
Abstract
External nasal deformity is common and can be treated surgically. It often occurs in conjunction with the development of the nasal septal cartilage, vomer, and vertical plate of the ethmoid bone but may be caused by trauma. Here, we present a case of external nasal deformity caused by trauma. A woman presented with nasal obstruction due to dysfunction of the nasal valve area and was referred to our department for treatment. No chronic rhinosinusitis or nasal septal deviation that causes nasal obstruction was noted at the initial examination. However, trauma-related scarring was observed in the nasal valve area, and a Cottle test yielded positive results. The patient underwent combined rhino- and Z-plasty surgery and is currently undergoing follow-up at an outpatient clinic.
Although otolaryngologists generally use an endonasal approach to treat nasal obstruction, it is important to perform an appropriate evaluation of the external nose and to collaborate with a plastic surgeon, as necessary.
Introduction
The midline of the nasal cavity, the boundary between the left and right sides is composed of the nasal septum cartilage, vomer, vertical plate of the ethmoid bone, and nasal ridge of the maxillary bone. During the human growth process, elongation of the nasal septum cartilage and vomer often causes nasal septal deviation due to stress on the junction. Depending on the direction of cartilage growth, it may also cause external nasal deformity. Conversely, external nasal deformity and nasal septal deviation are sometimes associated with facial trauma, and proper treatment based on a three-dimensional view of the nasal cavity morphology is necessary to reduce functional nasal obstruction.
We report the rare case of a woman who required facial plastic surgery owing to trauma–related nasal obstruction and review the literature to highlight the favorable outcomes of open rhinoplasty and scar contracture repair with Z-plasty
Case Report
A woman was brought to the emergency department of our hospital after falling and hitting her face. She had an open wound in the nasal area, which was sutured at the same department (Figure 1A, 1B). Subsequently, the patient was referred to our department because she exhibited symptoms of nasal obstruction. The patient’s general condition was good and no significant findings (e.g., nasal discharge or nasal tumor) were observed during nasal endoscopy. There was no deviation of the nasal dorsum or depression of the nasal apex, and the sutured wound appeared clear without any signs of infection. However, the left nasal wing was deformed, and the external nostrils were collapsed (Figure 1C). Paranasal computed tomography (CT) revealed no evidence of rhinosinusitis or nasal septal deviation, whereas the Cottle test results were positive (Figure 1D). Resultantly, we diagnosed the patient with trauma-related anterior nasal valve dysfunction and decided to perform open rhinoplasty and scar contracure repair suing Z-plasty to expand the nasal valve, in cooperation with a plastic surgeon. (A) Trauma to the nasal valve area at initial emergency department visit. A large laceration was observed in the nasal valve area and it was nearly detached. (B) Facial findings after suturing in the emergency department. (C) Facial findings at the first visit to the otolaryngology department. There is no sign of infection in the wound; however, there is a depression along the wound. (D) Paranasal sinus CT findings. No obvious sinusitis or nasal septal deviation was detected.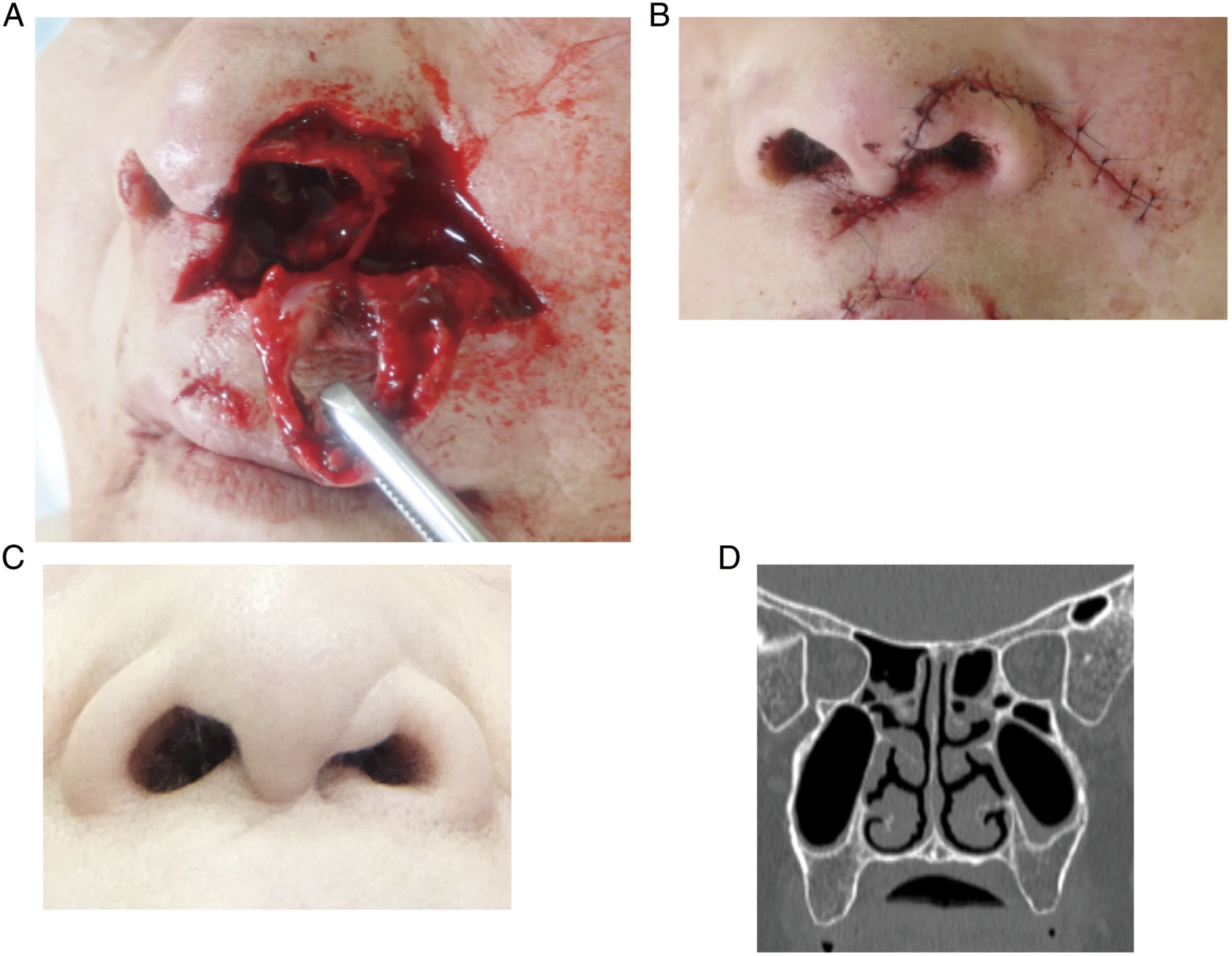
The plastic surgeon made an incision in the lateral nasal edge through the entrance of the right lateral nasal cavity, followed by reverse V-shaped incision at the front of the nasal pillar. On the left side, an incision was made along the previous surgical scar to identify the anterior margin of the nasal wing cartilage, along which the subcutaneous tissue was removed. The anterior edge of the nasal septal cartilage was identified, the bilateral nasal septal mucosa was separated under the cartilage membrane, and the posterior vertical version of the ethmoid bone was resected endoscopically. The posterior part of the nasal septum cartilage was removed as a graft, preserving the L-strut. The graft was divided into two parts and sutured bilateral to the L-strut to elevate the nasal apex. Additionally, Z-plasty was performed on the left nasal cavity entrance where scar contracture had occurred, and the bolster was fixed to the back of the nose. Surgery was completed with packing of the nasal canal (Figure 2A). The patient’s postoperative course was uneventful, and the bolster and packing were removed on the second day. She was discharged from the hospital on the eighth postoperative day. Her symptoms had completely subsided, and she was discharged from our department 3 months after the surgery (Figure 2B). (A) Intraoperative findings. The nasal septal cartilage was divided into two parts and sutured bilateral to the L-strut to elevate the nasal apex. (B) Postoperative facial findings. The wound is healing uneventfully.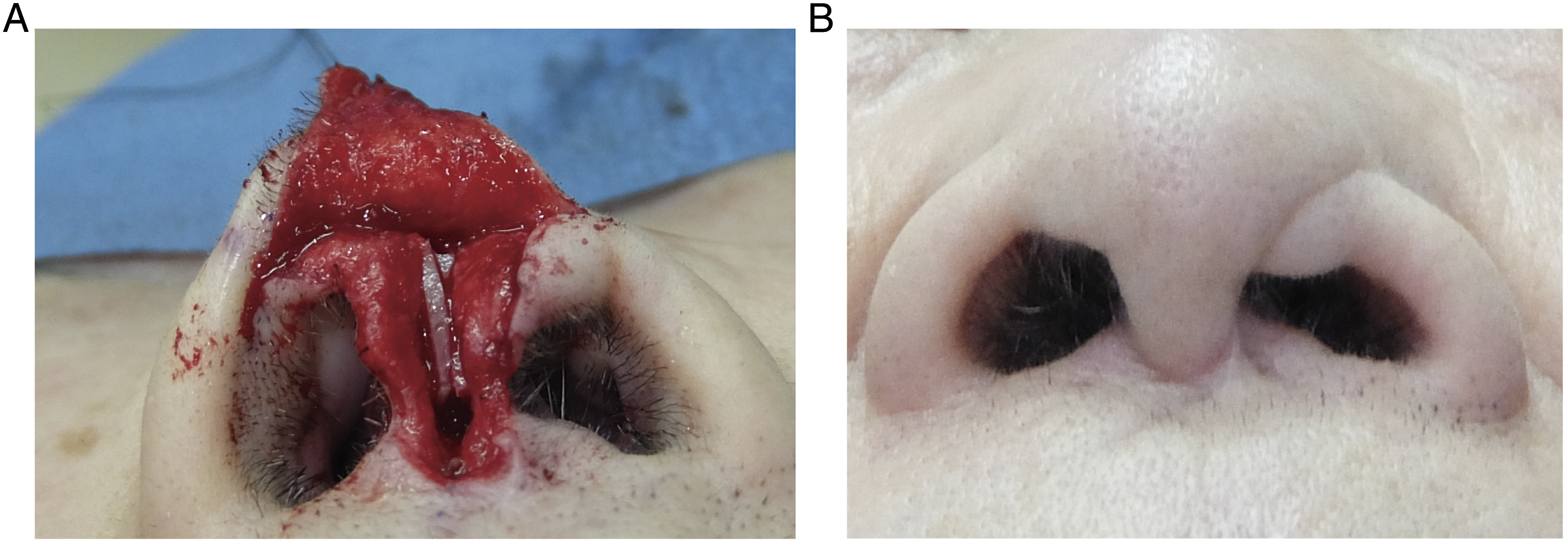
Discussion
In otorhinolaryngology, septoplasty and inferior turbinate surgery are commonly performed to reduce nasal obstruction, mainly via the nasal approach. However, nasal components include structures such as the lateral nasal cartilage, nasal bones, and nasal wing cartilages, as well as the nasal septum and inferior turbinate. Even when these are affected, nasal obstruction may occur. Particular attention should be paid to external nasal abnormalities, as failure to select an appropriate technique may result in inadequate therapeutic effects.1,2 For external nasal deformity, open rhinoplasty is generally performed via an incision in the nasal bridge, and various grafts are used to correct the shape of the nose depending on the degree of deformity.3-6
In the present case, the patient had significant nasal obstruction. In contrast, nasal deviation was mild; therefore, we initially attributed the nasal obstruction to nasal valve dysfunction. A spreader graft can be used to correct severe deviation of the nasal dorsum and a batten graft can be used to correct severe deviation of the anterior edge of the nasal septum. In this case, the nasal dorsum and the anterior edge of the nasal septum exhibited almost no deviation; hence, we did not use these grafts. Since the patient exhibited severe narrowing of the nasal valve area, we attempted to further improve the airflow by elevating the nasal plug area with nasal septum cartilage during the open rhinoplasty combined with Z-plasty in the scar area. Z-plasty is effective in extending the distance between two points and is a useful technique when scar contractures and depressed deformities are present.7,8 Previous reports have suggested the usefulness of Z-plasty for nasal valve stenosis; moreover, in the current case, nasal valve stenosis was improved by open rhinoplasty combined with Z-plasty because of the heavy scarring and significant deformation of the nasal valve area.9,10 Although otolaryngologists are unfamiliar with Z-plasty, this procedure is performed routinely by plastic surgeons, and cooperation between otolaryngologists and plastic surgeons is important in open rhinoplasty.
In conclusion, we encountered a patient with symptoms of nasal obstruction associated with traumatic external nasal deformity. It is important to examine the cause of nasal obstruction symptoms from a three-dimensional view of the nasal cavity and perform surgical treatment in collaboration with a plastic surgeon, if necessary.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Statement of Human and Animal Rights
This article does not contain any studies involving human or animal subjects.
Statement of Informed Consent
Informed consent was obtained from the patient for their anonymized information to be published in this article.