
Abstract
Kaposi’s sarcoma (KS) is a vascular sarcoma derived from vascular endothelial cells and presents with multiple lesions. It mainly appears on the skin and oral mucosa, usually in the face, oral mucosa, and genitals. Very few cases of primary lesions in the nasal cavity have been reported. It is often difficult to diagnose only by imaging examination. Here, we describe a case of KS in a patient who was human immunodeficiency virus (HIV)-negative, in which the primary sites were the nasal mucosa and nasal septum. A diagnosis was made according to the patient’s clinical presentation, physical examination, laboratory examination, imaging examination, and histopathological results. We used surgical resection combined with chemotherapy, with 6 months’ postoperative follow-up without recurrence. We reviewed the relevant literature to identify similar cases and summarize the findings reported on this rare manifestation of KS. We recommend that, where possible, antiviral therapy such as interferon, and regular review should continue, to improve the survival rate and patients’ quality of life.
Introduction
Kaposi’s sarcoma (KS), first reported by scholar Moriz Kaposi in 1872, is a vascular sarcoma derived from vascular endothelial cells and presents with multiple lesions. 1 It mainly appears on the skin and oral mucosa, usually in the face, oral mucosa, and genitals, as multiple painless purple spots. 2 The diseased region can also involve lymph nodes and the viscera. 2 Very few cases of primary lesions in the nasal cavity have been reported.3 -10
Here, we describe a case of KS in a patient who was human immunodeficiency virus (HIV)-negative, in which the primary sites were the nasal mucosa and nasal septum. We reviewed the relevant literature to identify similar cases and summarize the findings reported on this rare manifestation of KS.
Materials and Methods
Case Analysis
A patient with recurrent left nasal bleeding was admitted to the ward from the outpatient otolaryngology department of our tertiary hospital. We recorded the basic data, diagnosis and treatment process, surgical details and follow-up data of the patient in detail.
Literature Review
Additionally, to evaluate the current literature on the diagnosis and treatment of primary KS of the nasal cavity, we searched online databases (PubMed, Web of Science, and National Library of Medicine) from inception through December 2021 for relevant literature, using the search terms ((((Kaposi’s Sarcoma) OR (Kaposis Sarcoma)) OR (Kaposi Sarcoma)) OR (Sarcoma, Kaposi’s) ) AND (((Nasal cavity) OR (Nose)) OR (Head and Neck)). Results were limited to those reported in the English language, describing case reports and case series of patients with KS of the nasal cavity. Patients with primary KS sites outside the nasal cavity and non-English literature were excluded from the analysis. From the selected articles, we extracted the basic information about the patients, the specific part of the nose affected, accompanying diseases, specific types of KS, treatment, and follow-up.
Results
Case Report
Our patient was a 53-year-old Chinese male patient, who was HIV-negative, was not immunosuppressed, and had no history of organ transplantation. The patient was of Zhuang nationality, denied Western European ancestry, and had no travel history in Xinjiang. He had a history of repeated nosebleeds from the left nasal cavity of more than 6 months’ duration, with no obvious cause.
On physical examination, double middle and lower nasal turbinate hypertrophy, right-ward deviation of the nasal septum was noted. In the left nasal cavity, there was a visible tumor with a maximum diameter of 2 cm and a tough texture, which was mainly located in the middle of the nasal septum.
Pathological features of the preoperative left nasal mass included spindle cell hyperplasia, mixed red blood cell, lymphocyte, and plasma cell infiltration around the lesion. A diagnosis of Classic KS (CKS) was considered (Figures 1A and 1B). Immunohistochemistry revealed that the tumor was SMA (-), desmin (-), CD31 (vascular +), CD34 (vascular +), Ki-67 (10% positive rate), S-100 (individual +), D2-40 (focal +), FLT-1 (+), CK-Pan (-), and EMA (-). Combining morphology on hematoxylin‒eosin staining and immunohistochemical phenotype, the lesion was diagnosed as CKS. (A): Histopathology features of biopsy specimen (hematoxylin and eosin stain [HE], ×10); (B): Histopathology features of biopsy specimen (HE, ×40); (C): Postoperative histopathology (HE, ×10); (D): Postoperative histopathology (HE, ×40).
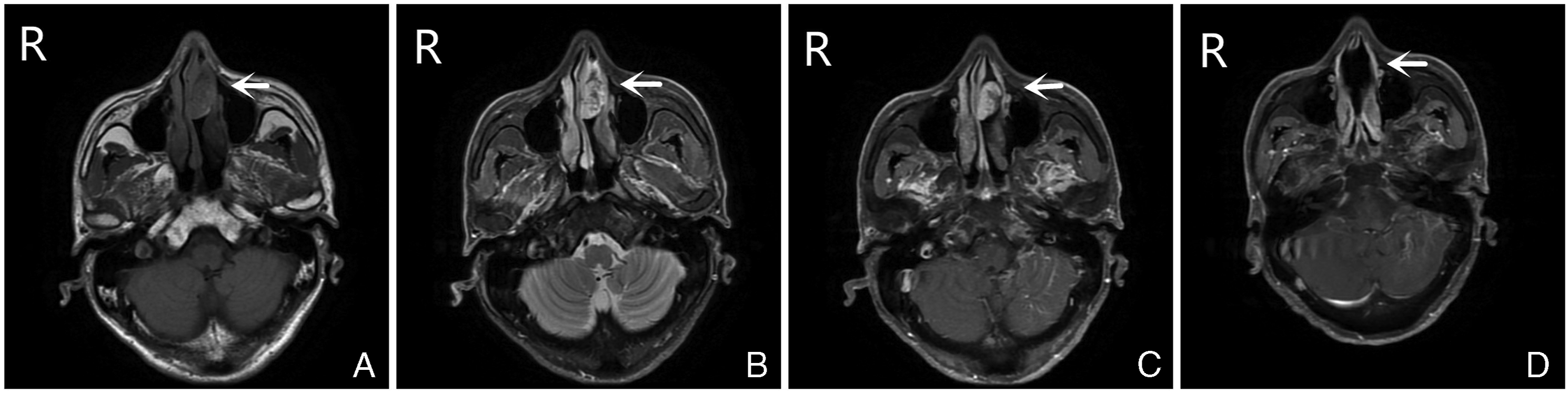
Preoperative nasal endoscopy revealed that the visible mass blocked the left nasal cavity and caused the right-ward nasal septum deviation. Abnormalities in the nasopharynx were absent (Figure 2A). Narrow-band imaging suggested swelling vascular crawling (Figure 2B). Nasopharyngeal magnetic resonance imaging (MRI), and particularly enhanced MRI, showed an abnormal mass signal in the left nasal tract, a uniform hypo- and isointensity signal in T1-weighted imaging, hyper- and hypointensity signal in T2-weighted imaging, and a hypo-intense margin in diffusion-weighted imaging. The lesion measured about 32 mm × 13 mm × 23 mm, and exerted pressure on the left middle and lower turbinate and on the nasal septum. Contrast-enhanced imaging demonstrated that the left nasal tract lesion was significantly uneven, and that the faint signal from the internal plaque did not enhance (Figures 3A‒3C). There was no peripheral lymph node or skin lesions. Hematological examination, liver and spleen ultrasound, and lung computed tomography were normal. (A): Preoperative nasal endoscopy examination; (B): Preoperative narrow band imaging; (C): Postoperative nasal endoscopy examination. (A): Preoperative nasopharyngeal magnetic resonance imaging (MRI), T1-weighted imaging (T1WI); (B): Preoperative MRI, T2WI; (C): Preoperative enhanced MRI, T1WI; (D): Postoperative enhanced MRI, T1WI.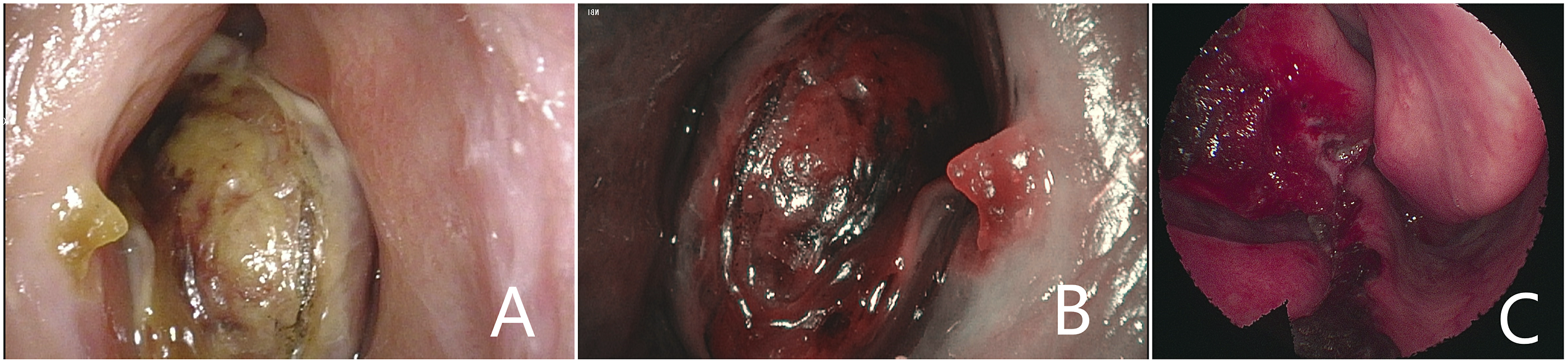
A diagnosis was made according to the patient’s clinical presentation, physical examination, laboratory examination, imaging examination, and histopathological results, because early clinical symptoms of KS are nonspecific and often lead to misdiagnosis or delayed diagnosis. We considered a differential diagnosis of angiosarcoma, squamous cell tumor of the nasal cavity, hemangioma of the nasal cavity, and nasal inverted papilloma. The whole tumor, part of the nasal septum cartilage, and part of the ethmoid vertical plate were resected under nasal endoscopy and general anesthesia. Rapid frozen pathological examination of the tumor margin was negative.
Postoperative symptomatic and supportive treatment, such as anti-inflammation and hemostasis, was provided. Two weeks post-operatively, three courses of chemotherapy (doxorubicin liposome 30mg iv drip d1, q3w plan) were administered. The patient was regularly followed-up on an outpatient basis. Interferon antiviral therapy was rejected for economic reasons.
Postoperative left nasal tumor histopathology revealed spindle cell proliferation, an irregular fissured lumen, and erythrocyte extravasation, typical of CKS (Figures 1C and 1D). Postoperative nasal endoscopy showed unobstructed bilateral nasal cavities, a partially resected nasal septum. The left nasal cavity was free of the tumor mass, and the postoperative wound was visible (Figure 2C). At the 3-month follow-up visit, the patient showed good recovery. Plain and enhanced MRI of the nasopharynx at this visit confirmed partial absence of the nasal septum, nasopharyngeal cavity symmetry, the opening of the Eustachian tube, symmetrical pharyngeal recess, no abnormal signal, and no skull base bone abnormalities (Figure 3D). Blood test results were not significantly abnormal. At present, after 6 months, the CKS in the nasal cavity has not recurred.
Literature Review
Literature Review of English-Language Reported Cases of primary Kaposi’s Sarcoma of the Nasal Cavity.

M, male; F, female; ND, not documented.
Gnnep et al discussed nine cases of KS in the head and neck, including one case in an HIV-negative individual, which was treated surgically and recurred at 9 months. 10 Venizelos et al also reported a case of nasal KS in a patient with an adequate immune system. 3 Their patient was a 59-year-old female who underwent left nasal septum resection. The patient did not undergo further treatment, and was in a good condition 4 years later. 3 A further HIV-negative case of KS in the nasal cavity was described by Mouden et al 4 This was a 56-year-old woman who was treated with chemotherapy alone, resulting in excellent local control over 12 months. 4 Huang et al reported two HIV-negative cases, which were treated by surgical resection and surgical resection combined with radiotherapy, respectively, but did not mention their prognosis.
The six previously reported HIV-positive patients with nasal KS underwent surgical resection. One case recurred at 2 months, 5 while another had not recurred by 5 months. 9 Recurrence was not mentioned in the four other cases.6,7
Discussion
At present, the etiology of KS is not clear. It is considered to be the result of the interaction of genetic, 11 immune, cytokine, endocrine, racial, and environmental factors. 12 KS has been associated with HHV-8 virus infection.12,13 While oral and craniofacial involvement is common in HIV-positive patients, head and neck KS is rare in HIV-negative patients (< 5% of KS cases). 14 The most usual manifestation of KS in HIV-negative patients is bilateral lower limb lesions. 15 In head and neck KS, the incidence of nasal cavity involvement is markedly lower; thus, it should be considered as an obvious manifestation. The presence of primary KS of the nasal cavity with atypical manifestation in individuals with normal immune function is a very rare finding. 16
According to its clinical characteristics, KS is roughly divided into four different types: classic, endemic, iatrogenic, and acquired immunodeficiency syndrome (AIDS)-associated KS. 17 Among them, CKS patients are more prevalent in individuals of Western European descent, more common in China’s Xinjiang region, males, and those aged 50‒70 years. Paultrikidou et al observed 251 patients with head and neck KS, and found that the hard palate and oropharynx were often affected. 18 In our case of CKS, the patient was HIV-negative, had not undergone transplantation, had no history of travel within Africa or Xinjiang.
Kaposi’s sarcoma can be divided into a patch stage, plaque stage, and nodular stage according to differences in histopathology. 17 In the patch stage, the epidermis is flat, and the lesions are mainly located in the dermis. Some irregular vascular proliferation, with small attachment structure and chronic inflammation is observed around the normal tissue, but some endothelial cells are observed; thus, the tissue structure is similar to the normal structure. 19 In the plaque stage, lesions accumulate in the dermal and subcutaneous tissues. In this stage, the skin becomes slightly elevated, and the proliferated blood vessels progress into the subcutaneous tissue. Vascular endothelial cells are visible, and spindle cells begin to appear. The stroma also contains numerous macrophages with a high hemosiderin content. 19 Typical pathological manifestations can be observed in the nodular stage. A large number of flaky, fused spindle cell foci, with fissure-like vascular cavities containing red blood cells, appear. Chronic inflammatory infiltration by lymphocytes, plasma cells, and dendritic cells can be seen in the stroma. Immunohistochemistry reveals expression of CD31, CD34, and vimentin in the spindle-shaped tumor cells. In the present case, the pathological examination showed spindle cells, red blood cells, and inflammatory cell infiltration. Immunohistochemically, CD31 (blood vessel +) and CD34 (blood vessel +) staining was consistent with a pathological diagnosis of CKS, and histology indicated that it was at the nodular stage. Pathological examination is often needed to differentiate CKS from angiosarcoma, fibrosarcoma, and suppurative granuloma.
The treatment of KS mainly includes surgery, radiotherapy, chemotherapy, and antiviral therapy. The treatment goal is to relieve symptoms, prevent disease progression, and alleviate organ involvement and psychological stress. 20 Single localized lesions can be treated by surgery, and extensive lesions can be treated by radiotherapy. 21 The condition can also be treated with systemic chemotherapy. It has been reported that paclitaxel combined with antiretroviral therapy has marked therapeutic effects on AIDS-related KS, 22 while gemcitabine has some effects on the treatment of KS. 23 In addition, interferon therapy has a significant effect on CKS. 19 For HIV-positive patients, it is recommended that highly active antiretroviral therapy be included. 19 In this case, the patient was diagnosed with CKS by biopsy after enhanced MRI excluded hemangioma before the operation. The nodular lesion was limited to the left nasal cavity. Thus, we undertook complete endoscopic resection of the tumor and part of the nasal septum cartilage, part of the vertical plate of the ethmoid bone. Intraoperatively, the rapid frozen pathology of the resected tumor revealed a negative margin. Postoperatively, the patient received symptomatic and supportive treatment and three courses of liposomal doxorubicin chemotherapy at 2 weeks after surgery, with regular outpatient re-evaluation. As CKS is accompanied by non-Hodgkin’s lymphoma in some patients, and as some secondary cancers are also common in the first 2 years after CKS diagnosis, it is necessary to follow-up CKS patients. 24
Conclusions
Primary KS of the nasal cavity is a very infrequent disease. The case we reported here was only the sixth case of CKS in an HIV-negative individual. Otolaryngologists should be acquainted with the characteristics of this disease, and should not omit histopathological and laboratory examination, in order to avoid misdiagnosis or missing the diagnosis, which would result in delayed treatment of the disease. In our case, we used surgical resection combined with chemotherapy, with 6 months’ postoperative follow-up without recurrence. We recommend that, where possible, antiviral therapy such as interferon, and regular review should continue, to improve the survival rate and patients’ quality of life.
Footnotes
Authors’ Note
The case report section of this manuscript has been accepted by the Chinese Medical Case Repository (CMCR) organized by the China Association for Science and Technology in Beijing, China, March, 2022. That case repository supports and encourages authors to submit articles to other relevant academic journals after publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was supported by 2018 Guangxi Higher Education undergraduate Teaching Reform Project. (NO: 2018JGB269). This paper was funded by Baise Scientific Research and Technology Development Plan Project. (NO: 20213718).
Consent
The patient gave written informed consent for the publication of the case report and related images.