
Abstract
Introduction
Despite the presence of a growing body of literature suggesting cost-ineffectiveness of routine pathologic analysis of tonsillectomy specimens, little is known about common institutional policies and practice patterns of pediatric otolaryngologists. The objectives of this study were to determine the prevalence of routine pathological evaluation of tonsillectomy specimens for uncomplicated pediatric adenotonsillectomy procedures and to evaluate opinions regarding this controversy among board-certified pediatric otolaryngologists.
Methods
This was a cross-sectional survey study sent to board-certified pediatric otolaryngologists currently practicing and registered with the American Society of Pediatric Otolaryngology (ASPO) assessing their institutions’ or practices’ current policies on sending routine tonsillectomy specimens for pathology, their experience with this practice, and their opinions on whether routine pathologic analysis should be employed. Basic statistical analysis was then conducted.
Results
Respondents mostly practiced in an academic setting (68.4%), with the next most common being academically affiliated private practice (21.8%), and private practice was the least common (9.8%). Most respondents (85.1%) did not agree with routine pathologic analysis of otherwise uncomplicated pediatric tonsillectomy specimens.
Conclusion
Most pediatric otolaryngologists who responded to this survey do not support routine pathological analysis of otherwise uncomplicated pediatric tonsillectomy specimens. However, the results are likely biased and should be interpreted carefully, since only a small percentage of pediatric otolaryngologists responded to the survey. Potential cost savings could be seen by patients, payers, and hospital systems with judicious use of surgical pathology, specifically in cases with concurrent signs or symptoms suspicious for malignancy.
Keywords
Introduction
Tonsillectomy is the second most common surgery performed in pediatric patients with hundreds of thousands of procedures being performed each year. 1,2 The indications for tonsillectomy in children are overwhelmingly for benign causes with the two most common reasons being obstructive sleep apnea and recurrent tonsillitis. 2 Given that these are the two most common indications, the utility of routine pathologic examination of tonsil tissue after tonsillectomy has been in question for some time. It has been estimated that foregoing the routine pathologic analysis of tonsil specimens could result in an annual savings of approximately 35 million dollars in the United States. 1 The massive potential savings to the healthcare system coupled with the lack of valuable information provided by routine gross or microscopic pathologic examination of tonsil tissue makes this an important and interesting topic to consider.
For the practicing otolaryngologist, pragmatism with the use of both healthcare dollars and resources are of utmost importance. Elimination of potentially unnecessary interventions not only lowers the economic healthcare burden but also could increase patient satisfaction due to improved clinical efficiency. 3 In addition, elimination of unnecessary interventions improves overall healthcare efficiency, which has been shown to be correlated to reduction in complications and overall positive patient outcomes. 4 For the practicing otolaryngologist, optimization of these factors and maximization of patient satisfaction are critical components to the patient experience. Although the choice of whether to send routine tonsillectomy specimens to pathology might not directly impact surgeons, this choice can have important consequences that include the cost to the patient and thus patient satisfaction, time, and cost incurred by the pathologist and/or pathology technicians, and ultimately the healthcare efficiency of their respective institutions.
Despite significant evidence indicating cost-ineffectiveness of routine pathologic analysis of tonsillectomy specimens, 5 -8 little is known about current practice patterns, opinions, and national trends among pediatric otolaryngologists surrounding the matter. Moreover, the presence of institutional policies regarding routine pathologic analysis of pediatric tonsil specimens at various institutions and practices has not previously been reported. There have been several studies that have retrospectively investigated the trends in utilization of pathologic analysis after tonsillectomy and the outcomes of these analyses. 1,2,5,6,9,10 However, no study to date has described the practice patterns and attitudes regarding routine pathologic analysis of tonsil tissue among board-certified pediatric otolaryngologists. To understand this issue more completely, it is important to understand the opinions of surgeons who perform these procedures and interpret these results regularly. In this study, we performed a cross-sectional survey of board-certified pediatric otolaryngologists in the United States to assess the attitudes, practice patterns, and experiences of both individual physicians and their institutions.
Materials and Methods
Depiction of the Ten-Item Questionnaire Along With Accompanying Summary of Responses by Question. in Total, 134 Pediatric Otolaryngologists Out of 657 (20.4%) Responded to the Survey.
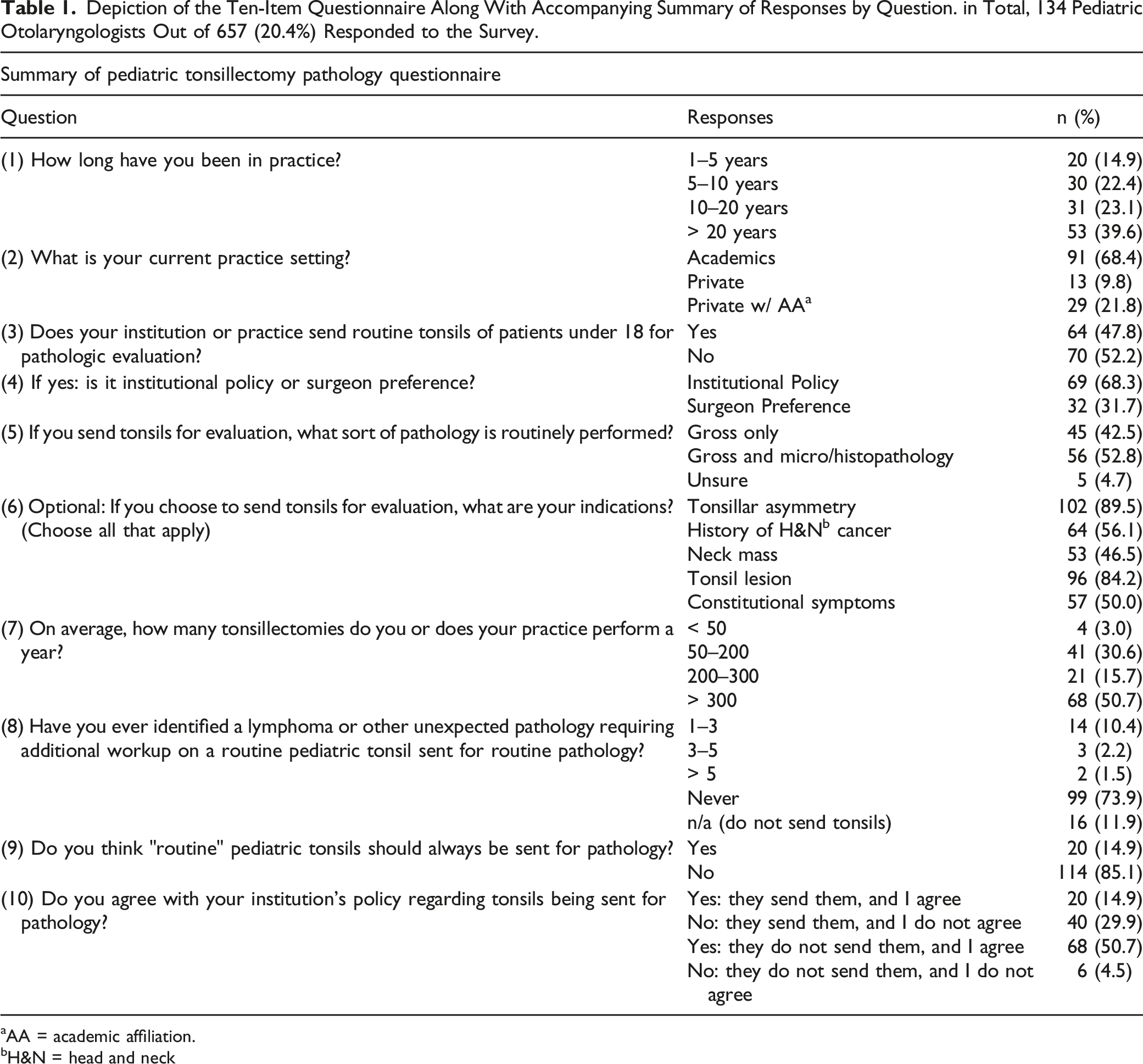
aAA = academic affiliation.
bH&N = head and neck
After approval was obtained from ASPO’s Research committee, the survey was sent via a single email to all current practicing ASPO members, which were 657 members at the time of the study. The email contained a short cover letter indicating a description of the study followed by a link. Respondents were required to enter their ASPO-associated email address to complete the survey, which could only be completed once per email address to eliminate the possibility of duplicate responses. The survey was left open to collect responses from January 1, 2021, through October 1, 2021. No follow-up emails were sent. When the designated period had elapsed, responses were downloaded to Microsoft Excel (Microsoft Corporation, Redmond, WA) for further analysis and subdivision. Basic statistical analysis was then conducted.
In addition to the survey component, additional data regarding reimbursement rates was queried from the Centers for Medicare & Medicaid Services (CMS) by Current Procedure Terminology (CPT) codes for both gross and microscopic evaluation of tonsillectomy. We downloaded the 2022 Medicare reimbursement rates (U.S. Department of Health and Human Services, Centers for Medicare & Medicaid Services, 2022 Reimbursement Schedule) for CPT code 88300, used for gross-only pathologic examination of the tonsils, and CPT code 88304 for both gross and microscopic pathologic examination of the tonsils.
Results
At the conclusion of the study, 134 responses were received out of the 657 total ASPO members (Table 1). Response rate was 20.4%. These data were further subcategorized below.
Practice Information
Most respondents were academic-based (68.4%), with 21.8% having an academically affiliated private practice; only 9.8% were purely private practice-based (Figure 1). There was a wide variation in experience, but overall, the respondent group represented a highly experienced population, with 62.7% of respondents having at least 10 years of experience and 39.6% with 20 years of experience. Only 14.9% of respondents had less than 5 years of experience.
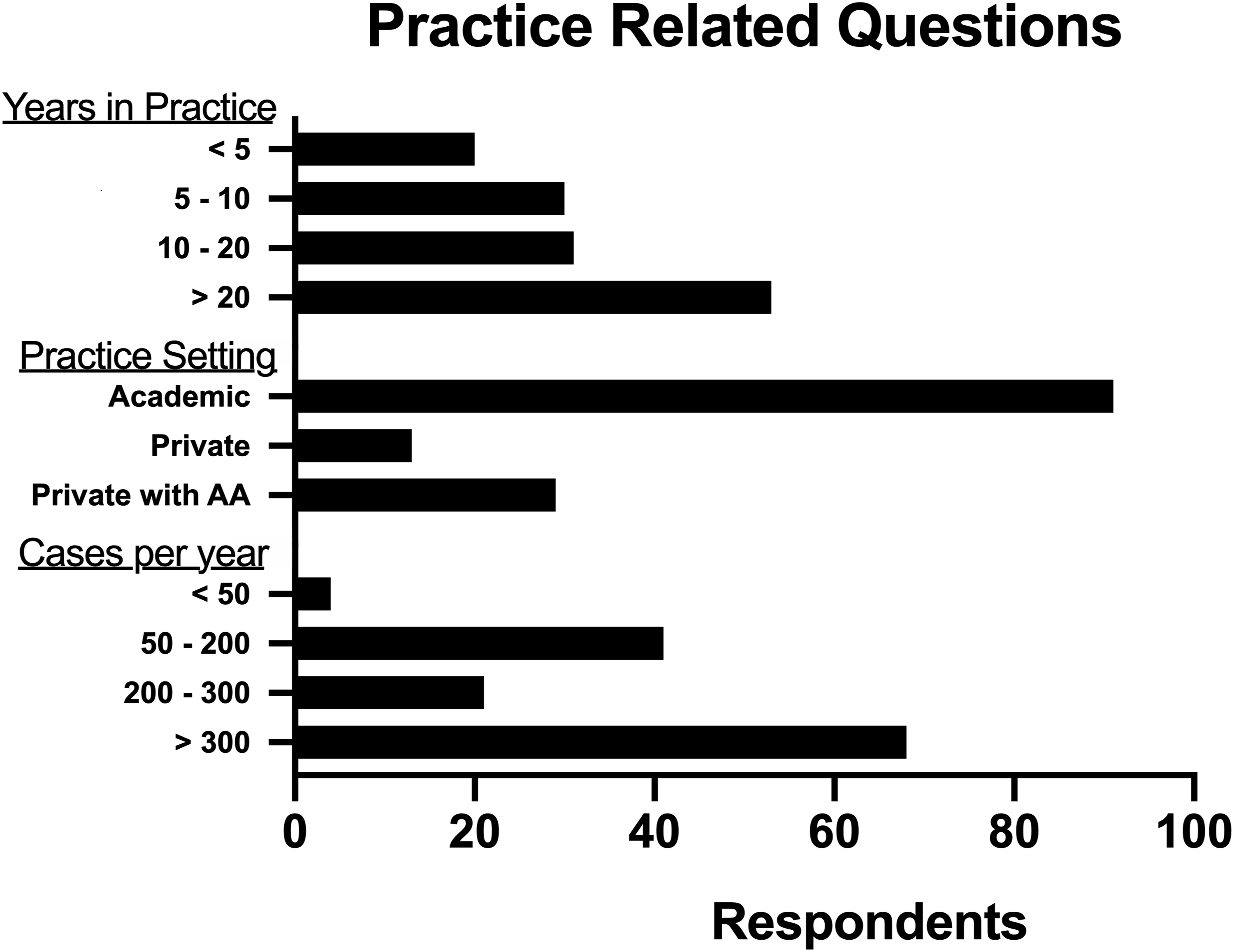
In addition to significant surgeon experience, this group of respondents generally performed a high volume of tonsillectomies. Most reported performing at least 200 tonsillectomies annually (66.4%), with more than half performing more than 300 tonsillectomies, and only 3.0% performing less than 50 per year.
Institutional Policy Versus Physician Preference
Slightly less than half of respondents indicated that their institutions require routine evaluation of tonsillectomy specimens in all patients under the age of 18 years (47.8%) (Figure 2). Out of all respondents who regularly send their tonsillectomy specimens for pathology, 68.3% indicated they do so due to institutional policies or mandates versus 31.7% due to surgeon preference.
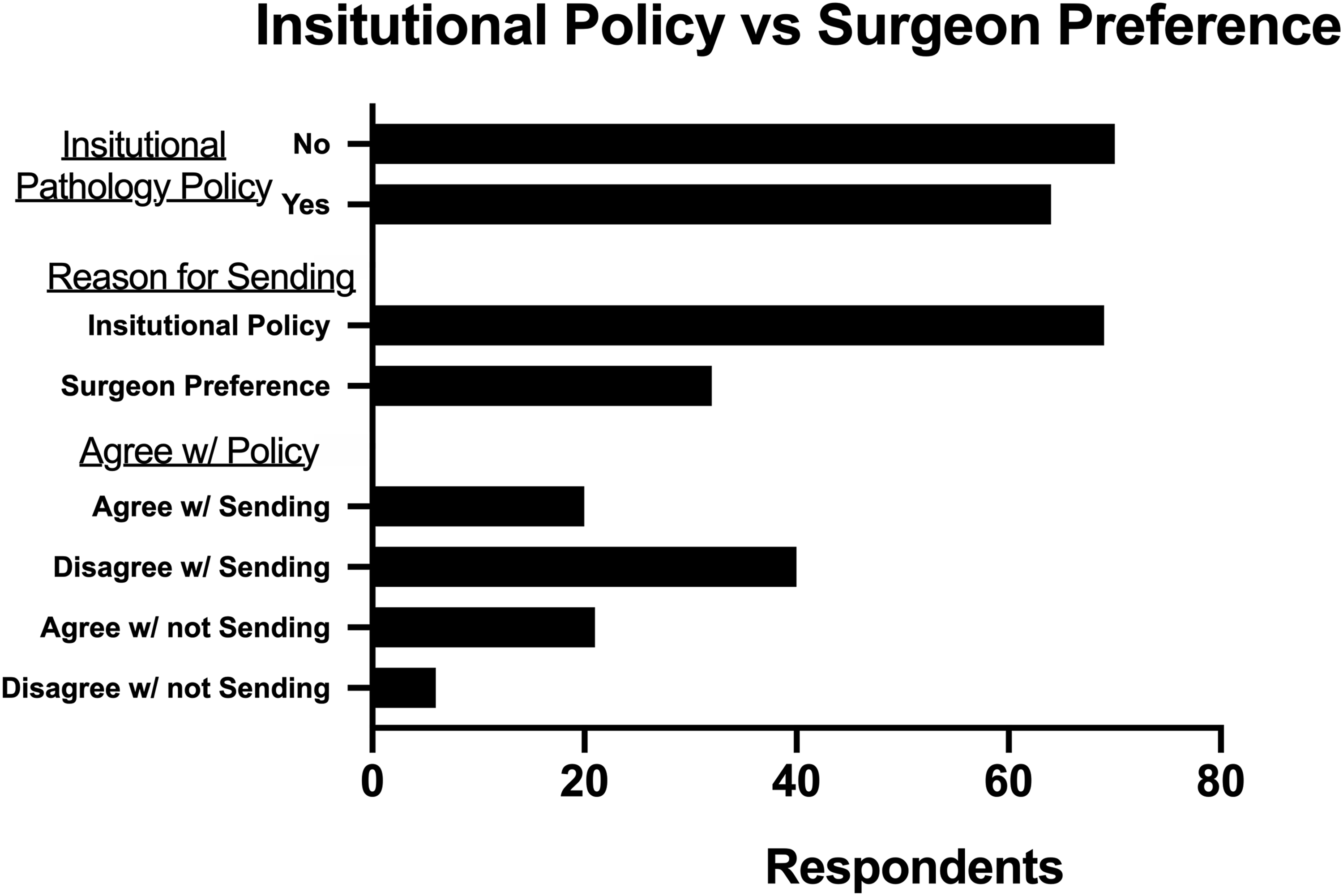
The final question of the survey asked respondents if they agreed or disagreed with their institution’s policies regarding routine pathology. One-third of respondents whose institutions require routine pathologic analysis agree with those guidelines, whereas two-thirds disagreed. The respondents whose institutions do not require routine pathology generally agreed with this policy (91.9%), whereas only 8.1% disagreed with their institutions not requiring routine pathologic analysis.
Approval of Routine Tonsillectomy Pathology
Overall, 85.1% of respondents disapproved of routine pathologic analysis of otherwise uncomplicated tonsillectomy specimens. Most of these respondents were academic otolaryngologists (67.5%), with 10.5% in private practice and 21.1% in private practice with academic affiliation. Out of the 20 (14.9%) who believed routine pathologic analysis should be performed, 14 (70%) worked in academics, 1 (5%) in private practice, and 5 (25%) in private practice with academic affiliation. Additionally, out of those respondents who agreed with routine pathology, 1 reported having seen > 5 previous cases of lymphoma or other unexpected pathology from a routine pediatric tonsillectomy, 2 respondents reported having 3–5 previous cases of unexpected pathology, and 4 respondents had 1–3 previous cases.
When asked to name indications or findings that would trigger a surgeon to order pathologic analysis in a particular patient, most reported tonsillar asymmetry (89.5%) and tonsillar lesion (84.2%) as indications. Less respondents reported neck mass (46.5%), constitutional symptoms (50.0%), and history of head and neck cancer (50.1%) as additional indications.
Centers for Medicare & Medicaid Services Reimbursement Rates for Pathologic Examination of the Tonsils
Query of the CMS reimbursement data showed that, in 2022, Medicare reimbursement for gross-only pathologic tonsillar examination (CPT code 88300) was $15.57, whereas reimbursement for combined gross and microscopic examination (CPT code 88304) was $42.22. Notably, these codes are to be applied twice if the examination is performed separately on both left and right tonsils.
Discussion
This study primarily aimed to gauge practice patterns and institutional policies regarding routine pathologic analysis of pediatric tonsillectomy specimens among ASPO members. Response rate was low, with only 134 members out of 657 responding to the survey (20.4%). Although the study protocol did not permit the demographic analysis of the non-respondent ASPO population, 68.4% of respondents practiced in an academic setting, which is similar to previously reported ASPO demographic data by Preciado et al. in 2009. 11 In addition, survey respondents had a diverse range of experience, with 37.3% of respondents having less than 10 years of experience and 39.6% reporting greater than 20 years of prior experience. In their survey study of ASPO members, Preciado et al. previously reported 67% of respondents in the 36-to-50-year age range and presumably less than 20 years’ experience. This may indicate a slightly more experienced surgeon population in our study, since nearly 40% of respondents reported more than 20 years of prior experience.
Direct costs of pathologic analyses can be difficult to understand in a granular fashion given the complex peculiarities of hospitals and healthcare systems as well as the variability in payment models between different institutions. 12 Therefore, procedural charges in this study were investigated utilizing CMS reimbursement data, as has previously been done by Nelson et al. 12 Current 2022 reimbursement rates of $15.57 for gross-only and $42.22 for combined gross and microscopic pathologic examination are lower than those seen in 2008 reported by Nelson et al., which were $22.85 and $61.32, respectively. It should be emphasized that these costs only represent CMS reimbursement and do not factor into a multitude of institution-level variables, which may include costs to transport or store specimens. Nonetheless, the data gives the tonsillectomy surgeon insight into the economic scale of pathologic tonsillectomy analysis and the potential for healthcare cost savings by forgoing potentially unnecessary analyses.
The trends of utilization of pathologic analysis routinely after tonsillectomy have shifted drastically over time. In 1996, nearly 60% of institutions sent their tonsil specimens for gross and microscopic pathologic examination. 1 By 2001, a follow-up survey revealed that the standard had shifted towards sending tonsil specimens for gross pathologic examination only. 9 More recently, the focus has shifted to investigating whether even routine gross pathologic analysis should be performed. In a recent study, Hobbs et al. examined 3,183 cases of routine tonsillectomy for which gross analysis was performed and found that gross pathologic analysis did not change the management in any of the cases, whether or not they were ultimately sent for microscopic analysis. 2 In another study, 21,223 pediatric routine tonsillectomies that underwent microscopic evaluation were evaluated, and only 3 cases of previously unsuspected malignancies were found, a rate of 0.01%. 13 In the present study, 66.4% of respondents reported performing more than 200 tonsillectomies annually, thus representing a highly experienced sample of surgeons who mostly thought routine pathologic analysis to be unnecessary. The fact that these high-volume surgeons tended not to agree with routine pathology speaks further to firsthand opinions and experiences that support not performing complete pathology on all routine tonsillectomy specimens.
Pediatric otolaryngologists and general otolaryngologists perform the majority of the more than half million annual pediatric adenotonsillectomies, with each provider often performing hundreds yearly. 14 -16 A significant body of literature has grown over time showing the extremely low rate of occult malignancy found in the analysis of routine pediatric tonsillectomy specimens. 1,5 -7,9,10 The largest retrospective study to date on the topic of pathology for tonsillectomy examined over 54,000 patients and found a < 0.1% malignancy rate 7 —however, this study included both adult and pediatric tonsillectomies. In pediatric-only studies, 6 malignancies were seen out of 13,547 patients (0.044%). Given the frequency that these procedures are performed and the relative nonutility of pathologic analysis, it seems prudent to save pathology for those cases which differ from the norm due to suspicious clinical signs and symptoms—nonetheless, institutional policies at many hospital systems require the pathologic analysis of all tonsillectomy specimens, a finding that was corroborated by this study. 8
Cost-effectiveness, healthcare spending, and resource utilization have become subjects of critical importance in the United States in regards to delivering optimal patient care. 17 Unnecessary analysis of routine tonsillectomy specimens can incur significant direct and indirect costs to the healthcare system or hospital, payer, and patient. 8 Several authors have argued against the pathologic analysis of routine pediatric tonsillectomy specimens, citing these substantial costs without clinically recognizable benefit. 5 -8 One retrospective study by Netser et al. examined over 2,700 tonsillectomy specimens and performed a cost–benefit analysis. 17 Their findings overwhelmingly confirmed cost-ineffectiveness of pathologic evaluation in routine cases but cost-effectiveness in non-routine cases. Despite this relatively robust body of literature, it is clear from the results of this study that institutional policies vary significantly across different institutions in the United States, as 47.8% of respondents (n = 64) reported routine pathologic analysis of tonsillectomy specimens by their institution or practice. Furthermore, 29.9% of respondents (n = 40) reported disagreeing with their institution’s policy of sending routine tonsil specimens, signifying an area of disagreement between surgeons and institutional policy. This could potentially be rectified through institutional policy change—however, the authors emphasize that surgeons should always use their best clinical judgment when deciding whether to send tonsillectomy specimens.
It is important to note the distinction between pediatric and adult tonsillectomies, and there is evidence in the adult population arguing in favor of routine pathologic analysis of adult tonsillectomy specimens. 18 One retrospective study of 5,058 patients found significant pathologic findings (defined as an inflammatory process, a benign neoplasm, or an occult malignancy) in 1% of specimens, with no occult malignancies seen in pediatric patients. However, the possibility of occult malignancy cannot be discounted entirely, as some authors have argued in favor of routine pathologic analysis, even in pediatric patients, given the potential benefits of early diagnoses of malignancies like lymphoma. 19
One survey study sent to members of the American Academy of Otolaryngology-Head & Neck Surgery (AAO-HNS) showed a statistically significant decrease over time in the amount of specimens being sent for complete pathologic analysis. 9 However, 80% of respondents in this study were private practice otolaryngologists with only 12% in academics, thereby not representing a similar population to that in this study. Additionally, that study was performed in the 1990s, and similar corroborating data since that time is unavailable. Another single-institution retrospective study by Hobbs et al. determined that gross pathologic analysis of pediatric tonsillectomy specimens did not change clinical management in any cases, while a significant cost savings was seen. 2 These findings support the growing notion that gross evaluation may be an adequate alternative to full histopathologic evaluation, especially in cases without concurrent clinical indications for pathology or concern for malignancy.
When examining specifically the respondents who either agreed with institutional policy to send routine tonsils for pathology or those who did not agree with an institutional policy to not send tonsils, we found that 25 out of 134 (19%) felt this way. Out of those 25 respondents, 20 (80%) agreed with an institutional policy to send specimens, and 5 (20%) disagreed with a policy not to send. Most of these respondents (n = 19, 76.0%) were at academic institutions, 5 with an academic affiliation (20.0%) and 1 in private practice (4.0%). Almost all (n = 22, 88.0%) of this group had been in practice for at least 5 years, with 56% (n = 14) being in practice for at least 10 years. All but one respondent reported performing >50 tonsillectomies per year. Interestingly, the 2 respondents who reported finding abnormal pathology >5 times were included in this group.
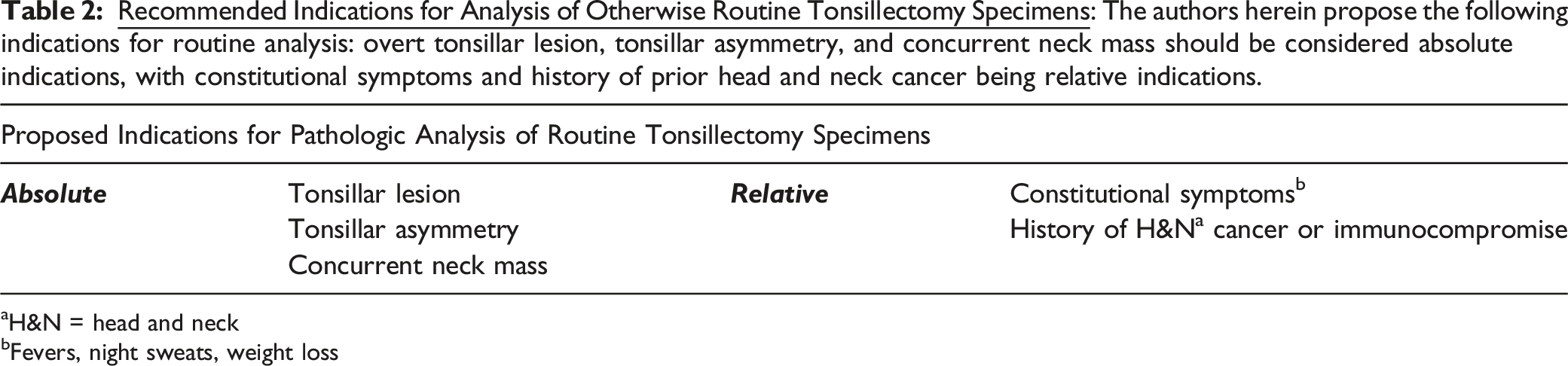
aH&N = head and neck
bFevers, night sweats, weight loss
Weaknesses of this study include the fact that it utilized a non-validated survey, which was vulnerable to opinion-based biases. Another major weakness of this study was a likely selection bias given the low response rate of 20.4%, as certain individuals might be more likely to respond (i.e., academic-based surgeons). Additionally, as this study was only sent to members of ASPO, it preferentially selected those surgeons regularly performing a high volume of tonsillectomies (> 300 per year) and might not be as generalizable to general otolaryngologists. Those surgeons performing the procedure more often could be more likely to respond, thereby not accurately reflecting the practicing pediatric otolaryngology community. Additionally, a larger sample size with a higher response rate would be useful for additional studies. It should be emphasized that these observations and recommendations only apply to pediatric patients, as adult tonsillectomies are known to harbor a significantly high rate of malignancy than pediatric tonsillectomies. 18,19 Nonetheless, these findings suggest the presence of disagreements between surgeon preference and institutional policy at many institutions across the United States. Areas of future research could focus on the medicolegal implications of not performing pathologic analysis that might make institutions more hesitant to stop this practice. Additionally, the role of pathologic analysis within hospital funding models could potentially encourage more testing at these institutions. Further study of these issues could shed light on the reasons behind the persistence of this common practice in the United States and potentially lead to institutional policy changes, thereby reducing overall healthcare costs and overall benefit to the physicians, hospital systems, and, most importantly, patients.
Conclusion
Most respondents to this survey study disapprove of routine pathologic examination of pediatric tonsillectomy specimens in uncomplicated cases. However, many institutions continue to require this practice, suggesting the presence of a discrepancy between institutional policies and surgeon preferences in the pediatric otolaryngology community. The respondents of this survey likely represent a biased sample given the low response rate, and more study would be needed to accurately represent the entire population of pediatric otolaryngologists. However, given the frequency of pediatric adenotonsillectomy among pediatric and general otolaryngologists, healthcare resources could be more appropriately allocated by discontinuation of routine pathologic analysis in lieu of directed examination only when dictated by clinical signs or symptoms. Regardless of institutional policy, individual providers should always use healthcare resources judiciously, and surgical pathology is no exception.
Footnotes
Acknowledgments
The authors acknowledge the American Society of Pediatric Otolaryngology for allowing our survey to be sent via their online system.
Author Contributions
Drafting and editing of manuscript: Rossi, Freeman, Ohlstein
Concept, guidance, and review of manuscript: Pine, Daram, Darling, McKinnon
Author’s Note
This article has not been previously presented nor has it been previously published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
All data in this study was obtained with the guidance and approval of the University of Texas Medical Branch (UTMB) Institutional Review Board (IRB) in Galveston, Texas. Survey responses were obtained with the approval of the American Society of Pediatric Otolaryngology.
Informed Consent
There were no human subjects in this study; therefore, informed consent is not applicable.
Data Availability
Data were obtained under approval of the UTMB IRB and ASPO and were stored in a secured, encrypted location. They can be accessed upon request.