
Abstract
Comorbidities are common with craniofacial anomalies and can include auditory neuropathy spectrum disorder (ANSD). Identification of these comorbidities, such as a diagnosis of ANSD, has increased with expanded multi-disciplinary care teams and the use of auditory objective measures. Patients with craniofacial anomalies often have complex medical histories including extreme prematurity and jaundice, which may lead to the development of additional comorbidities. The 5-year-old boy that is the subject of this case study presented with noted developmental delays and residing in foster care with an unknown family/medical history. Initially presenting with middle ear dysfunction, exacerbated by craniofacial anomalies, the underlying cause of his speech delays was missed. Behavioral audiometry was attempted with inaccurate results. Surgery was performed to correct the craniofacial anomalies, middle ear dysfunction, and was followed with auditory brainstem response (ABR) testing. The boy healed well without complications. The ABR revealed ANSD, hearing aids were fitted for the diagnosis, regular speech therapy was initiated, and the boy continues to make steady progress toward developmental milestones. The purpose of this case study was to highlight the course of identification and treatment of a complex case that may provide insight into determining a differential diagnosis of ANSD when initially obscured by craniofacial anomalies.
Keywords
Introduction
The development of multi-disciplinary care teams has led to a more thorough and efficient treatment of children with craniofacial-related disorders. The addition of audiologists to these teams has given new insight and more comprehensive care for patients with hearing and balance disorders. Underlying conditions, such as auditory neuropathy spectrum disorder (ANSD), can be hidden by the presence of visually observable disorders like craniofacial anomalies. The objective of this case study was to highlight the course of identification and treatment of a complex case that may provide insight into determining a differential diagnosis of ANSD when initially masked by craniofacial anomalies.
Several studies have examined the prevalence of hearing-related disorders in children with cleft lip and/or palate.1,2 Broen et al. [1996] evaluated the hearing histories of 28 children with and 29 without cleft palate. The children were administered a hearing screening at 0.5, 1, and 2 kHz using visual reinforcement audiometry. Normal-hearing criteria at those frequencies were 30 dB HL at 9 months, 25 dB HL at 12 months, and 20 dB HL for each subsequent test. Middle ear status was also evaluated by tympanometry using a 226 Hz probe tone. These two procedures were measured from 9 to 30 months of age at 3-month intervals. Although all of the children showed abnormal middle ear status at some point from 9–12 months, those with cleft-related craniofacial issues had some degree of conductive hearing loss (CHL) for the remaining evaluations. They concluded that not only was middle ear dysfunction more common in children with cleft lip and/or palate but they should also receive pressure equalization (PE) tubes earlier.
There are several common birth defects that present with some form of craniofacial component. During the years from 2004 to 2006, the Centers for Disease Control (CDC) reported there were 7,088 cases of children born with a cleft lip, palate, or both annually. 2 This type of craniofacial anomaly is one of the most common birth defects that occur in the United States. While all causes of these anomalies are unknown, most result from genetic factors. This same study also noted 6,037 reported cases of Trisomy 21 (Down syndrome) during the same time period. Down syndrome, which most commonly is known for cognitive delays, also presents with frequent CHL. 3
Birth defects and associated risk factors can also lead to conditions such as ANSD. Patients admitted to the neonatal intensive care unit (NICU) may often have medically-related risk factors for ANSD. These risk factors may include but are not limited to prematurity, hyperbilirubinemia, meningitis, ototoxic antibiotics, low birth weight, respiratory distress, and mechanical ventilation. 4 Any of these factors or a combination thereof may lead to ANSD, which stems from a disruption in the synapse between inner hair cells and afferent auditory neurons or a dys-synchrony of electrical impulses transmitted anywhere along the auditory pathway from the auditory nerve to the brain.
Many papers have been published on the diagnostic criteria for ANSD.5–7 Berlin et al. (2010) evaluated 260 children and detailed common criteria to diagnose ANSD. These criteria are based on a combination of test results that include the cochlear microphonic (CM), auditory brainstem response (ABR), otoacoustic emissions (OAEs), and/or middle ear muscle reflexes (MEMRs). Each of these factors alone cannot definitively diagnose ANSD. The CM is a product of polarity-sensitive electrical activity originating from both outer and inner hair cells. 8 The presence of a CM during ABR testing indicates dys-synchrony of the auditory signal en route for interpretation by the brain. Measurable OAEs indicate normal cochlear outer hair cell (OHC) function, but require a normally functioning middle ear in order to measure them. It is important to note that OAEs are not a hearing test but an objective measure of OHC functionality and may be absent in 50% of cases of patients with ANSD. 9 Middle ear muscle reflexes (MEMRs) are efferent reflexes triggered by loud intensity stimuli and are controlled by landmarks of the auditory pathway including inner hair cells (IHC), the auditory nerve, and the brainstem. These reflexes may be absent if any of the landmarks in that auditory pathway are damaged. 10 MEMRs are typically absent in patients with ANSD and may be used as a “cross-check” for diagnosis. However, it should be noted that MEMRs are also typically absent with the presence of middle ear dysfunction. Diagnostic criteria for ANSD included (1) the presence of a CM or OAEs (measures of cochlear function) and (2) the absence of an ABR, abnormal ABR morphology, or the absence of middle ear muscle reflexes (MEMRs) (measures of auditory neural function).
This case study examines the multi-disciplinary evaluation of a young boy that presented with complications related to craniofacial/cleft palate, including nasal columella deformity (secondary to repaired cleft lip/palate) and food aspiration resulting from unsuccessful palate repair. With symptoms related to conductive hearing loss (CHL) that are typically present in children with craniofacial anomalies, underlying conditions such as ANSD may go undiagnosed. Additional audiological testing may be required to make this diagnosis. This testing may be further complicated by the presence of middle ear dysfunction. The overall goal of this case study is to provide insight regarding a differential diagnosis for clinical audiologists, so that conditions such as ANSD may be discovered if hidden by other observable anomalies.
Case study
The subject of this case study was a 5-year-old boy who initially presented with unknown birth history because he was a ward of the state residing in foster care. His foster parent signed informed consent allowing for this case study to be published. Child Protective Services took custody of the boy at the age of 5 years due to physical abuse and parental drug abuse. Accurate medical history could not be obtained, and newborn hearing screening outcomes were not known. At the initial visit, the boy expressed no complaints or pain. The caregiver was given a referral by the boy’s primary care physician to see the craniofacial/cleft team to follow up on his first cleft palate surgery. Each member of the multi-disciplinary team examined the boy, including plastic surgery, genetics, speech-language pathology, audiology, otolaryngology, and orthodontics.
Orthodontics reported that all teeth were in proper alignment and there were no dental abnormalities. Genetics found no evidence of comorbidities but would conduct blood testing. Speech-language pathologists noted significant delays in language development milestones. The foster guardian expressed concerns with progress in his kindergarten classroom noted by the boy’s teacher. He often appeared confused when given directions and rarely expressed verbal understanding. The child possessed a limited vocabulary for his age and had difficulty understanding simple verbal instructions. Speech therapy would be initiated twice weekly moving forward. Plastic surgery found evidence of previous bilateral cleft lip and palate repair as well as a flattened nasal bridge and shortened columella. The child’s foster mother reported that he frequently had issues with leaking from his nose, and the surgeon discovered an opening in the previous cleft palate repair. Recommendations were made to repair the opening in the cleft palate and extend the columella to correct the flattened nose anomaly.
Initial audiology evaluation involved extensive testing, which was an established test battery protocol for all patients examined for the craniofacial clinic and included:
Otoscopy and Tympanometry: Otoscopy revealed the presence of middle ear effusion bilaterally. A Grason-Stadler Inc. (GSI) Tympstar was used to measure middle ear status using a 226 Hz probe tone. Testing in the left ear indicated that the ear canal volume, peak pressure, and tympanic membrane (TM) mobility were within normal limits. Right ear measurements indicated normal ear canal volume but no TM mobility or tympanic peak pressure. This finding is consistent with otitis media with effusion (OME).
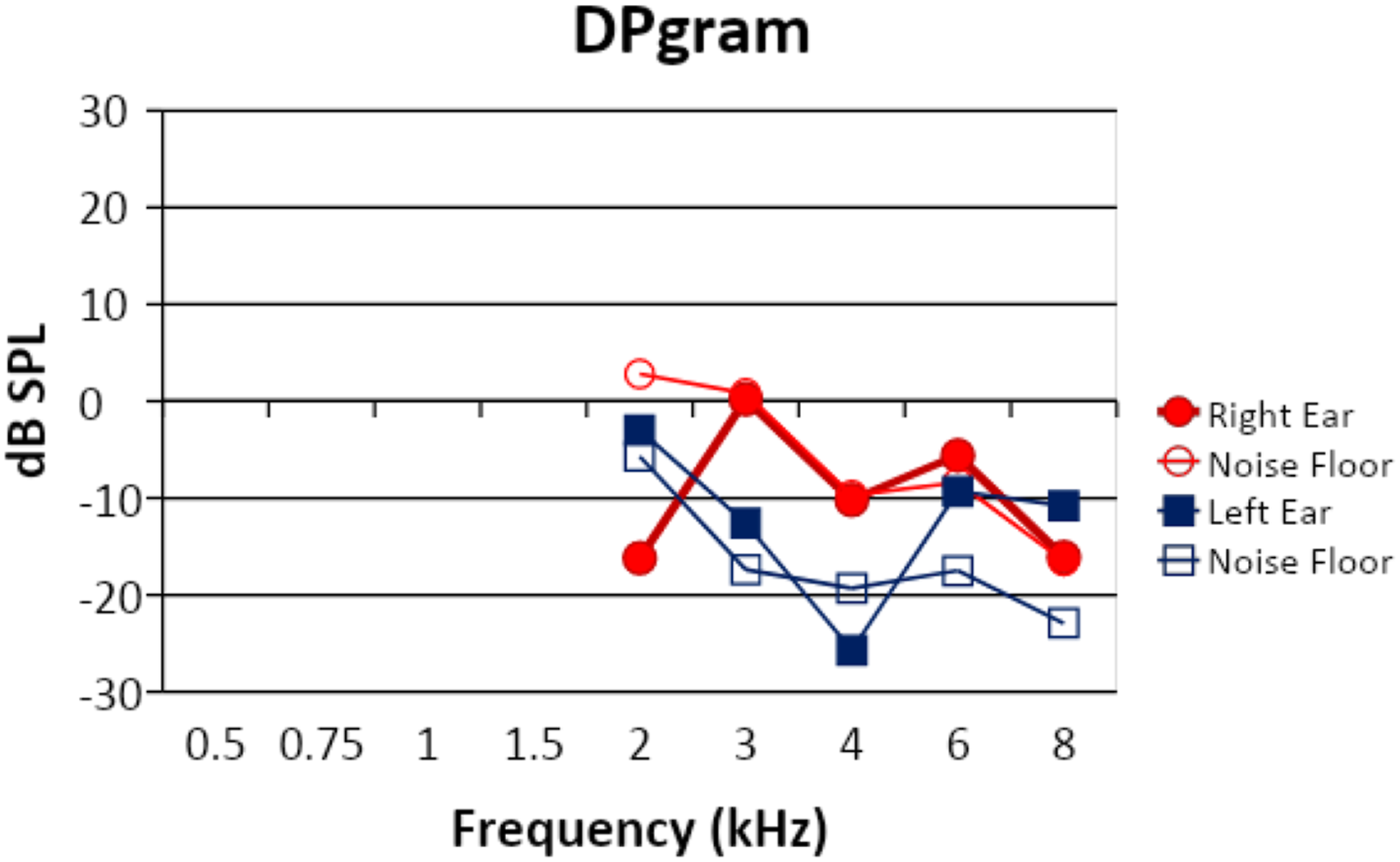
Otoacoustic Emissions: Distortion product otoacoustic emissions (DPOAEs), an objective measure of cochlear OHC function, were measured across the frequencies of 2 kHz–8 kHz bilaterally. Abnormal tympanometry may contraindicate the measurement of DPOAEs in the right ear. However, the auditory protocol from the craniofacial/cleft team required all testing to be performed bilaterally. Results are shown in Figure 1. The open circles indicate the noise floor detected in the right during testing and the filled circles are the measured responses. The open and closed squares indicate the same for the responses and noise floor measured in the left ear. The patient was tolerant and quiet for the procedure. DPOAE responses were absent at all frequencies bilaterally. The absent response of the right ear is expected as the sound used to measure the response may not properly travel through the auditory pathway with the inadequate movement of the tympanic membrane and possible OME as found with tympanometry. Normal tympanometry and absent DPOAE responses in the left ear may indicate the presence of a hearing loss.
Ipsilateral Middle Ear Muscle Reflexes: MEMRs, an objective measure for sensation level and to evaluate proper function of the auditory pathway, were tested at frequencies of 0.5, 1, 2, and 4 kHz bilaterally. Abnormal tympanometry contraindicates the effectiveness of measuring MEMRs in the right ear. However, auditory protocol from the craniofacial/cleft team required all testing to be performed bilaterally. Reflex thresholds were attempted from 80 dB to a maximum stimulation level of 105 dB. All measurements were absent bilaterally at all tested levels and frequencies.
Speech Reception Thresholds and Word Recognition: Speech testing was attempted with a point to picture task using ER-3A insert headphones and monitored live voice. No results could be obtained. To verify this lack of findings and as a result of the middle ear issues, the transducer was changed to TDH-39 headphones and repeated. Again, speech reception thresholds were attempted using pediatric spondees (e.g., ice cream, hotdog, and airplane) with a finger-pointing method. Thresholds were obtained at 25 dB HL in the right ear and 10 dB HL in the left with fair reliability. Word recognition was attempted utilizing the Word Intelligibility by Picture Identification test, which is designed for children typically 5–8 years old. The child was unable to condition or complete the task.
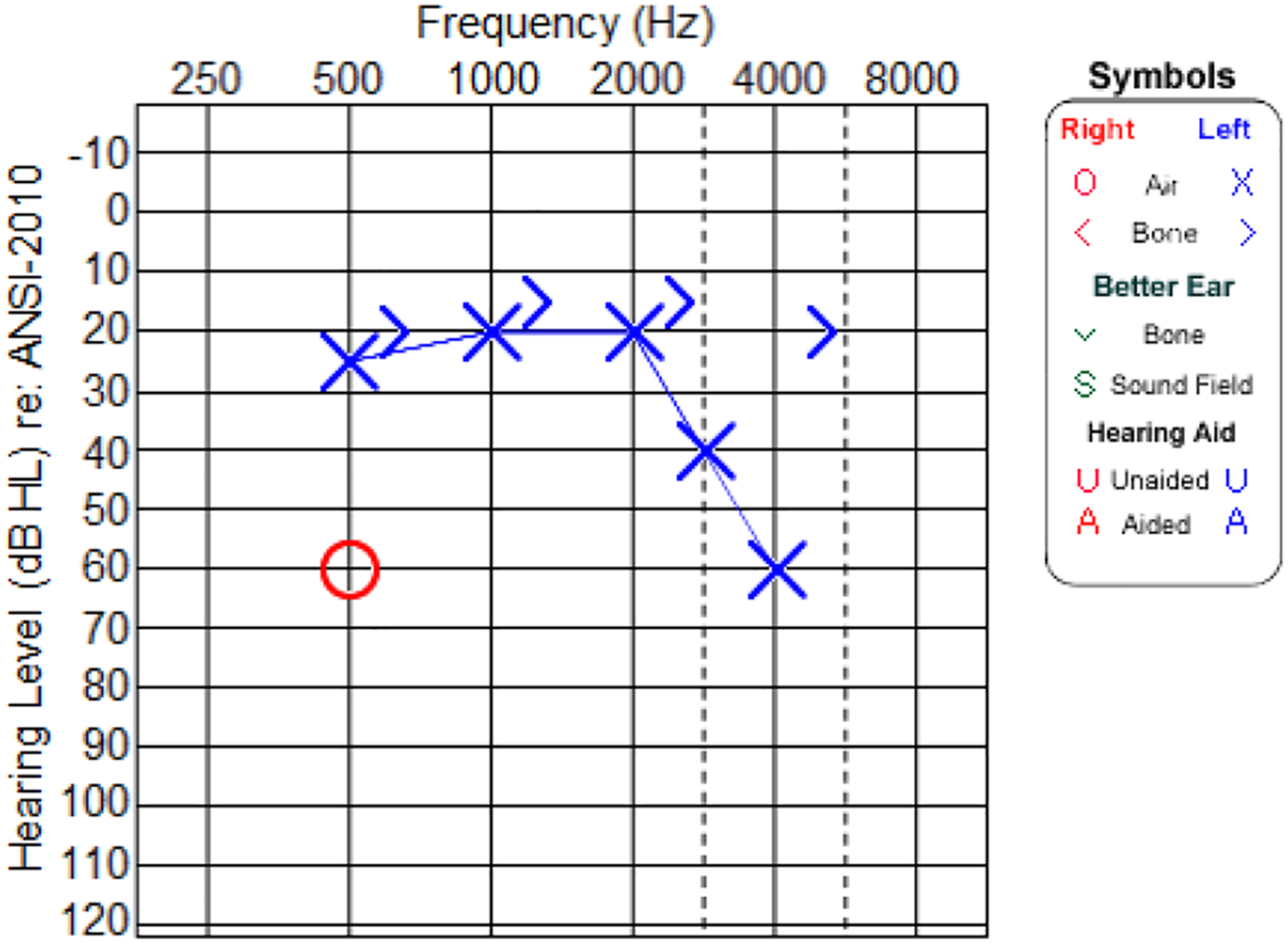
Audiometric Behavioral Testing: Conditioned play audiometry (CPA) was used with TDH-39 headphones and age appropriate for the child. This method involves conditioning the child to performing an action with a toy at the onset of an auditory stimulus. Stimuli including warble tones, narrow-band noise, and pulsed pure tones were attempted. As children may lose interest in the task, alternating stimuli may keep them further engaged. Figure 2 shows the audiogram obtained with behavioral testing. The results obtained indicated a mostly mild to moderately severe sensorineural hearing loss with the exception of a conductive component at 4 kHz in the left ear. Only a single response at 500 Hz was obtained in the right ear at the moderately severe hearing loss range. Bone-conduction thresholds were unable to be obtained for this ear to determine type of hearing loss. However, the indicated thresholds obtained occurred after numerous attempts of presented stimuli and unrepeatable responses. Therefore, it should be noted that reliability was poor. The poor reliability of the test results left the hearing status of the patient to be unknown. Results from DPOAE testing. The open circles indicate the noise floor detected in the right ear during testing and the filled circles are the measured responses. The open and closed squares indicate the same for the responses and noise floor measured in the left ear. The audiogram from the initial audiology visit with the craniofacial team. Symbol legend is included in the figure. Left (X) and right ear (O) thresholds are indicated on the audiogram. Unmasked bone conduction thresholds (>) are also indicated. Measures were attempted with ER-3A insert headphone transducers. The limited behavioral data was obtained with poor reliability and was unable to be repeated.
To determine the hearing levels for each ear, the patient was scheduled for a sedated ABR. This test was to be done intraoperatively during a single surgery for craniofacial anomalies and myringotomy for pressure equalization (PE) tube placement. Prior to the placement of PE tubes, incisions were made in the tympanic membranes to assess middle ear status and a thick, purulent fluid was removed via suction. If the fluid is not removed prior to the ABR, the conductive component can impact results both by determining thresholds and lead to extended latencies across waveform morphology. Surgery began with a revision of the previous repair of the bilateral cleft palate. The shortened columella was then cut and a full rhinoplasty was performed to correct the flattened nasal bridge anomaly. A cartilage graft was harvested from the concha of the right ear and used to extend the nasal columella.
Cerumen was removed prior to a myringotomy. After incision of each TM, suction was required to remove a thick, purulent fluid from the middle ear cavity of both ears. Pressure equalization (PE) tubes were placed in the incision of each TM. Suction continued until the remaining discharge was removed from the middle ear cavity. No other complications were noted. Surgery was successful without complications.
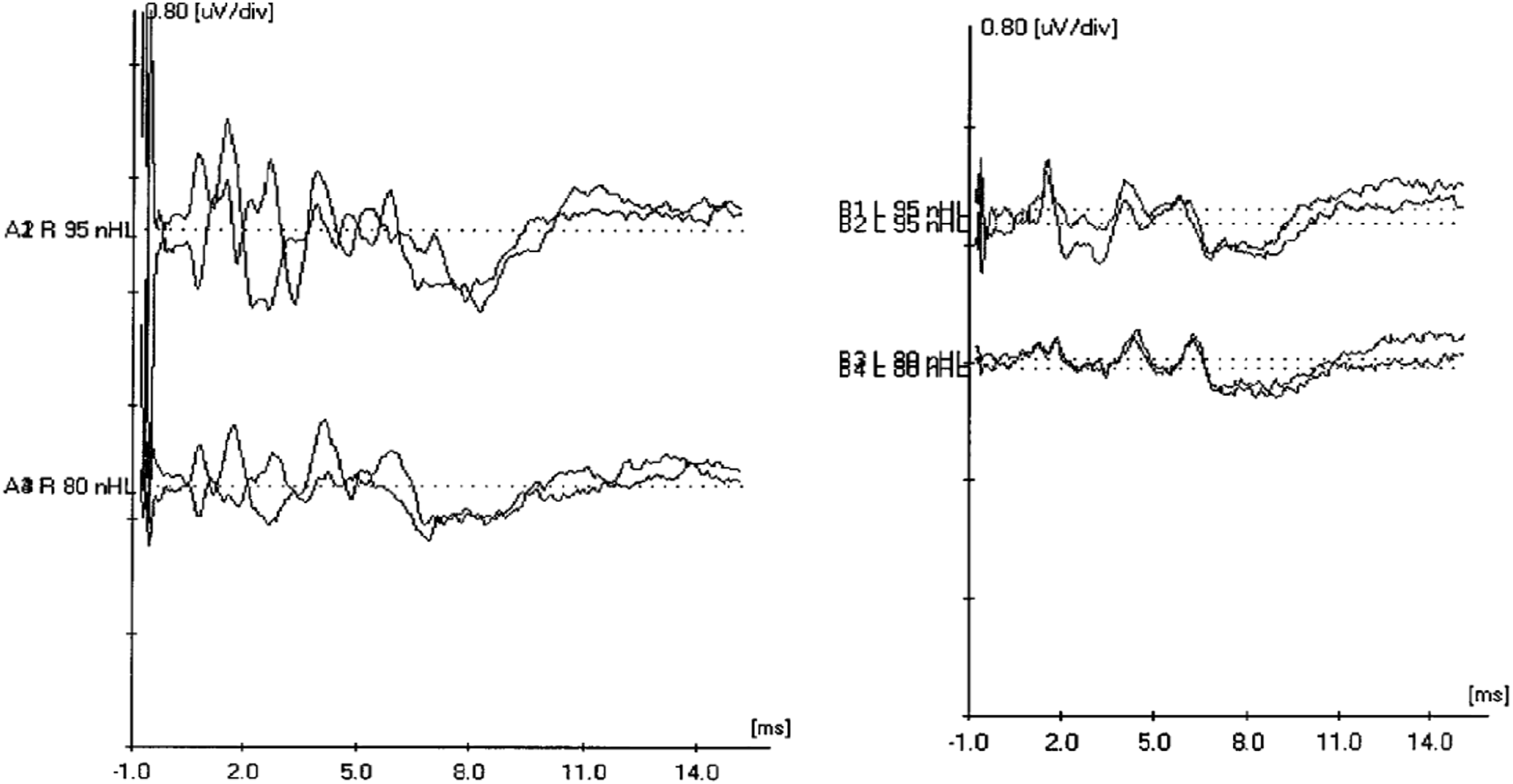
Intraoperative Auditory Brainstem Response: ABR testing was conducted following bilateral PE tube placement. ER-3A insert headphones were used to present stimuli. Waveforms were recorded with a single channel using a Cz, M1, and M2 electrode montage. A high-intensity click was presented to determine morphology, synchrony, and interpeak-latency to evaluate the integrity of the auditory pathway. These waveforms are depicted in Figure 3. Waveform morphology of the left ear depicts normal neural synchrony. Results in the right ear indicated abnormal waveform morphology with the presence of a CM. If a CM is discovered during an ABR, it needs to be repeatable and confirmed prior to documentation. This was done by performing high-intensity click runs using both rarefaction and condensation starting at 95 dBnHL and decreasing intensity in subsequent trials. The CM remained after this process. A control run, which involved clamping the insert headphone tubing, was also performed to rule out transducer or stimulus artifact. No waveforms, interference, or artifact was present during the control run. Due to the present CM during measurements and not visible during the control runs, the results of the ABR indicated ANSD in the right ear. Initial click waveforms from intraoperative auditory brainstem response (ABR) testing indicating morphology are shown. Results from the left ear and right ear are displayed on the left and right side of the figure, respectively. Click ABR waveform morphology for right and left ears respectfully.
Earmold impressions were taken following surgery and testing. Behind the ear style hearing aids were fitted and set to desired sensation level (DSL) targets bilaterally. The boy demonstrated consistent behavioral responses to Ling sounds ([m], [ah], [oo], [ee], [sh], and [s]). An individualized education plan (IEP) was established and a frequency-modulation (FM) system was purchased by his school to help with milestone development. An FM system is an assistive listening device that allows direct streaming from a speaker to a CI or hearing aid user. This stream allows for aided comprehension of speech in noisy and reverberant environments.
Discussion
The overall goal of this case study was to demonstrate how additional diagnostic information can uncover unsuspected conditions, such as ANSD, that may be hidden by more visually apparent disorders, such as craniofacial/cleft anomalies. After being granted custody, the foster parent believed the child was withdrawn and silent as a result of his prior abusive home life. Chronic OME delayed the diagnosis of ANSD and a trial with hearing amplification. Following initial hearing aid fitting, an IEP was put into place and educational services were started at his school. Teachers and caregivers reported steady improvements in delayed developmental milestones. 11
Regular speech therapy has greatly improved the child’s vocabulary and speech production over a period of three years. The child has shown substantial improvement in receptive language skills through the ability to demonstrate an understanding of complex instructions. Expressive language skills have also improved from a previous total spoken vocabulary of five words to over 200 words. This improvement in vocabulary was due to the consistent use of amplification, speech therapy, and peer interaction.
A hearing amplification trial is a common audiological treatment for ANSD, but standards for hearing aid programming targets (based on the patient’s hearing loss) have yet to be established. Audiometric behavioral thresholds do not necessarily always correspond to the levels that patients with ANSD are actually hearing. 12 A “conservative” approach has traditionally been used to estimate target amplification levels. A study by He et al. (2013) used evoked potentials by ABR to objectively estimate the hearing thresholds of children with ANSD using frequencies ranging from 250–4000 Hz9. The results of the study indicate a range of thresholds for each tested frequency but needed further subject trials to better determine the error in found threshold ranges. A “conservative” approach has traditionally been used to estimate target amplification levels as no definitive research has emerged. As a result, a low 10dB was added across all frequencies when programming the patient’s hearing aids.
Hearing aids are not the only option for treating a patient with ANSD. Following an amplification trial, some children still may not be meeting their developmental milestones. A retrospective study by Brenaman et al. (2012) compared outcomes for children diagnosed with ANSD who received a CI to outcomes for children with SNHL fitted with hearing amplification. Speech-recognition scores between the two groups showed no significant differences. They concluded that barring evidence of cochlear nerve deficiency, cochlear implantation was a viable option to treat children diagnosed with ANSD.
Ipsilateral MEMRs and OAEs can be useful tools for diagnosing ANSD. However, the frequency of middle-ear dysfunction in children can prevent these tests from producing measurable results. Nwokoye et al. (2015) found in a study of 212 children with no other comorbidity that 61.3% of participants were diagnosed with otitis media. 13 The occurrence is even higher with children with cleft palate. Dhillon (1988) found that 97% of 100 examined ears were diagnosed with OME prior to cleft palate closure. 14 As the efficacy of ipsilateral MEMRs and OAEs are dependent on a clear auditory pathway, the abnormal status of the middle ear may obscure testing required to determine auditory neuropathy.
A multi-disciplinary approach can be instrumental in providing a differential diagnosis of patients with craniofacial issues to determine the presence of comorbidity. Numerous diagnostic tests may aid in the identification of ANSD. After the condition is identified, many treatment options are available. The subject of this case study continues to make steady progress with his hearing, language, and educational milestones. Three years following his initial diagnosis and fitting of binaural hearing aids, he has become more social at school and teachers report an expanded vocabulary.
Footnotes
Acknowledgments
The content of this case study is solely the authors’ responsibility and does not necessarily reflect the official view of the University of Chicago Medicine. The authors wish to think the Craniofacial/Cleft Team at the University of Chicago Medicine; Russell Reid, MD for plastic surgery services, Darrel Waggoner, MD for genetics evaluations, Michael Stosich, DMD for orthodontics consultations, Brandon Chiu, MD for otolaryngology intervention, and Michelle Hughes, PhD for providing feedback on earlier drafts of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Written consent was obtained from the legal guardian of the subject of this case study who allowed for its submission.
Data availability
The data supporting this case study are available from the corresponding author, JDS, upon request.