
Abstract
This case study demonstrates a 58-year-old female who contracted COVID-19 post-vaccination presenting with severe left-sided facial pain, headaches, and dyspnea. A computed tomography was ordered and showed acute sinusitis, and upon bedside endoscopy, the patient was shown to have necrosis of the left-sided middle turbinate with no discoloration, palate necrosis, or facial changes. All samples of the necrotic tissue were reported to be invasive fungal sinusitis. The entire turbinate was resected in the operating room and ethmoid, frontal, and maxillary sinuses were healthy. Chest x-rays post-operatively showed pulmonary effusions and edema although the patient was not stable enough for a lung examination to rule out a pulmonary fungal infection. A bedside endoscopy showed no further necrosis post-operatively although a repeat endoscopy showed duskiness at the lateral attachment of the basal lamella right at the most posterior resection of the middle turbinate. The patient was placed on multiple antifungal agents. The patient remained in hypoxemic respiratory failure and septic shock while on pressors and 2 weeks following this, expired. Post–COVID-19 patients have been shown in the literature to have an increased risk of developing invasive fungal sinusitis (IFS) and all IFS cases during active COVID-19 infection have had a 100% mortality rate.
Introduction
Acute invasive fungal sinusitis (AIFS) is a life-threatening fungal infection that incurs significant morbidity and mortality. 1 The relationship between immunosuppression and infection with this disease has been previously described in the literature. Known risk factors include uncontrolled diabetes, ketoacidosis, organ transplant, and hematological malignancies. 2 Timely diagnosis is essential for the initiation of medical or surgical management in this population.
The emergence of COVID-2019 caused a worldwide pandemic, and co-infection with AIFS was described for the first time. 3 The mechanism involves dysregulation of the host’s immune system allowing for infection by opportunistic pathogens. 3 Current literature suggests that COVID-19 infection and treatment with systemic steroids are risk factors for AIFS. 4
While the incidence of AIFS followed by infection with COVID-19 remains unknown, there are only a handful of cases reported in the United States to date.5,6 We present the diagnosis and management for a case of AIFS in a patient who presented at our hospital with facial pain, dyspnea, and headaches following infection with COVID-19.
Case Report
The patient is a 58-year-old female that originally presented to an outside hospital where she was hospitalized for 4 days due to vaccine breakthrough COVID-19 infection.
The patient had a history of hypertension, end-stage renal disease, and a kidney transplant that was complicated by chronic rejection. Two days after being discharged from the outside hospital, she re-presented now with hypoxemia. Her blood oxygen was in the 70 s, and she was placed on a 15-liter nonrebreather and started on antibiotics. During this encounter, she also complained of severe left-sided facial pain, headaches, and dyspnea.
A computed tomography (CT) scan was ordered concerning for left-sided sinusitis and showed acute sinusitis (Figure 1). A bedside endoscopy demonstrated necrosis of the left middle turbinate. Initial visualization showed necrosis along the middle turbinate along the head, black with no facial changes, only pain, no discoloration, and no palate necrosis. Samples of the necrotic tissue were taken, and all came back as invasive fungal sinusitis. Non-contrast Coronal Computed Tomography Sinus. Mucosal thickening is present in the maxillary sinuses bilaterally without evidence of orbital or intracranial extension. Radiological findings correlate with clinical findings of acute sinusitis.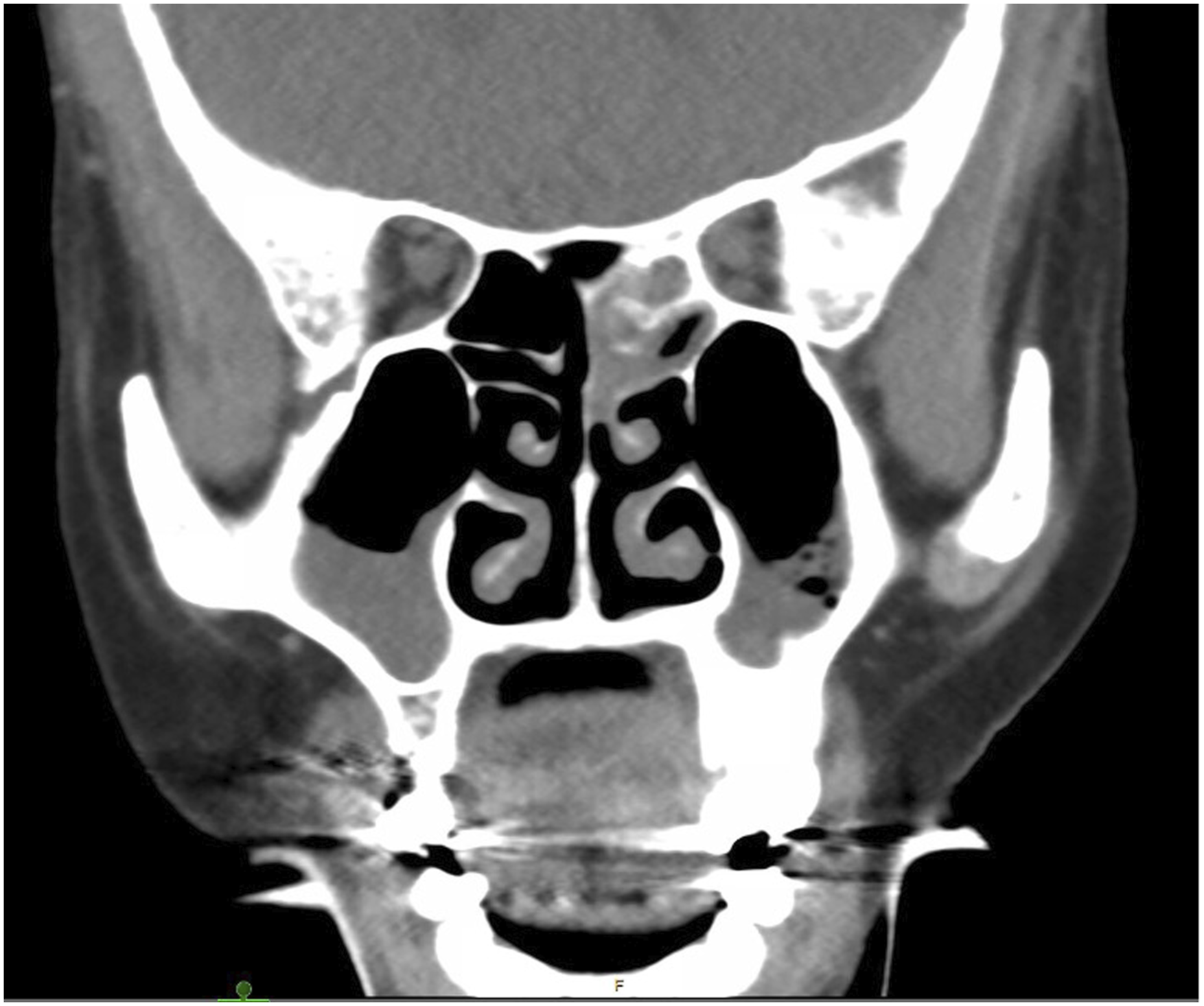
The patient was taken to the OR where it was realized the necrosis was caught relatively early and starting to invade the middle turbinate without evidence of extension to other anatomic sites. The entire turbinate was resected and the ethmoid, maxillary, and frontal sinuses were opened which were found to be healthy.
At the end of the case, we were, unfortunately, unable to wean her off the vent. The patient was transferred to the ICU and subsequently required pressors. Chest X-rays revealed a significant number of pulmonary effusions and edema. Additionally, there was a concern for the presence of invasive fungi in her lungs. Cavitating lesions on lung x-ray and CT scan were seen, although the patient was not stable enough for an examination of the lungs to rule out a pulmonary fungal infection.
Typically, patients that have invasive fungal sinusitis (IFS) are taken for a second look after 2 days to monitor for residual disease. In this case, this was not possible as she was deemed too unstable, she was being prone positioned at this time.
A bedside endoscopy was performed using a flexible bronchoscope to debride the left nasal cavity, further exploration did not show evidence of further necrosis. The IFS portion appeared to be cleared out.
A week later, a repeat endoscopy showed duskiness at the lateral attachment of the basal lamella right at the most posterior site of resection of the middle turbinate, otherwise, all other tissue was healthy. However, she remained too unstable for further surgical intervention in an operating room. Her cultures grew mucor, so she was placed on multiple antifungal agents including amphotericin and isavuconazole (Cresemba).
After 2 weeks, the patient remained in hypoxemic respiratory failure, and septic shock while on 3 pressors. A DNR was declared 2 weeks later, and the patient regrettably expired.
Discussion
A case such as this one is uncommon in the United States but appears to be more common in countries such as India where there have been multiple reports of IFS in the setting of COVID-19, most of which tend to be pulmonary infections. With invasive fungal infections during active COVID-19 infection, there were more than just case reports that are seen in the literature, with all cases having 100% mortality.5,7,8
Mehta et al suspect that the use of steroids, monoclonal antibodies, and broad-spectrum antibodies used to treat COVID-19 may contribute to the development and exacerbation of preexisting fungal infections. 8 Invasive fungal sinusitis has also been shown to be more common in immune-compromised patients, such as those with diabetic, renal, and liver dysfunction.5,9,10
Interestingly, there have been articles published on IFS in patients who recovered from COVID-19. On multivariate analysis, a history of COVID-19 infection was an independent risk factor when controlling for other comorbidities. Longitudinally, patients with a history of infection with COVID-19 experience a 3-fold increased risk of developing IFS, compared to those without. 9
Conclusion
Although the incidence of IFS in patients recovering from or having an active COVID-19 infection has not been established, there has been a noticeable increase in this type of fungal infection specifically in these patients. It is important to monitor patients at risk for fungal disease for clinical signs and symptoms of IFS especially due to the 100% mortality rate as proper diagnosis and management of the fungus may improve rates in the future.8,10
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.