthetic diffusion after the injection of local anesthetic.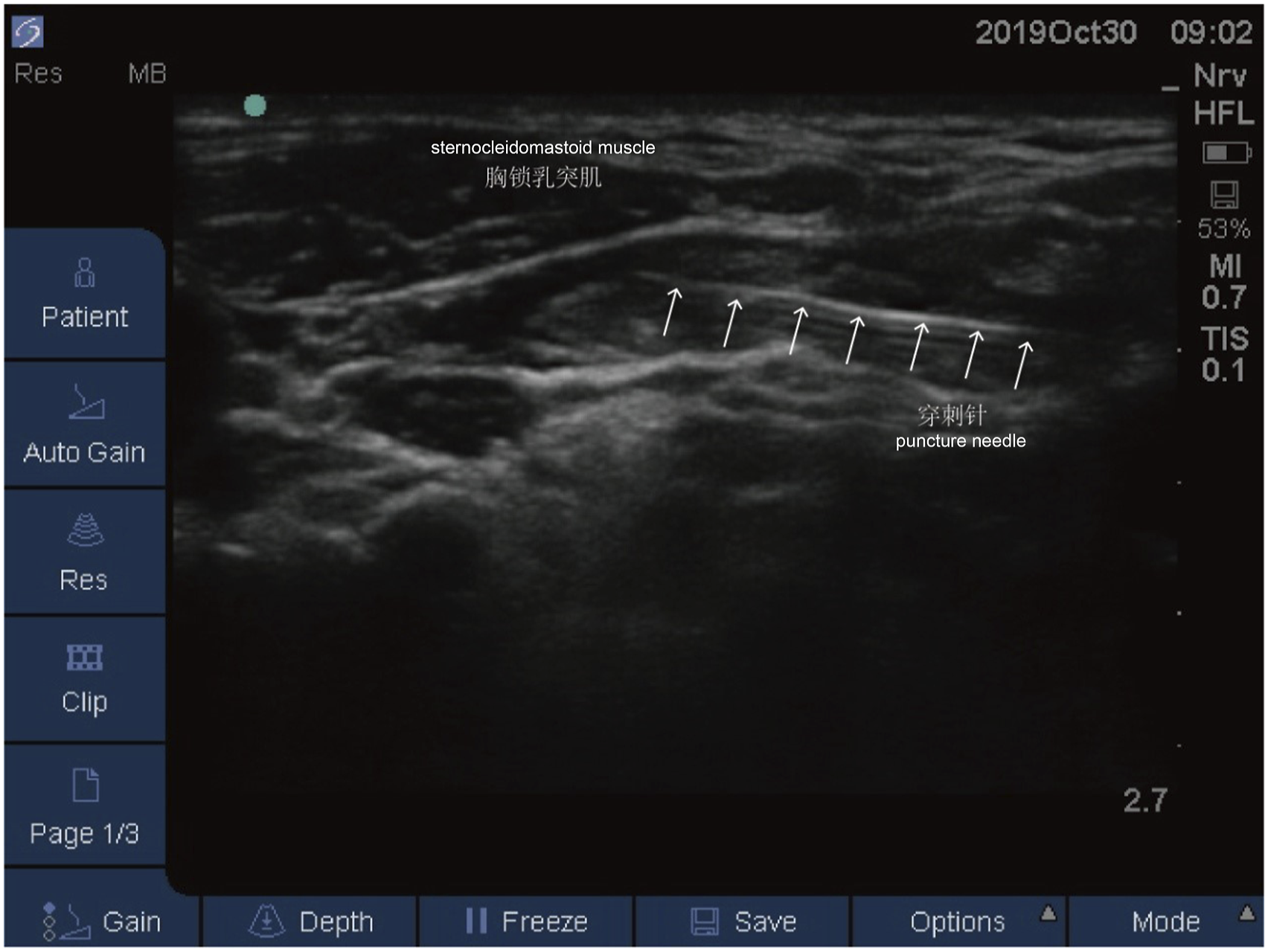
The surgical side was subjected to the deep and superficial CPBs, while the contralateral side only underwent the superficial CPB. The anesthetic effect was then tested via the acupuncture method, and the difference on the nociceptive sensation in the skins from the cervical plexus and anterior innervation was compared. The surgically disinfected towel was laid on the patients when the nerve block was determined to be effective. Dexmedetomidine (0.5 μg/kg, SML0956, Sigma-Aldrich) was administered as an adjuvant during the surgery for 10 minutes. Next, dexmedetomidine was intravenously pumped at a dosage of 0.1–0.5 μg/(kg*h) to ensure the patients in a moderately sedated and awake state for phonation during surgery.
Observational Indexes
The BP, ECG, heart rate (HR), and SpO2 of patients were recorded before anesthesia, 10 minutes post anesthesia, and at the time of the implantation of testing materials.
Statistical Analyses
All the statistical analyses in this study were performed with SPSS software (version 17.0, IBM Corporation, Armonk, NY). All data were expressed as mean ± standard deviation (SD). Statistical significance was determined using t test, which was defined when P-value was below 0.05.
Results
All patients underwent the surgery under the aforementioned anesthesia method without intraoperative assistance of infiltrate local anesthesia. No complications, like local anesthetic toxicity, and total spinal anesthesia were reported. 2 of 15 cases were given 5–10 μg of Sufentanil, and no Horner’s syndrome was found in patients after anesthesia.
Comparison on the blood pressure and heart rate in patients before, during and after anesthesia.

Note: 1 mm Hg = 0.133 kPa; *P < 0.05, vs. Before and after anesthesia.
Discussion
The vocal cords are the major vocal organs in the throat. The muscles, which are responsible for the movements of vocal cords, are mainly controlled by an inferior motor nerve and a branch of the vagus, named recurrent laryngeal nerve (RLN). The damage on RLN may result in the onset of VCP. 11 A variety of injuries can cause the palsy on RLN, like the trauma on the neck or chest, stroke, iatrogenic injury, sclerosis, infection, and tumor invasion or compression, among which the iatrogenic injury and tumor-induced damage to the RLN are suggested to be the culprit of UVCP. 12 As a fundamental otolaryngological clinical problem and a prevalent disorder resulting in the insufficiency of glottal closure, hoarseness, and aspiration during swallowing, UVCP continues to gain attention in terms of its notable impacts on voice, swallowing and even airway functions. 13 Traditionally, patients diagnosed with UVCP will undergo a period of voice therapy and “watchful waiting.” Accordingly, patients are expected to wait up to a year until the definitive treatment is provided, during which the function of their vocal cords is allowed to recover. However, many patients may suffer from difficulty in communicating and swallowing for up to a year, and may receive a permanent surgical treatment in the form of vocal cord medialization considering the inadequate improvement, which is constituted by either an injection under the general anesthesia or laryngeal framework surgery. 14 Currently, a combined procedure of type I thyroplasty under the local anesthesia has been proven as both an effective and reliable method and the gold standard approach for the treatment of UVCP, where a thyroid cartilage wedge is implanted contralaterally to the immobile vocal cord. 15 In the current study, 15 patients with UVCP were included, among which UVCP is the complication resulted from thyroid surgery (3 cases), radiotherapy for nasopharyngeal carcinoma (NPC) (1 case), pulmonary surgery (1 case), craniocerebral trauma (1 case), and unknown etiology (9 cases). All of the 15 patients with UVCP successfully received type I thyroid cartilage laryngoplasty and vocal cord medicalization surgery. The surgery was performed by opening cartilaginous window on the thyroid cartilage, determining the size of silastic implantation, and placing the implant through the cartilaginous window, so as to completely close the glottis and phonate well. These procedures are usually conducted under local anesthesia with the sedation, so that the voice can be monitored during the procedure. 16 Besides, due to the complex innervation and proximity of multiple anatomically important and delicate structures, the regional anesthesia on the nerves of the cervical plexus remains as a serious challenge for the anesthesiologists. 17
Ever since 2009, the combination of ultrasound-guided CPB and a periarterial local anesthetic infiltration has been widely performed, which has potential benefits in avoiding accidental vascular punctures and possibly reducing the dose of local anesthetic. 18 However, the neural innervation of regions around the neck is complicated, and the sympathetic trunk and cranial nerves are implicated in the innervation of both the arterial vessel wall and the sternocleidomastoid. Thus, it is necessary to administer additional intraoperative doses of local anesthetic and/or opioids/sedatives. In the current study, both deep and superficial CPBs were carried out on the surgical side, and only superficial CPB was also conducted on the contralateral side. The application of ultrasound-guided superficial/deep CPB ensures the spread of the local anesthetic into the designated area, which thereby increases the success rate, and prevents the local anesthetic from going too deep or penetrating the adjacent tissue. Notably, the superficial cervical plexus is unnecessary to be visible in order to complete the block, and meanwhile, the localization of the plexus is uncertain on the image. Therefore, in the current study, the puncture needle was inserted below the sternocleidomastoid muscle. The tip of the needle was inserted and adjusted directly between the sternocleidomastoid muscle and the prevertebral fascia, close to the posterior edge of the sternocleidomastoid muscle, so as to ensure that the local anesthetic was injected between the sternocleidomastoid muscle and the prevertebral fascia and allow sternocleidomastoid muscle and prevertebral fascia to be stratified.
A prior study has suggested that the addition of dexmedetomidine to ropivacaine can help improve CPB. Notably, dexmedetomidine is the most recent α2-adrenergic agonist introduced to clinical practice. Ropivacaine is a novel local anesthetic, possessing better safety profile in many aspects, like in the prolonged analgesia for the nerve block. 19 In the current study, intravenous dexmedetomidine pumping was successfully used to assist the painless sedation and ensure the patients to be awake for the phonation during surgery. For instance, with the accurate localization under ultrasound guidance, the anesthesia was successfully completed on a patient with limited neck movement and leathery stiffness of the soft tissue in the neck after the radiotherapy for NPC. Traditional blind CPBs require 10–15 mL of local anesthetic for unilateral anesthesia of superficial CPB and 5–6 mL of local anesthetic for deep CPB, for a total unilateral volume of 15–20 mL. However, under ultrasound guidance, the total volume of unilateral local anesthetic only needs 9–10 mL. Besides, the performance of ultrasound-guided CPB contributes to the accurate localization of local anesthesia and reduction of total amount of local anesthesia, further reducing the occurrence of its complications. In the current study, with the guidance of ultrasound, the thyroid cartilage laryngoplasty was conducted with both deep and superficial CPBs, and meanwhile dexmedetomidine was pumped intravenously, so as to keep the patients in a moderately sedated state where they were allowed to phonate during the surgery. In this study, the overall smooth anesthesia appeared in all patients and there was no significant difference in changes of HR, DBP, and MBP throughout the surgery with the exception of reduction in SBP.
In this study, to evaluate the ultrasound-guided CPB with the intravenous dexmedetomidine pumping, 15 patients with thyroid cartilage laryngoplasty are enrolled. The results demonstrate that ultrasound-guided CPB with the intravenous dexmedetomidine pumping is a safe anesthesia method for patients during thyroid cartilage laryngoplasty, where patients can cooperate to phonate under the sedation. Results from this study authenticate the efficacy of ultrasound-guided CPB with the intravenous dexmedetomidine pumping on type I thyroid cartilage laryngoplasty and vocal cord medialization surgery. It is hoped that these findings will be conducive to clinical needs for anesthesia in the future.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.